Direct Lateral Hip: Optimize Exposure with Sharp Curved Hohmann
Key Takeaway
Learn more about Direct Lateral Hip: Optimize Exposure with Sharp Curved Hohmann and how to manage it. The direct lateral approach to the hip is indicated for primary and revision total hip replacement, especially for advanced arthritis or femoral neck fractures. This surgical method involves careful splitting of the gluteus medius muscle, protecting the superior gluteal nerve. Imaging like radiographs and sometimes CT/MRI precede the procedure. Tools such as a **sharp curved hohmann** retractor are crucial for achieving optimal surgical exposure.
Introduction and Epidemiology
The direct lateral approach to the hip, popularized by Hardinge in 1982, remains a foundational surgical exposure in modern orthopedic surgery. This approach provides excellent visualization of both the acetabulum and the proximal femur while maintaining a significantly lower dislocation rate compared to traditional posterior approaches. The direct lateral approach is widely utilized for primary total hip arthroplasty, revision arthroplasty, and the management of proximal femoral fractures. By directly splitting the gluteus medius and vastus lateralis, the surgeon gains direct access to the hip joint without the need for posterior soft tissue release, thereby preserving the posterior capsular structures that are critical for preventing posterior instability.

Epidemiologically, the direct lateral approach is one of the most frequently utilized surgical exposures for hip arthroplasty globally, particularly in European registries, although the posterior and direct anterior approaches have seen increased utilization in North America. The enduring popularity of the lateral approach is attributed to its reproducible anatomy, extensile nature, and the inherent stability it provides to the prosthetic joint. However, the approach is not without its controversies, primarily centering around the potential for postoperative abductor weakness and the development of a Trendelenburg gait if the abductor mechanism is not meticulously repaired or if the superior gluteal nerve is compromised during the proximal split.


Mastery of this approach requires a profound understanding of the abductor footprint, the course of the superior gluteal nerve, and the strategic use of retractors. Specifically, optimizing acetabular exposure relies heavily on the strategic placement of a sharp curved Hohmann retractor over the anterior acetabular rim. This maneuver safely retracts the anterior capsular structures and the split abductor mass, providing an unimpeded view of the acetabulum for precise reaming and component seating.

Surgical Anatomy and Biomechanics
Osseous Structures
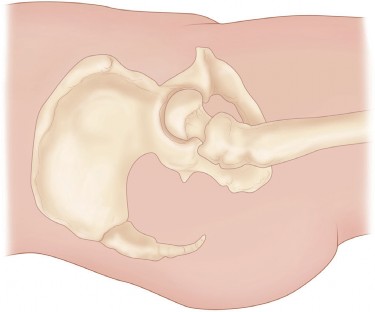
The osseous anatomy relevant to the direct lateral approach includes the greater trochanter, the femoral neck, the acetabulum, and the anterior inferior iliac spine. The greater trochanter serves as the critical landmark for both the skin incision and the deep fascial dissection. It is the insertion site for the gluteus medius (lateral and superoposterior facets) and the gluteus minimus (anterior facet). Understanding the exact footprint of these tendons is essential for a precise split and subsequent repair. The acetabulum is oriented with varying degrees of anteversion and inclination, which must be visualized clearly after capsulotomy to ensure accurate component positioning.

Musculotendinous Units
The direct lateral approach does not utilize a true internervous plane. Instead, it involves an intermuscular split through the gluteus medius and the vastus lateralis. The gluteus medius and minimus are innervated by the superior gluteal nerve, while the vastus lateralis is innervated by the femoral nerve. The approach elevates the anterior portion of the gluteus medius and minimus in continuity with the vastus lateralis, creating an anterior flap. The gluteus maximus is split bluntly in line with its fibers during the superficial dissection. The preservation of the posterior half of the gluteus medius is vital for maintaining pelvic stability during the single-leg stance phase of gait.


