Percutaneous Reduction and Fixation of Calcaneal Fractures: A Comprehensive Surgical Guide
Key Takeaway
Percutaneous reduction and fixation of calcaneal fractures offers a minimally invasive alternative to extensile lateral approaches, significantly reducing wound complications. This technique utilizes targeted stab incisions, fluoroscopic or arthroscopic guidance, and precise screw placement to restore the posterior facet and tuberosity alignment. Ideal for Sanders type II fractures, it provides comparable functional outcomes to open reduction while accelerating return to work and minimizing soft tissue morbidity in high-risk patients.
Introduction and Biomechanical Rationale
The management of displaced intra-articular calcaneal fractures remains one of the most debated topics in orthopedic trauma. Historically, the extensile lateral approach has been the gold standard for open reduction and internal fixation (ORIF), providing unparalleled visualization of the posterior facet and lateral wall. However, this approach is fraught with significant soft tissue morbidity, including marginal wound necrosis, dehiscence, and deep infection, owing to the tenuous vascular supply of the lateral hindfoot angiosome.
To mitigate these risks, percutaneous reduction and fixation techniques have emerged as a highly effective, minimally invasive alternative. By utilizing targeted stab incisions, indirect reduction maneuvers, and fluoroscopic or arthroscopic assistance, orthopedic surgeons can achieve anatomical restoration of the posterior facet and calcaneal tuberosity while preserving the delicate soft tissue envelope. This approach is particularly advantageous in patients with significant comorbidities, such as diabetes mellitus, peripheral vascular disease, or a history of tobacco use, where an extensile approach would carry an unacceptably high risk of wound breakdown.
Clinical Pearl: The primary biomechanical goals of calcaneal fracture fixation are the restoration of congruity in the subtalar joint (specifically the posterior facet), the recovery of calcaneal height (Böhler’s angle) and width, and the correction of varus malalignment of the tuberosity. Failure to correct varus malrotation severely limits transverse tarsal joint mobility and leads to debilitating lateral impingement.
Preoperative Planning and Patient Positioning
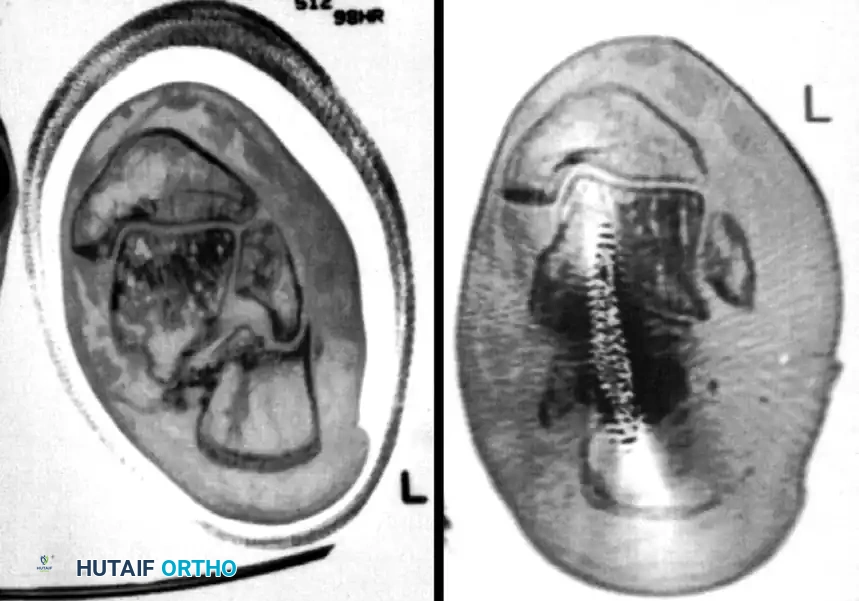
Meticulous preoperative planning is essential for successful percutaneous fixation. Standard radiographs, including lateral, axial (Harris), and anteroposterior views of the foot, should be obtained. A fine-cut computed tomography (CT) scan with sagittal and coronal reconstructions is mandatory to delineate the fracture pattern, assess the degree of posterior facet comminution, and classify the injury according to the Sanders classification system. Percutaneous techniques are most amenable to Sanders Type IIA and IIB fractures, where the posterior facet is split into two primary articular fragments.
