Operative Management of Clavicle Fractures: A Comprehensive Surgical Guide
Key Takeaway
Clavicle fractures are among the most common orthopedic injuries. While historically managed nonoperatively, modern evidence demonstrates superior union rates and functional outcomes with open reduction and internal fixation (ORIF) for displaced fractures. This comprehensive guide details the evolving treatment paradigms, biomechanical considerations, precise surgical approaches, and postoperative rehabilitation protocols essential for optimizing patient outcomes and minimizing complications such as nonunion and malunion.
INTRODUCTION AND HISTORICAL PERSPECTIVE
The clavicle is one of the most frequently fractured bones in the human body, accounting for approximately 2.6% to 4% of all adult fractures and up to 44% of all shoulder girdle injuries. The mechanism of injury most often involves a direct blow to the lateral aspect of the shoulder or, less commonly, a fall on an outstretched hand (FOOSH) that transmits axial loads through the upper extremity to the shoulder girdle.
Historically, the prevailing orthopedic dogma dictated that the vast majority of clavicular fractures would heal uneventfully without serious consequences when managed with nonoperative treatment (e.g., figure-of-eight brace or simple sling). The resulting bony prominences and cosmetic deformities were widely believed to be preferable to the unsightly surgical scars and potential complications associated with open reduction and internal fixation (ORIF).
This conservative treatment paradigm was heavily influenced by the landmark epidemiological studies of Neer and Rowe in the 1960s. Their two large series demonstrated nonunion rates of less than 1% in conservatively managed midshaft fractures, compared with nearly 4% in operatively treated fractures. For decades, these results established the foundational concept that union rates and functional outcomes were excellent with conservative treatment and generally superior to operative intervention.
The Modern Paradigm Shift
More recent, high-quality prospective studies and meta-analyses have fundamentally challenged the historical reliance on conservative management, particularly regarding union rates, functional recovery, and the morbidity associated with symptomatic malunions.
A pivotal prospective observational study evaluating 868 patients with clavicular fractures treated nonoperatively revealed an overall nonunion rate of 6.2%. Furthermore, this study identified critical independent risk factors for nonunion, including:
* Advanced age
* Female sex
* 100% displacement (complete lack of cortical contact)
* Presence of severe comminution
Further solidifying the shift toward operative intervention for specific fracture patterns, a comprehensive meta-analysis encompassing 2,144 fractures demonstrated a nonunion rate of 15% for displaced clavicular fractures treated nonoperatively. In stark contrast, the nonunion rate for comparable displaced fractures managed with ORIF was only 2%. Consequently, the contemporary orthopedic consensus strongly supports surgical stabilization for displaced midshaft clavicle fractures to optimize functional outcomes, accelerate return to activity, and significantly reduce the incidence of nonunion and symptomatic malunion.
SURGICAL ANATOMY AND BIOMECHANICS
A profound understanding of clavicular anatomy and the deforming muscular forces is essential for achieving anatomic reduction and stable fixation.
Osteology
The clavicle is an S-shaped tubular bone that acts as the sole osseous strut connecting the axial skeleton (sternum) to the appendicular skeleton (scapula/acromion).
* Medial Two-Thirds: Convex anteriorly, tubular in cross-section, and provides a robust medullary canal.
* Lateral One-Third: Concave anteriorly, flattened superior-inferiorly, and lacks a defined medullary canal.
The junction between the tubular medial segment and the flattened lateral segment represents a biomechanical weak point, explaining why approximately 80% of all clavicle fractures occur in the middle third (diaphysis).
Deforming Muscular Forces
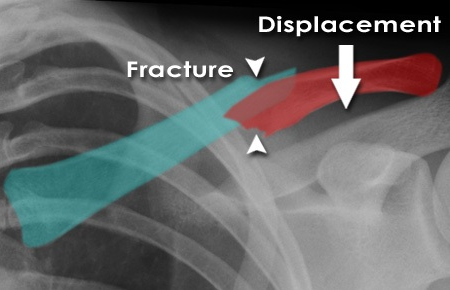
When a midshaft clavicle fracture occurs, predictable displacement patterns arise due to the unopposed pull of attached musculature:
1. Medial Fragment: Displaced superiorly and posteriorly by the strong pull of the sternocleidomastoid (SCM) muscle.
2. Lateral Fragment: Displaced inferiorly and medially. The weight of the arm and the pull of the deltoid drive the fragment inferiorly, while the pectoralis major and latissimus dorsi pull the shoulder girdle medially, resulting in fracture shortening and overriding.
Clinical Pearl: The degree of initial shortening is a critical prognostic indicator. Shortening greater than 1.5 to 2.0 cm alters the resting tension of the shoulder girdle musculature, leading to altered scapulothoracic kinematics, decreased shoulder endurance, and a higher risk of symptomatic malunion if treated nonoperatively.
Neurovascular Proximity
The clavicle serves as a protective shield for the underlying neurovascular bundle. The subclavian artery, subclavian vein, and the cords of the brachial plexus pass directly posterior and inferior to the middle third of the clavicle.