Neurovascular Anatomy
The most critical neurovascular structure at risk during the direct lateral approach is the superior gluteal nerve. This nerve exits the greater sciatic foramen, courses between the gluteus medius and minimus, and supplies both muscles as well as the tensor fasciae latae. Anatomical studies demonstrate that the main branch of the superior gluteal nerve crosses the ilium approximately 3 to 5 centimeters proximal to the tip of the greater trochanter. Therefore, the proximal split of the gluteus medius must not extend beyond 3 centimeters proximal to the greater trochanter to avoid denervating the anterior portion of the abductor muscle complex. The primary blood supply encountered includes branches of the lateral femoral circumflex artery, particularly the ascending branch, which must be identified and coagulated within the vastus lateralis split.

Indications and Contraindications
The direct lateral approach is highly versatile and is indicated for a wide spectrum of hip pathologies. It is classically used for primary total hip replacement in patients with advanced osteoarthritis, rheumatoid arthritis, or post-traumatic arthritis. It is also an excellent choice for patients with a displaced femoral neck fracture requiring either hemiarthroplasty or total hip arthroplasty. The approach provides sufficient exposure for complex primary cases, including developmental dysplasia of the hip, where the anatomy may be distorted. Furthermore, the direct lateral approach is frequently utilized for revision total hip replacement surgery, as it can be easily extended proximally into the ilium or distally along the femoral shaft for extensile exposure.

Contraindications are relatively few but must be carefully considered. It may be relatively contraindicated in patients with profound pre-existing abductor deficiency, as further surgical trauma to the gluteus medius could result in an intractable Trendelenburg gait. Additionally, cases requiring extensive exposure of the posterior column of the acetabulum for complex fracture fixation or specific revision scenarios may be better served by a posterior or extensile posterior approach.


| Pathology | Operative Indications for Lateral Approach | Non-Operative Management |
|---|---|---|
| Advanced Osteoarthritis | Intractable pain, functional limitation, failure of conservative therapy | NSAIDs, physical therapy, intra-articular injections, weight loss |
| Displaced Femoral Neck Fracture | Garden III/IV fractures in elderly, independent ambulators | High surgical risk patients (comfort care), extremely limited life expectancy |
| Revision Arthroplasty | Aseptic loosening, instability, component malposition, infection (staged) | Stable asymptomatic radiolucencies, prohibitive medical comorbidities |
| Developmental Dysplasia | Severe secondary arthritis, subluxation requiring structural grafting | Mild dysplasia without significant joint space narrowing or pain |
| Avascular Necrosis | Collapse of femoral head (Ficat Stage III/IV) with secondary arthritis | Pre-collapse stages (Core decompression, bisphosphonates, restricted weight-bearing) |


Pre Operative Planning and Patient Positioning
Clinical Examination and Imaging
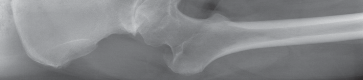
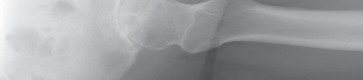
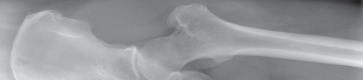
Thorough preoperative evaluation is mandatory. Plain radiographs remain the cornerstone of preoperative planning. An anteroposterior (AP) pelvis radiograph, along with AP and lateral radiographs of the affected hip, are highly recommended. These images allow for the assessment of bone quality, joint space narrowing, osteophyte formation, and the presence of subchondral cysts.


Surgeons must strictly template the radiographs to determine optimal component size and precise component position. The primary goals of templating are the restoration of the anatomic center of rotation, the reproduction of native leg length, and the re-establishment of femoral offset. Failure to restore offset can lead to abductor laxity, increasing the risk of instability and gait abnormalities. Occasionally, advanced imaging such as a computed tomography (CT) scan or magnetic resonance imaging (MRI) is indicated. These modalities are particularly useful to assess severe acetabular bone loss, large subchondral cysts, and complex three-dimensional deformity in developmental dysplasia during primary or revision total hip replacement.
Patient Positioning and Preparation
The patient is typically placed in the lateral decubitus position, although the supine position can also be utilized depending on surgeon preference. In the lateral decubitus position, the patient is secured using a peg board or a vacuum bean bag system. The pelvis must be strictly orthogonal to the floor to ensure that intraoperative assessment of acetabular cup version and inclination is accurate.