Operating Room Setup
- Positioning: Place the patient in the lateral decubitus position on a radiolucent operating table. A bean bag positioner is highly recommended to maintain stability.
- Tourniquet: Apply a well-padded thigh tourniquet to provide a bloodless surgical field, though inflation may only be necessary during specific open reduction steps or if excessive bleeding obscures arthroscopic visualization.
- Fluoroscopy: Position the C-arm fluoroscope to allow unimpeded access for lateral, axial (Harris), and Broden’s views. The ability to rapidly transition between these views is critical for assessing articular reduction and hardware trajectory.
Step-by-Step Surgical Technique
1. Traction and Tuberosity Control
The initial step in percutaneous fixation involves regaining control of the displaced calcaneal tuberosity, which is typically pulled proximally and into varus by the Achilles tendon.
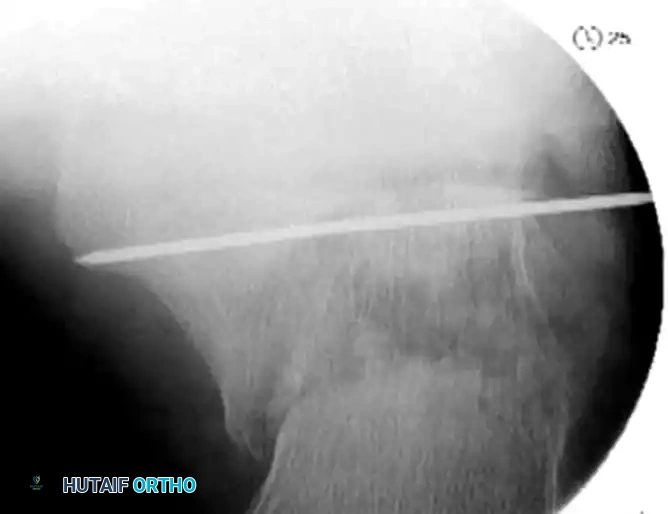
- Insert a large, fully threaded Steinmann pin or Schanz screw transversely into the posteroinferior aspect of the tuberosity fragment.
- Apply sustained manual traction in a plantar and valgus direction. This maneuver utilizes ligamentotaxis to disimpact the fracture fragments, restore calcaneal height, and correct the varus deformity.
- If manual traction is insufficient, a temporary external fixator or a femoral distractor can be applied between the calcaneal tuberosity and the distal tibia to maintain length and alignment during the procedure.
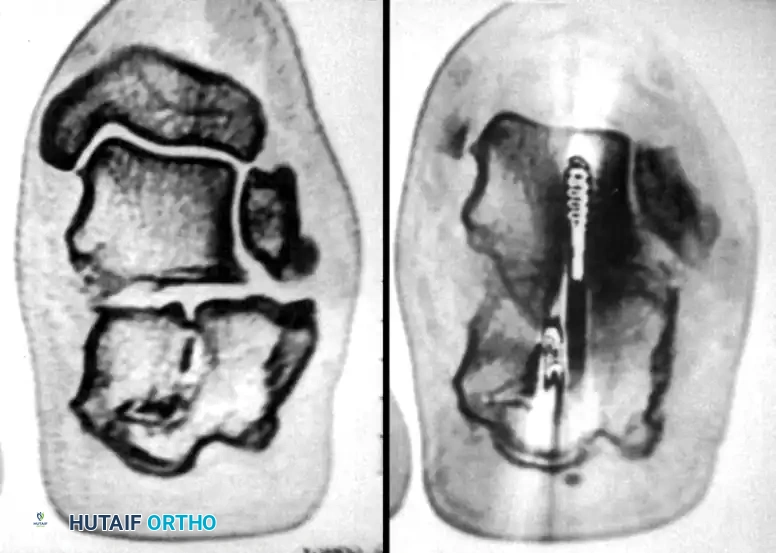
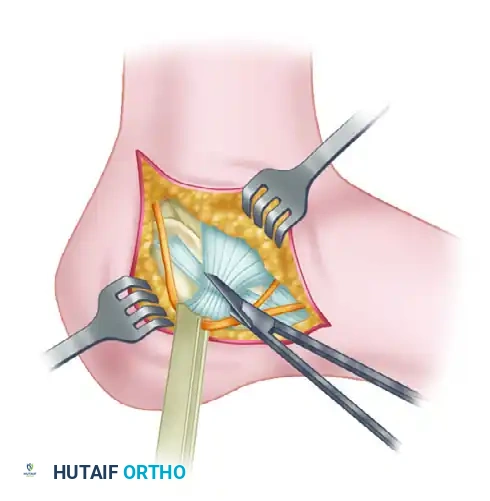
2. Reduction of the Posterior Facet
Once the tuberosity is disimpacted, attention is directed to the articular surface of the subtalar joint.
