Lateral Decompression of Malunited Calcaneal Fractures: A Comprehensive Surgical Guide
Key Takeaway
Lateral decompression of a malunited calcaneal fracture addresses lateral impingement syndrome caused by lateral wall blowout. This procedure involves sural nerve neurolysis, peroneal tenolysis, and lateral wall ostectomy to restore hindfoot morphology. It is indicated for patients with isolated lateral impingement without severe subtalar arthritis. Proper execution relieves subfibular pain, restores peroneal tendon excursion, and improves shoe wear tolerance, offering a reliable salvage option before considering arthrodesis.
INTRODUCTION TO CALCANEAL MALUNION AND LATERAL IMPINGEMENT
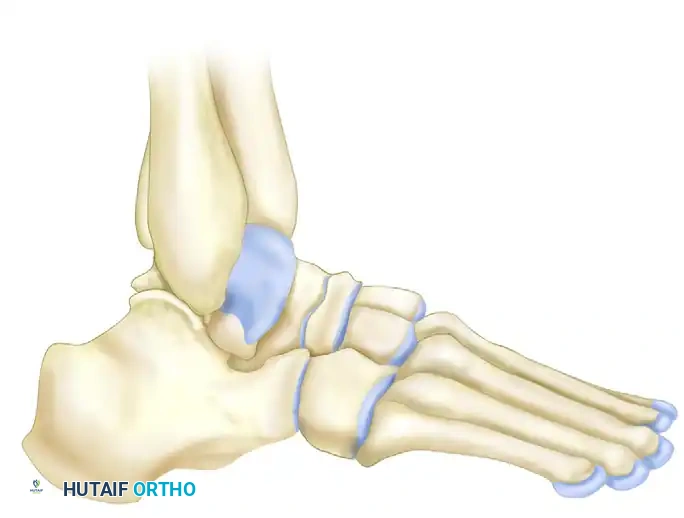
The management of malunited calcaneal fractures presents a formidable challenge to the orthopedic surgeon. Historically, nonoperative treatment of displaced intra-articular calcaneal fractures frequently resulted in a characteristic and debilitating malunion. The hallmark of this deformity is a loss of calcaneal height, an increase in heel width (the "lateral blowout"), and a varus or valgus malalignment of the tuberosity.
Among the most symptomatic components of this malunion is the lateral exostosis. As the lateral wall of the calcaneus expands outward during the initial axial load injury, it heals in a laterally displaced position. This creates a severe mechanical conflict within the subfibular space, leading to direct impingement of the peroneal tendons and the sural nerve against the distal tip of the lateral malleolus.
Lateral decompression of a malunited calcaneal fracture, as popularized by Braly, Bishop, and Tullos, is a highly effective salvage procedure designed to address this specific pathoanatomy. By excising the prominent lateral bony mass, performing a peroneal tenolysis, and releasing the sural nerve, surgeons can reliably restore hindfoot morphology, alleviate subfibular pain, and improve shoe wear tolerance in carefully selected patients.
PATHOANATOMY AND BIOMECHANICS
Understanding the three-dimensional deformity of a calcaneal malunion is critical for successful surgical intervention. The primary deforming forces during the initial injury result in a predictable pattern of structural collapse:
- Loss of Height: The posterior facet is driven into the body of the calcaneus, decreasing the talocalcaneal angle and the calcaneal pitch. This results in a horizontal talus, which severely limits ankle dorsiflexion due to anterior tibiotalar impingement.
- Increase in Width: The lateral wall is blown out, obliterating the normal subfibular sulcus. This creates a "nutcracker" effect, compressing the peroneus brevis and longus tendons between the lateral malleolus and the expanded calcaneal wall.
- Peroneal Tendon Pathology: Chronic compression leads to tenosynovitis, tendon flattening, longitudinal tears, and in severe cases, subluxation or dislocation of the tendons out of the retromalleolar groove.
- Sural Nerve Entrapment: The sural nerve, coursing superficial to the peroneal tendons, becomes encased in dense perineural fibrosis or is directly compressed by the lateral bony prominence, leading to intractable neuropathic pain and neuroma formation.
Clinical Pearl: The severity of lateral impingement is often underestimated on standard radiographs. A thorough clinical examination, including palpation of the subfibular space and assessment of peroneal tendon excursion, is paramount. Pain that is strictly localized to the lateral subfibular region, without deep sinus tarsi pain, is the ideal indication for an isolated lateral decompression.