Surgical Warning: The distance between the posterior cortex of the clavicle and the subclavian vein can be as little as 10 to 15 mm. Plunging with a drill bit, over-penetration with a depth gauge, or using excessively long screws in this region can result in catastrophic, life-threatening hemorrhage or permanent neurologic deficit.
INDICATIONS FOR OPERATIVE MANAGEMENT
The decision to proceed with ORIF must be individualized, weighing the fracture pattern against patient-specific factors such as age, activity level, and medical comorbidities.
Absolute Indications
- Open fractures.
- Fractures associated with neurovascular compromise (e.g., diminished pulses, brachial plexus palsy).
- Severe skin tenting with impending soft tissue compromise or necrosis.
- "Floating shoulder" (ipsilateral displaced fractures of the clavicle and the scapular neck), which destabilizes the superior suspensory shoulder complex (SSSC).
Relative Indications (Strongly Supported by Modern Evidence)
- Complete displacement (100% translation with no cortical contact).
- Shortening greater than 1.5 to 2.0 cm.
- Severe comminution (e.g., Z-type fracture fragments).
- Polytrauma patients (to facilitate early mobilization and weight-bearing through the upper extremities for transfers).
- High-demand athletes or manual laborers requiring rapid return to baseline function.
- Symptomatic nonunion or malunion following failed conservative management.
PREOPERATIVE PLANNING AND IMAGING
Standard radiographic evaluation should include:
1. Anteroposterior (AP) View: Provides a general overview of the shoulder girdle.
2. 15° to 20° Cephalic Tilt View (Zanca View): Projects the clavicle above the underlying ribs and scapula, providing an unobstructed view of superior/inferior displacement and comminution.
3. Apical Oblique View: Useful for assessing anterior/posterior translation.
Computed Tomography (CT) with 3D reconstruction is not routinely required for midshaft fractures but is highly valuable for evaluating medial third fractures (to assess sternoclavicular joint involvement) and lateral third fractures (to assess intra-articular extension into the acromioclavicular joint).
SURGICAL TECHNIQUE: OPEN REDUCTION AND INTERNAL FIXATION (ORIF)
Patient Positioning and Preparation
- Position: The patient is placed in a modified beach-chair position (elevated 30° to 45°) on a radiolucent table.
- Support: A folded towel or small bump is placed vertically between the scapulae to allow the shoulders to fall posteriorly. This maneuver helps restore clavicular length and aids in preliminary fracture reduction.
- Draping: The entire forequarter, from the base of the neck to the sternum and past the acromion, is prepped and draped free. The ipsilateral arm must be draped free to allow intraoperative manipulation, which is crucial for achieving reduction.
Surgical Approach
Two primary plating positions are utilized: superior and anteroinferior. The surgical incision is tailored to the chosen plating strategy.
- Incision: A transverse incision is made centered over the fracture site. For superior plating, the incision is placed slightly superior to the clavicle. For anteroinferior plating, the incision is placed slightly inferior to the clavicle. Alternatively, an incision following Langer's lines (oblique, supraclavicular) can be used for superior cosmetic outcomes, though it limits extensile exposure.
- Superficial Dissection: The skin and subcutaneous tissues are incised. The platysma muscle is divided in line with the incision.
- Nerve Preservation:
> Surgical Pitfall: The supraclavicular nerves (medial, intermediate, and lateral branches from the C3-C4 cervical plexus) course superficially over the clavicle. Every effort must be made to identify, mobilize, and protect these branches. Iatrogenic transection results in a numb patch over the anterior chest wall and can lead to painful neuroma formation. - Deep Dissection: The clavipectoral fascia is incised. Subperiosteal dissection should be strictly limited to the fracture ends to preserve the periosteal blood supply, which is critical for fracture healing. Avoid aggressive circumferential stripping of comminuted butterfly fragments.
Fracture Reduction
- The fracture ends are debrided of hematoma and interposed soft tissue.
- The arm is manipulated (abducted and pushed superiorly/posteriorly) to assist with gross reduction.
- Pointed reduction forceps (Weber clamps) are applied to the main medial and lateral fragments.
- If a large butterfly fragment is present, it can be anatomically reduced and provisionally held with Kirschner wires or definitively fixed to one of the main fragments using a 2.7 mm or 3.5 mm lag screw, converting a complex fracture into a simple two-part fracture.
Plate Selection and Application
The choice between superior and anteroinferior plating depends on surgeon preference, fracture morphology, and patient anatomy.
- Superior Plating: Biomechanically advantageous as it places the plate on the tension band side of the bone. Pre-contoured locking plates match the S-shape of the clavicle. However, superior plates are more prominent under the skin, leading to higher rates of symptomatic hardware irritation and subsequent removal.
- Anteroinferior Plating: Offers a safer trajectory for drilling (screws are directed posterosuperiorly, away from the neurovascular bundle). The plate is cushioned by the pectoralis major, resulting in less hardware prominence. Furthermore, the screws can often be longer, providing excellent pull-out strength.