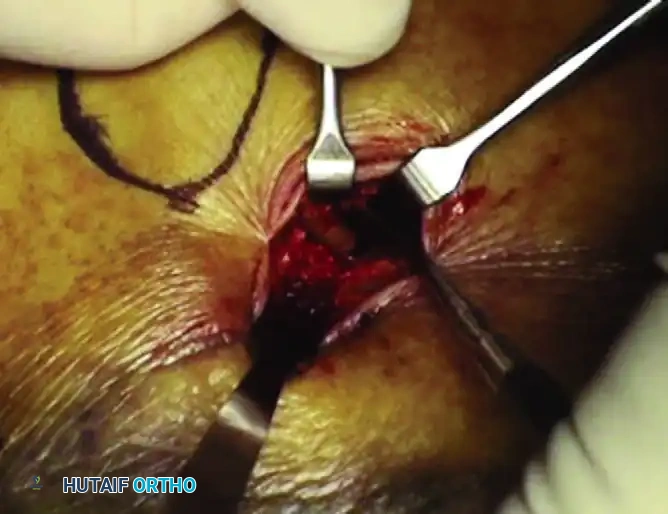
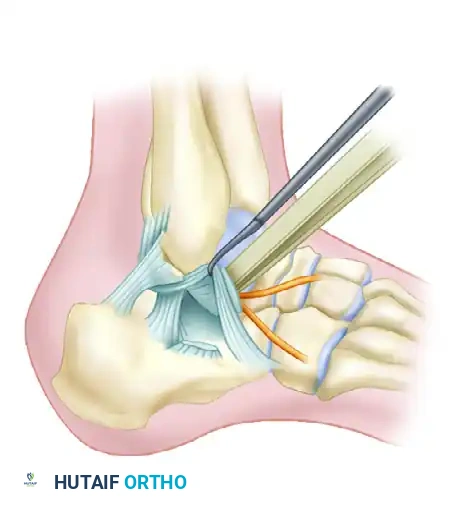
- Make a small stab incision directly over the sinus tarsi, guided by fluoroscopy.
- Introduce a small periosteal elevator or a specialized bone tamp through the incision. Position the instrument beneath the depressed posterior facet fragment.
- Under continuous fluoroscopic guidance (utilizing Broden’s views), gently elevate the articular fragment until it is flush with the "constant" sustentacular fragment.

Surgical Warning: Subtalar arthroscopy can be an invaluable adjunct during this step, particularly for Sanders Type IIA and IIB fractures. It provides direct, magnified visualization of the articular cartilage, ensuring an anatomical reduction that fluoroscopy alone may fail to confirm.
3. Provisional Fixation
Once anatomical reduction of the posterior facet is achieved, it must be provisionally stabilized before definitive screw placement.
- Insert multiple smooth Kirschner wires (K-wires) from the lateral aspect of the calcaneus, directing them medially into the dense bone of the sustentaculum tali.
- Verify the position of the K-wires using axial and Broden’s fluoroscopic views to ensure they do not penetrate the subtalar joint or the medial neurovascular bundle.