PREOPERATIVE EVALUATION AND IMAGING
A meticulous preoperative evaluation is required to differentiate isolated lateral impingement from global subtalar post-traumatic arthritis. Patients with advanced subtalar arthritis will not achieve satisfactory pain relief from lateral decompression alone and will require a subtalar arthrodesis.
Clinical Examination
Evaluate the hindfoot alignment in a weight-bearing position. Assess the flexibility of the transverse tarsal and subtalar joints. Palpate the peroneal tendons for tenderness, swelling, and instability during active eversion and dorsiflexion. Perform a Tinel's test along the course of the sural nerve to identify areas of entrapment or neuroma formation.
Radiographic Assessment
Standard weight-bearing radiographs of the foot and ankle are mandatory. A lateral standing radiograph must be scrutinized carefully to evaluate the overall geometry of the hindfoot.
Key radiographic measurements include:
* Talocalcaneal Height: Assesses the degree of vertical collapse.
* Cuboid-to-Floor and Navicular-to-Floor Distances: Evaluates the integrity of the longitudinal arch.
* Calcaneal Pitch Angle: Typically decreased in malunions.
* Talocalcaneal Angle: Evaluates the relationship between the talus and calcaneus.
* First Talometatarsal Angle: Assesses midfoot sag.
* Talar Declination Angle: This is a critical measurement. The talar angle of declination must be evaluated because it measures the excursion of the tibiotalar joint in extension. A severely depressed talar declination angle indicates a horizontal talus, which blocks ankle dorsiflexion.
In addition to plain films, a Computed Tomography (CT) scan (axial, coronal, and sagittal planes) is the gold standard for evaluating a calcaneal malunion. Coronal cuts perfectly demonstrate the lateral wall blowout, the degree of subfibular impingement, and the status of the subtalar joint cartilage.
SURGICAL TECHNIQUE: STEP-BY-STEP LATERAL DECOMPRESSION
The procedure described by Braly, Bishop, and Tullos focuses on a systematic approach to the lateral hindfoot, addressing the nerve, tendons, and bone in a sequential manner.
1. Patient Positioning and Anesthesia
- Administer general or regional anesthesia.
- Place the patient in a lateral decubitus position or a "sloppy lateral" position.
- Place a bump or roll under the ipsilateral hip to allow for internal rotation of the leg, providing greater, unobstructed exposure of the lateral aspect of the foot and ankle.
- Apply and inflate a pneumatic thigh tourniquet to ensure a bloodless surgical field, which is critical for identifying the sural nerve and assessing tendon viability.
2. Incision and Exposure
- Make a curved, extensile lateral incision. The incision should be placed just plantar to the course of the peroneal tendons, extending from the posterior aspect of the lateral malleolus to the region of the calcaneocuboid joint.
- Surgical Warning: If a previous subtalar fusion or open reduction internal fixation (ORIF) has been performed, attempt to use the existing incision to prevent intervening skin bridge necrosis.
3. Sural Nerve Neurolysis and Management
- The first critical step is the identification and protection of the sural nerve.
- Carefully dissect through the subcutaneous tissues. Identify the sural nerve and release it from the surrounding scar tissue. Perform a meticulous neurolysis, tracing the nerve to more normal anatomy both proximally and distally.
- If the nerve is severely crushed, encased in unyielding scar, or if distinct neuromas are present, excision is required. Excise any neuromas present, and dissect the nerve back proximally. Bury the proximal stump deep into muscle belly or bone in an area where the potential for external irritation over bony prominences during shoe wear is minimized.
4. Peroneal Tenolysis
- Once the nerve is managed and retracted safely, turn your attention to the peroneal tendons.
- Incise the peroneal tendon sheath longitudinally. Crucial Step: Take extreme care not to completely divide the superior peroneal retinaculum proximally, as this will lead to iatrogenic tendon dislocation.
- Perform a thorough tenolysis. Free the peroneus brevis and longus from all adhesions. Inspect the tendons for longitudinal tears; if present, debride and tubularize the tendons using fine non-absorbable suture.
5. Ligamentous Release
- With the peroneal tendons and sural nerve safely retracted (usually superiorly and anteriorly), identify the calcaneofibular ligament (CFL).