The dependent leg is padded and slightly flexed at the knee to relax the sciatic nerve and provide stability. The operative leg is prepped and draped free to allow for full manipulation during dislocation, trial reduction, and assessment of impingement and stability. Bony landmarks, including the anterior superior iliac spine, the greater trochanter, and the femoral shaft axis, are palpated and marked prior to incision.
Detailed Surgical Approach and Technique
Superficial Dissection
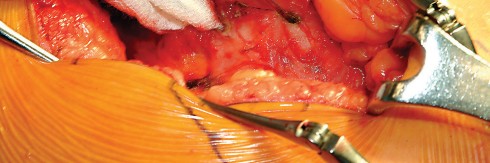
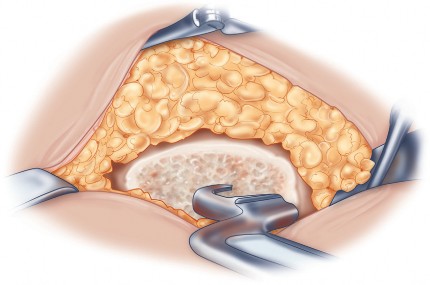
The skin incision is centered over the greater trochanter. It extends proximally, curving slightly posterior to the tip of the trochanter, and distally along the axis of the femoral shaft. Subcutaneous tissues are incised in line with the skin incision down to the fascia lata. The fascia lata is then incised sharply over the center of the greater trochanter. Proximally, this fascial incision splits the gluteus maximus in line with its muscle fibers. Distally, it splits the iliotibial band. Charnley retractors are often placed at this stage to hold the fascial flaps apart, exposing the underlying vastus lateralis distally and the gluteus medius proximally.
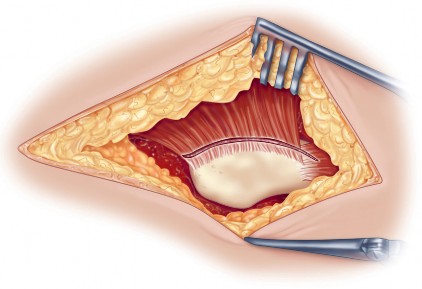
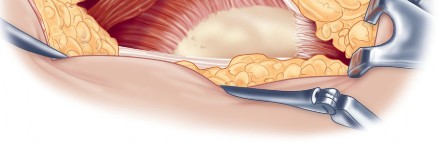
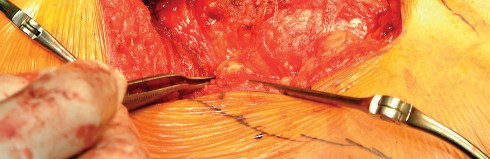
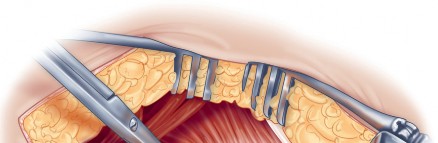
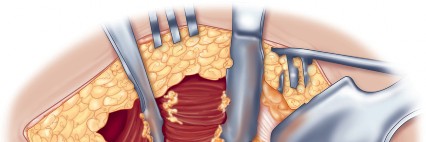
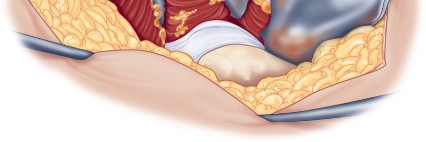
Deep Dissection and Abductor Splitting
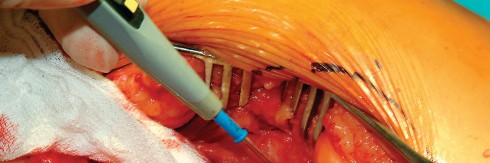
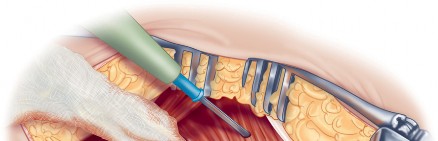
The deep dissection is the defining step of the Hardinge approach. The anterior third of the gluteus medius is identified. A split is made in the gluteus medius starting from the apex of the greater trochanter and extending proximally for no more than 3 to 5 centimeters to protect the superior gluteal nerve. This split is carried distally into the vastus lateralis, leaving a cuff of tendon attached to the greater trochanter to facilitate robust closure.