Fixation Steps:
1. The selected plate (typically a 3.5 mm pre-contoured locking or non-locking reconstruction plate) is applied to the reduced fracture.
2. A minimum of three bi-cortical screws (six cortices) should be placed on each side of the fracture. In osteoporotic bone or comminuted fractures, locking screws are preferred to enhance construct stability.
3. If the fracture pattern is oblique, a lag screw can be placed either independently outside the plate or through the plate to provide interfragmentary compression.
4. Fluoroscopy is utilized to confirm anatomic reduction, appropriate plate positioning, and correct screw length. Ensure no screws are excessively long, particularly in the medial and middle thirds.
Closure
- The wound is copiously irrigated with sterile saline.
- The clavipectoral fascia and platysma are meticulously closed as a distinct layer using absorbable sutures (e.g., 2-0 Vicryl) to ensure adequate soft tissue coverage over the hardware.
- The subcutaneous tissue is closed with inverted interrupted sutures.
- The skin is closed with a running subcuticular suture (e.g., 4-0 Monocryl) or surgical staples, depending on surgeon preference and tissue quality.
ALTERNATIVE FIXATION: INTRAMEDULLARY NAILING
For simple, transverse, or short oblique midshaft fractures without significant comminution, intramedullary (IM) fixation using Titanium Elastic Nails (TENs) or specialized clavicle pins is a viable alternative to plate osteosynthesis.
Advantages of IM Fixation:
* Smaller incisions and superior cosmetic outcomes.
* Minimal periosteal stripping, preserving the fracture hematoma.
* Load-sharing construct that promotes secondary bone healing via callus formation.
* Easier hardware removal.
Disadvantages:
* Inability to control rotation or maintain length in highly comminuted fractures.
* Risk of medial or lateral hardware migration, which can cause skin irritation or, rarely, intrathoracic migration.
POSTOPERATIVE PROTOCOL AND REHABILITATION
A structured, phased rehabilitation program is critical to restoring shoulder kinematics while protecting the surgical fixation.
Phase I: Immediate Postoperative (Weeks 0-2)
- The patient is placed in a broad arm sling for comfort.
- Immediate initiation of active range of motion (ROM) for the elbow, wrist, and hand to prevent stiffness.
- Pendulum exercises for the shoulder are permitted.
- Strict avoidance of active shoulder elevation above 90° and lifting objects heavier than a coffee cup.
Phase II: Early Mobilization (Weeks 2-6)
- The sling is gradually weaned.
- Initiate passive and active-assisted ROM exercises (e.g., pulley exercises, wand exercises).
- Progress to active ROM as tolerated, avoiding forceful end-range stretching.
- Scapular retraction and posture exercises are emphasized.
Phase III: Strengthening (Weeks 6-12)
- Radiographs are obtained at 6 weeks to assess for callus formation and maintenance of hardware position.
- Once clinical and radiographic signs of early union are present, isometric strengthening begins.
- Progress to isotonic strengthening using resistance bands and light weights.
- Focus on the rotator cuff and periscapular stabilizers.
Phase IV: Return to Activity (Months 3-6)
- Unrestricted ROM and progressive heavy lifting are permitted once complete radiographic union is confirmed (typically 10-16 weeks).
- Return to contact sports is generally delayed until 4 to 6 months postoperatively, ensuring the bone has remodeled sufficiently to withstand high-impact forces.
COMPLICATIONS AND MANAGEMENT
While ORIF of the clavicle yields excellent outcomes, surgeons must be prepared to manage potential complications.
- Hardware Prominence and Irritation: The most common complication following clavicle plating, particularly with superior plates. Up to 30% of patients may request plate removal. Removal should be delayed until at least 12 to 18 months postoperatively to minimize the risk of refracture.
- Nonunion: Despite operative fixation, nonunion occurs in 1% to 5% of cases, often due to inadequate fixation, excessive periosteal stripping, or patient non-compliance (e.g., smoking). Management requires revision ORIF with rigid locking plates and autologous bone grafting (e.g., iliac crest bone graft).
- Infection: Superficial infections are managed with oral antibiotics. Deep infections require prompt surgical debridement, hardware retention (if the construct is stable and the fracture is unhealed), and culture-directed intravenous antibiotics.
- Adhesive Capsulitis: Post-traumatic shoulder stiffness can occur, particularly in older patients or those with prolonged immobilization. Early, supervised physical therapy is the best preventative measure.
- Neurovascular Injury: Rare but devastating. Meticulous surgical technique, proper retractor placement, and careful drilling trajectories are paramount to avoiding injury to the subclavian vessels and brachial plexus.
CONCLUSION
The management of clavicle fractures has undergone a significant evolution. While conservative management remains appropriate for minimally displaced fractures, the modern orthopedic literature unequivocally supports open reduction and internal fixation for displaced, shortened, or comminuted midshaft fractures. By adhering to strict biomechanical principles, respecting the delicate surrounding neurovascular anatomy, and employing meticulous surgical techniques, orthopedic surgeons can reliably achieve anatomic restoration, minimize nonunion rates, and facilitate a rapid return to optimal function for their patients.
You Might Also Like