- Incise the calcaneofibular ligament to gain access to the lateral wall of the calcaneus.
- Note: Do not attempt to reconstruct the calcaneofibular ligament at the conclusion of the procedure. The inherent stiffness of the post-traumatic hindfoot typically renders lateral ankle instability a non-issue.
6. Lateral Wall Ostectomy (The Decompression)
- Incise longitudinally the floor of the peroneal tendon sheath and the underlying periosteum over the lateral calcaneus.
- Using a periosteal elevator, perform a subperiosteal dissection to expose the prominent lateral bony mass of the calcaneus.
- Utilize an osteotome, oscillating saw, or high-speed burr to excise the lateral exostosis.
- Goal of Resection: The amount of bone removed depends on the degree of lateral impingement evident intraoperatively and on preoperative CT scans. Attempt to narrow the heel, at least laterally, to a more normal width.
- Pitfall Avoidance: Exercise extreme caution to avoid violating the subtalar and calcaneocuboid joints during the bony resection.
- Once the bulk of the bone is removed, smooth all rough edges with a rongeur and a rasp. Ensure that the peroneal tendons can glide smoothly over the decorticated lateral wall without any friction or catching.
7. Management of Peroneal Tendon Instability
- In cases of chronic, severe blowout, the peroneal tendons may be dislocated or highly unstable once the lateral wall is removed.
- If the peroneal tendons are dislocated and contracted, Braly et al. recommended a Z-lengthening of both tendons before relocating them behind the lateral malleolus. Note: Routine lengthening of these tendons is not strictly necessary unless severe contracture prevents relocation.
- If the retinaculum is incompetent, repair it directly. If direct repair is impossible, reconstruct the retinaculum using an osteoperiosteal strip harvested from the lateral malleolus, as described by Zoellner and Clancy, performed after the ostectomy.
8. Hemostasis and Closure
- Repair the reflected overlying periosteum or the floor of the tendon sheath over the bed of the ostectomy to provide a smooth gliding surface for the tendons.
- If any raw cancellous bone is left exposed and bleeding, apply bone wax meticulously to achieve hemostasis and prevent postoperative hematoma formation, which can lead to recurrent fibrosis.
- Deflate the tourniquet and achieve meticulous pinpoint hemostasis.
- Close the subcutaneous tissues and skin in a routine fashion. Apply a bulky, soft, compressive dressing.
ADVANCED SALVAGE: SUBTALAR DISTRACTION BONE BLOCK ARTHRODESIS
While isolated lateral decompression is excellent for pure lateral impingement, many patients present with concurrent, painful post-traumatic subtalar arthritis. In these scenarios, lateral decompression must be combined with a subtalar arthrodesis.
Furthermore, the interval between the injury and the salvage procedure dictates the functional outcome; the longer the interval, the longer it takes for the patient to return to full activity or work. Functional outcomes are generally better in patients who undergo a late subtalar arthrodesis after an initial ORIF compared to those who were initially treated nonoperatively, as the initial ORIF often preserves some calcaneal morphology.
For patients who are candidates for subtalar arthrodesis, the lateral standing radiograph is the deciding factor. If the patient has a severely depressed talar angle of declination (a horizontal talus causing anterior ankle impingement), an in situ fusion is insufficient.
For these complex deformities, Carr et al. modified a procedure originally described by Gallie: the Subtalar Distraction Bone Block Arthrodesis.
Principles of Distraction Arthrodesis
This technically demanding procedure aims to simultaneously fuse the arthritic subtalar joint while restoring calcaneal height and the talar declination angle.
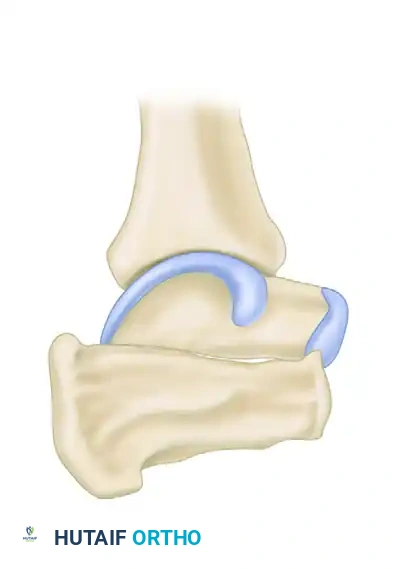
1. The subtalar joint is opened, and all residual cartilage and subchondral bone are resected down to bleeding cancellous bone.