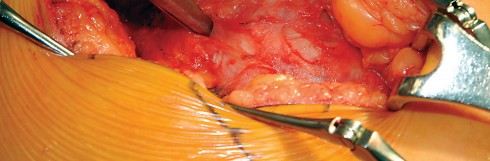
The anterior flap, consisting of the anterior portion of the gluteus medius, the underlying gluteus minimus, and the proximal vastus lateralis, is elevated off the anterior capsule using electrocautery or an osteotome. During the elevation of the vastus lateralis, branches of the lateral femoral circumflex artery are consistently encountered and must be meticulously ligated or cauterized to prevent postoperative hematoma.


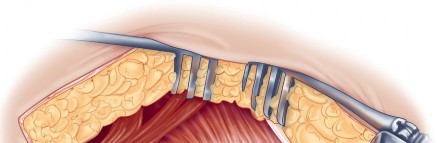
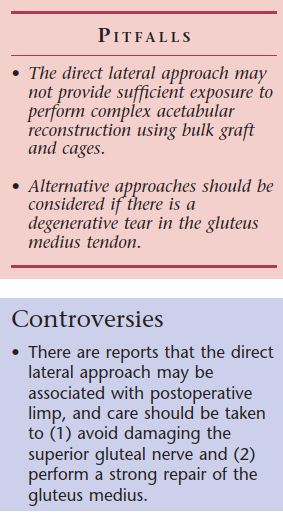
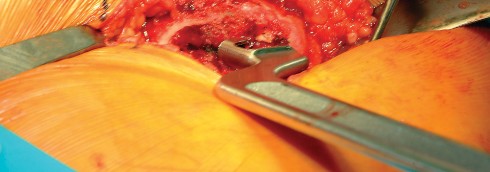
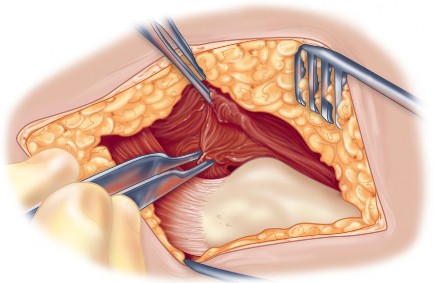
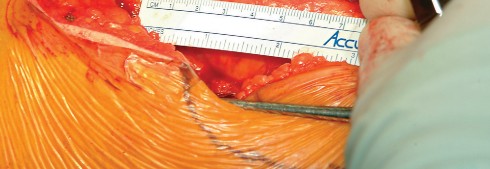
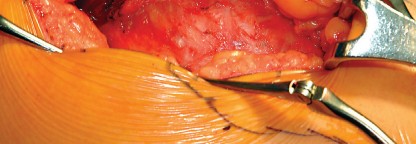
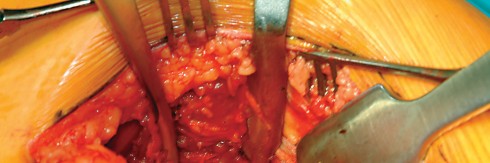
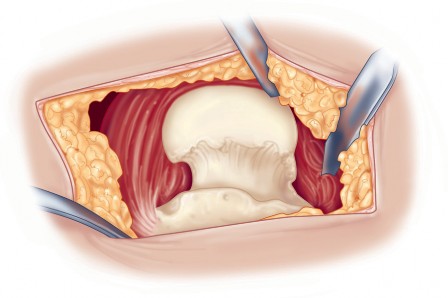
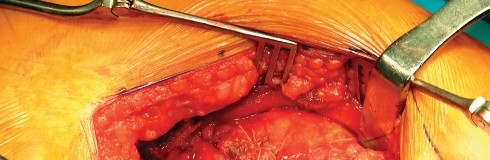
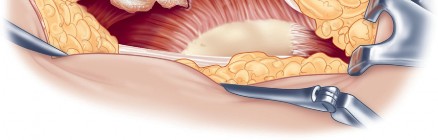
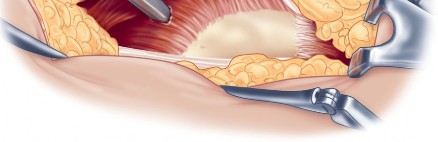
Optimizing Exposure with the Sharp Curved Hohmann
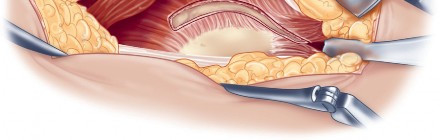
Once the anterior capsular exposure is achieved, a T-shaped or H-shaped capsulotomy is performed. The hip is then dislocated anteriorly with external rotation, extension, and adduction. After the femoral neck osteotomy is completed and the femoral head is removed, attention turns to acetabular preparation.