4. Definitive Fixation
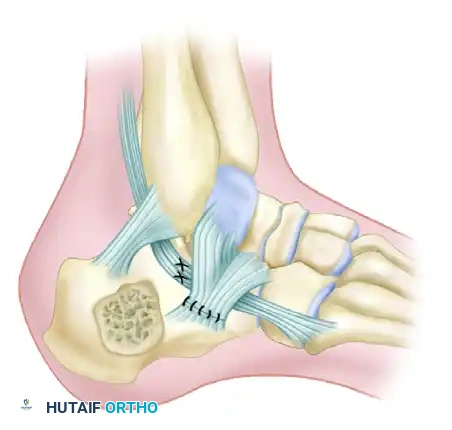
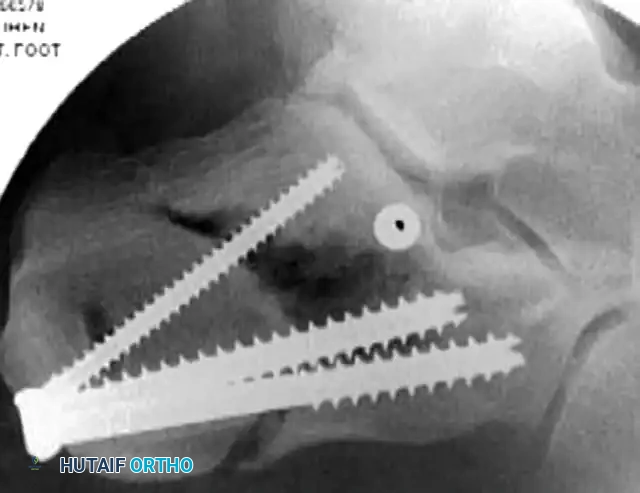
Definitive stabilization is achieved using cannulated screws, which provide compression across the fracture lines and rigid maintenance of the restored anatomy.
- Place 3.5-mm or 4.0-mm partially threaded cortical screws over the provisional K-wires. These screws are directed from lateral to medial, compressing the lateral articular fragment against the medial sustentacular fragment.
- To maintain the corrected position of the tuberosity, insert fully threaded screws from the posterior tuberosity directed anteriorly toward the calcaneocuboid joint, parallel to the initial Steinmann pin. Fully threaded screws are preferred here to act as position screws, preventing loss of calcaneal length.
- Remove the Steinmann pin and any remaining provisional K-wires.
- Perform a final fluoroscopic check to confirm extra-articular hardware placement, restoration of Böhler’s angle, and correction of varus alignment.
- Close the stab incisions using simple interrupted non-absorbable sutures.

Complications and Prevention Strategies
Wound Necrosis, Dehiscence, and Infection
Soft tissue edema and contusion are inherent aspects of high-energy calcaneal fractures. Operating through such compromised soft tissue—especially in the lateral hindfoot, which possesses a tenuous blood supply and lacks a protective muscle layer between the skin and bone—entails a significant risk of marginal wound necrosis.
Historically, after a standard extensile L-shaped approach with two-layer flap closure, wound complications developed in up to 25% of patients, with 21% requiring secondary surgical intervention (e.g., debridement, flap coverage). Other reported rates of marginal wound necrosis vary from 2% to 11%, and deep soft tissue infection rates can reach 7%. Risk factors for wound complications include diabetes mellitus, active smoking, open fractures, single-layer closure, extended time between injury and surgery, and a high body mass index (BMI).
Although the percutaneous approach drastically reduces these risks, serious complications can be further minimized by adhering to the following principles:
1. Smoking Cessation: Wound problems occur exponentially more frequently in active smokers. Patients must be strictly advised to abstain from smoking until complete wound healing is achieved.
2. Tissue Handling: If an open approach is utilized, carefully retracting the soft tissues and maintaining a full-thickness flap (including the periosteum) is crucial to preserve the calcaneal branch of the peroneal artery.
3. Drainage: Drains should be used under the lateral flap in open procedures to prevent postoperative hematoma formation, which can increase tension and compromise flap perfusion.
4. Closure Techniques: A meticulous two-layer closure should be performed, closing the wound from both ends toward the apex.
5. Suture Management: Sutures should be left in place for a minimum of 2 to 3 weeks. Early aggressive range-of-motion exercises should be avoided during this critical healing phase to lessen shear forces under the flap.
Loss of Reduction of Major Fragments
Loss of reduction, particularly of the tuberosity fragment, can occur if weight-bearing is initiated prematurely. Patients must be maintained on a strict non-weight-bearing protocol for a minimum of 8 to 10 weeks to prevent hardware failure and secondary displacement.
Malreduction
Accurately restoring the proper valgus alignment of the tuberosity fragment is paramount. The human foot tolerates varus malrotation exceptionally poorly, as it locks the transverse tarsal joint, leading to a rigid, painful midfoot and severe lateral subfibular impingement. Intraoperative axial Harris radiographs must be scrutinized to avoid this catastrophic complication.