2. A lamina spreader is inserted into the posterior facet to distract the joint. This action plantarflexes the talus (restoring the talar declination angle) and dorsiflexes the calcaneus (restoring calcaneal pitch).
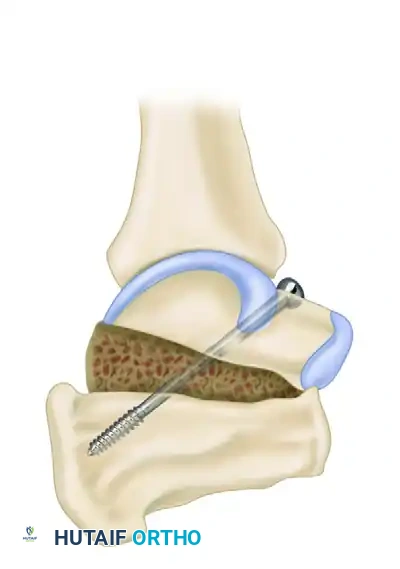
3. A tricortical iliac crest bone graft (or structural allograft) is fashioned to fit the distracted defect.
4. The graft is impacted into place, and the construct is rigidly fixed, typically with large-fragment cannulated screws directed from the calcaneal tuberosity up into the body of the talus.
Although technically demanding, the postoperative appearance of the foot and the improved ankle dorsiflexion (due to the unblocking of the anterior tibiotalar joint) can be highly impressive. A number of studies have demonstrated the usefulness of subtalar distraction bone block arthrodesis for the late complications of calcaneal fractures.
Surgical Warning: Failures of distraction arthrodesis typically occur in patients with pre-existing transverse tarsal joint arthritis, severe uncorrected malunions, and unresolved nerve problems. Therefore, meticulous patient selection and concurrent lateral wall decompression (if impingement is present) are mandatory.
POSTOPERATIVE CARE AND REHABILITATION
The postoperative protocol must be tailored to the exact procedures performed during the surgery.
Protocol for Isolated Lateral Decompression
- Days 0-3: The patient is placed in a bulky compressive dressing and a posterior splint. Elevation is strictly enforced to minimize edema and wound complications.
- Days 2-3: Early active and passive range of motion of the ankle and subtalar joints is initiated. Progressive weight-bearing as tolerated in a controlled ankle motion (CAM) boot is encouraged.
- Weeks 2-6: Sutures are removed at 2 to 3 weeks. Physical therapy focuses on peroneal strengthening, scar massage, and proprioceptive training.
- Weeks 8-12: Full activity, including impact sports and heavy labor, is generally allowed by 8 to 12 weeks after surgery, provided the wounds are fully healed and peroneal strength is restored.
Protocol for Decompression with Tendon Lengthening/Relocation
If a cast has been applied after peroneal tendon Z-lengthening or retinacular reconstruction, a more conservative approach is required to protect the repair:
* Weeks 0-3: The initial postoperative splint is changed to a short-leg, nonwalking cast before discharge. The patient remains strictly non-weight-bearing for 3 weeks to allow the tendon and retinaculum to heal.
* Weeks 3-6: The nonwalking cast is transitioned to a short-leg walking cast (or a locked CAM boot) for another 3 weeks. Weight-bearing is progressed.
* Weeks 6-12: The cast is removed. Aggressive range-of-motion and strengthening exercises of the ankle are begun. Full activity is delayed until 10 to 12 weeks postoperatively to ensure the integrity of the reconstructed retinaculum.
CONCLUSION
Lateral decompression of a malunited calcaneal fracture is a highly targeted, effective surgical intervention for patients suffering from subfibular impingement. By meticulously addressing the sural nerve, freeing the peroneal tendons, and excising the offending lateral bony mass, surgeons can dramatically improve patient quality of life. When combined with advanced techniques like subtalar distraction bone block arthrodesis for concurrent arthritis and height loss, even the most severe calcaneal malunions can be successfully salvaged. Strict adherence to anatomical principles, careful soft tissue handling, and appropriate postoperative rehabilitation are the cornerstones of a successful outcome.
You Might Also Like