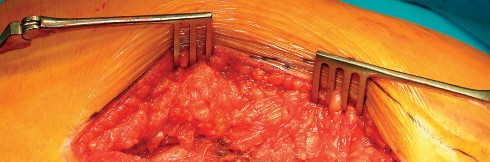
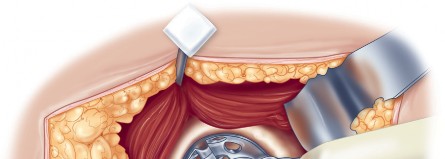
Acetabular exposure is the most technically demanding aspect of the lateral approach. To optimize exposure, the strategic placement of retractors is paramount. A sharp curved Hohmann retractor is carefully placed over the anterior lip of the acetabulum. The sharp tip must engage the bone securely to prevent slippage. This retractor serves a dual purpose: it retracts the anterior capsule and the elevated abductor-vastus flap anteriorly, providing unimpeded visualization of the anterior and superior acetabular rim.

Additional retractors are utilized to complete the exposure. A blunt Hohmann or Cobra retractor is placed inferiorly beneath the transverse acetabular ligament to retract the inferior capsule and soft tissues. A third retractor may be placed posteriorly. The precise placement of the anterior sharp curved Hohmann is the key to preventing the abductor mass from obscuring the surgeon's view during reaming and cup impaction.
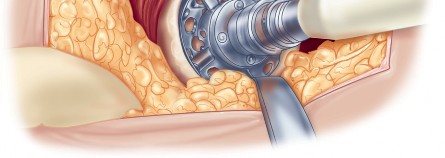
Component Preparation and Implantation
With the acetabulum fully exposed, the labrum is excised, and osteophytes are removed to identify the true floor of the acetabulum (cotyloid fossa). Sequential reaming is performed until punctate bleeding from subchondral bone is achieved. The acetabular component is then impacted into place, targeting approximately 40 to 45 degrees of inclination and 15 to 20 degrees of anteversion.
Following acetabular fixation, the femur is elevated and externally rotated for preparation. A box chisel is used to open the femoral canal laterally, ensuring neutral alignment to avoid varus malpositioning of the stem. Sequential broaching is performed until rotational stability is achieved. Trial components are placed, and the hip is reduced to assess leg length, offset, and stability through a full range of motion. Once satisfied, the definitive femoral stem and head are implanted.
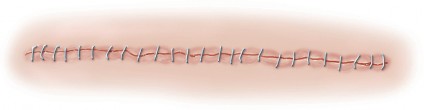
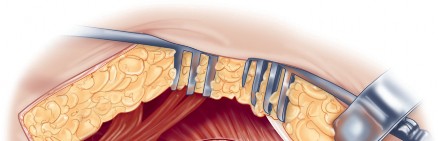
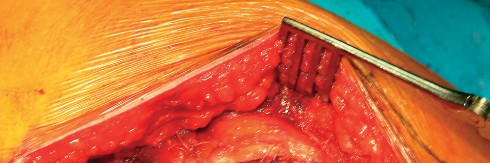
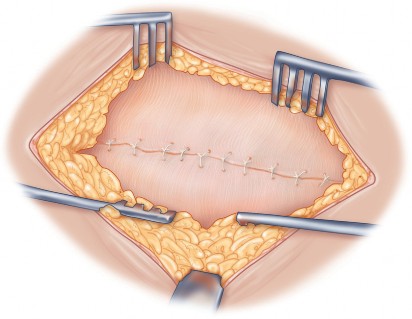
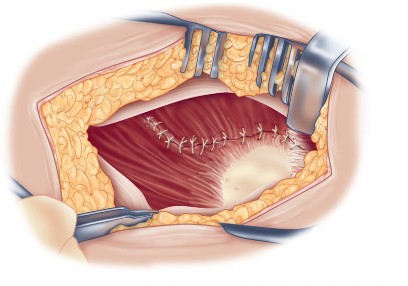
Meticulous Closure