Sural Nerve and Peroneal Tendon Injuries
Sural nerve and peroneal tendon injuries are more frequently associated with the extensile lateral approach but can occur during percutaneous pin placement. The sural nerve courses posterior and inferior to the peroneal tendons and must be protected during stab incisions. Peroneal tendons are particularly vulnerable to subluxation or laceration if the lateral calcaneal wall remains blown out. Limited periosteal elevation and the use of drill sleeves during percutaneous fixation are mandatory to prevent iatrogenic injury.
Evidence-Based Outcomes and Results
Significant controversy has historically surrounded the results of nonoperative versus operative treatment for calcaneal fractures. However, modern literature provides clear guidance.
In 2002, Buckley et al. published a landmark multicenter, prospective, randomized, controlled trial comparing operative and nonoperative management of displaced intra-articular calcaneal fractures. The findings fundamentally shaped modern protocols:
1. Without stratification, overall outcomes between operative and nonoperative groups were statistically similar.
2. Patients receiving workers’ compensation fared significantly worse regardless of treatment modality.
3. Crucially, after excluding the workers’ compensation cohort, patients managed operatively had significantly improved functional scores compared to those treated nonoperatively.
4. Women demonstrated significantly improved scores with operative treatment.
5. The subsequent need for subtalar arthrodesis was higher in patients treated nonoperatively, those with an initial Böhler angle of less than 0 degrees, and those with Sanders Type IV fractures.
6. Younger, self-employed patients reported improved gait satisfaction following operative fixation.
7. Bilateral fractures treated nonoperatively were highly likely to require subsequent arthrodesis.
Regarding percutaneous fixation specifically, studies report 61% to 72% good or excellent results, with 74% to 100% of patients successfully returning to work. The infection rate is remarkably low, ranging from 0% to 15%. When compared to historical controls of standard ORIF, patients undergoing percutaneous reduction returned to work earlier and demonstrated superior range of motion in the subtalar joint. The addition of injectable calcium sulfate bone cement to percutaneous fixation has been shown to allow earlier weight-bearing and yield better functional outcome scores without compromising the quality of the reduction.
Late Complications and Calcaneal Malunion
Regardless of the initial treatment method, chronic pain develops in a subset of patients, severely limiting their capacity to work and perform activities of daily living. Late complications leading to a painful outcome include:
- Posttraumatic arthrosis of the subtalar joint.
- Lateral subfibular impingement (often involving the peroneal tendons).
- Anterior ankle impingement resulting from the loss of the normal plantar-flexed position of the talus.
- Tibial or sural nerve entrapment.
- Plantar fat pad atrophy.
- Complex Regional Pain Syndrome (CRPS).
Classification of Calcaneal Malunions
Stephens and Saunders developed a prognostic CT-based classification system for calcaneal malunions to guide surgical reconstruction:
- Type I: Lateral wall exostosis without subtalar arthrosis.
- Type II: Lateral wall exostosis with significant subtalar arthrosis.
- Type III: Lateral wall exostosis, subtalar arthrosis, and varus malunion of the calcaneal body.


Surgical Management of Calcaneal Malunion
Patients presenting with chronic lateral subtalar pain must be evaluated for posttraumatic arthrofibrosis/arthrosis and lateral calcaneofibular impingement. A combination of CT imaging and selective subtalar injection of local anesthetic is highly diagnostic.
For patients requiring surgical intervention for malunion, the technique described by Braly, Bishop, and Tullos provides an excellent framework for lateral decompression and realignment:
-
Incision: Make an incision just plantar to the course of the peroneal tendons.

-
Nerve Decompression: Carefully identify and decompress the sural nerve, which is often encased in scar tissue.

-
Tenolysis: Incise the inferior extensor retinaculum and perform a thorough peroneal tenolysis.
-
Ligament Release: Transect the calcaneofibular ligament to fully expose the lateral wall of the calcaneus.
-
Osteotomy: Perform a lateral calcaneal osteotomy to resect the impinging lateral wall exostosis.

-
Tendon Lengthening: If the peroneal tendons are contracted or anteriorly dislocated, perform a Z-lengthening procedure.

-
Reconstruction: Repair or reconstruct the inferior retinaculum, ensuring the lengthened peroneal tendons are securely relocated in their anatomical groove.
By adhering to these rigorous biomechanical principles and minimally invasive techniques, orthopedic surgeons can optimize functional recovery, minimize devastating soft tissue complications, and effectively manage the complex sequelae of calcaneal fractures.
You Might Also Like