Closure is a critical phase of the direct lateral approach. The anterior flap of the gluteus medius and vastus lateralis must be securely repaired to the posterior cuff of the tendon left on the greater trochanter. Heavy non-absorbable sutures or strong absorbable sutures (e.g., #2 or #5) are utilized. Some surgeons prefer transosseous tunnels through the greater trochanter to ensure a robust repair. Failure to achieve a secure closure can lead to abductor avulsion, resulting in a persistent Trendelenburg gait and lateral hip pain. The fascia lata is closed meticulously to prevent fascial herniation, followed by standard subcutaneous and skin closure.

Complications and Management
While the direct lateral approach is highly reliable, it carries specific risks that the orthopedic surgeon must anticipate and manage. The most frequently discussed complication is abductor weakness. This can result from direct injury to the superior gluteal nerve if the proximal split exceeds 5 centimeters, or from mechanical failure of the abductor repair at the greater trochanter. Patients present with a characteristic Trendelenburg lurch.


Heterotopic ossification (HO) is statistically more common in the direct lateral approach compared to the posterior approach, likely due to the extensive muscle trauma within the abductor mass. Prophylaxis with non-steroidal anti-inflammatory drugs (NSAIDs) or localized radiation is recommended in high-risk patients. Dislocation, while less common than in the posterior approach, can still occur, typically in an anterior direction if the components are excessively anteverted or if the anterior capsular repair fails.


| Complication | Estimated Incidence | Prevention and Salvage Strategies |
|---|---|---|
| Abductor Weakness / Trendelenburg Gait | 4% - 12% | Prevention: Limit proximal split to <3-5 cm, meticulous transosseous repair. Salvage: Physical therapy, cane use, rarely gluteus maximus transfer. |
| Heterotopic Ossification | 15% - 30% (mostly asymptomatic) | Prevention: Meticulous hemostasis, NSAID prophylaxis (Indomethacin), single-dose radiation. Salvage: Surgical excision if mature and causing severe restriction. |
| Superior Gluteal Nerve Injury | 1% - 3% | Prevention: Respect the 3-5 cm safe zone proximal to the greater trochanter. Salvage: Compensation therapy, bracing. |
Clinical & Radiographic Imaging





You Might Also Like

