Acetabulum Posterior Approach: Simplest Fix for Hip Fractures
Key Takeaway
We review everything you need to understand about Acetabulum Posterior Approach: Simplest Fix for Hip Fractures. The acetabulum posterior approach grants surgical access to the posterior wall, posterior column, and dorsocranial acetabulum. Recognized as the easiest acetabular approach, it typically results in minimal blood loss. This approach is primarily utilized for the reduction and fixation of fractures involving the posterior lip, posterior column, and specific simple or associated transverse acetabular fractures.
Introduction and Epidemiology
Acetabular fractures represent a formidable challenge in orthopedic trauma, often resulting from high-energy mechanisms such as motor vehicle collisions or falls from height in younger patients, and low-energy falls in osteoporotic elderly individuals. These intra-articular fractures compromise the structural integrity of the hip joint, potentially leading to immediate instability, long-term degenerative arthritis, and significant functional impairment if not managed appropriately. Accurate anatomical reduction and stable internal fixation are paramount to restoring hip joint congruity and preserving long-term function.
The posterior approach to the acetabulum, commonly referred to as the Kocher-Langenbeck approach, is a cornerstone surgical window for addressing a specific subset of acetabular fracture patterns. Its utility lies in its direct access to the posterior column and posterior wall of the acetabulum, regions frequently involved in hip dislocation injuries. First described by Kocher and Langenbeck in the late 19th century, this approach has evolved, with modern modifications enhancing exposure and minimizing morbidity. While often considered the "simplest" of the major acetabular approaches due to its relatively straightforward anatomical planes and lower associated blood loss compared to extensile anterior approaches, its successful execution still demands meticulous anatomical understanding and refined surgical technique. Epidemiologically, posterior wall and posterior column fractures account for a significant proportion of all acetabular fractures, making proficiency with this approach essential for any orthopedic trauma surgeon. The AO/OTA classification system, a widely adopted framework, categorizes acetabular fractures based on the involvement of the anterior and posterior columns and walls, guiding the selection of surgical approach. The posterior approach is primarily indicated for B-type fractures (partial articular) involving the posterior column and/or wall, and specific C-type fractures (both columns) where the primary displacement is posterior.
Surgical Anatomy and Biomechanics
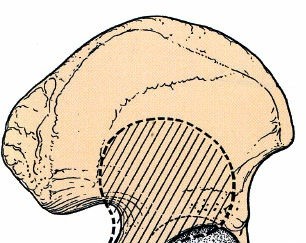
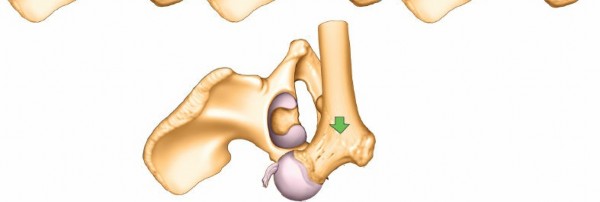
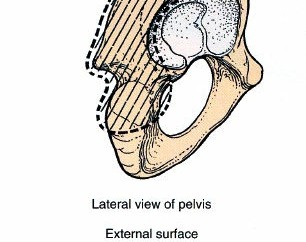
A thorough understanding of the surgical anatomy and biomechanics of the posterior acetabulum is critical for safe and effective surgical intervention via the posterior approach. The acetabulum is formed by the confluence of the ilium, ischium, and pubis. Its posterior column extends from the greater sciatic notch to the ischial tuberosity, while the posterior wall constitutes the posterosuperior rim of the acetabulum, providing critical support for the femoral head.
Osseous Structures and Key Landmarks
The posterior column is a substantial bony buttress that transmits weight from the ilium to the ischium. Fractures involving this column can compromise the structural integrity of the acetabulum. The posterior wall, though thinner, is crucial for resisting posterior translation of the femoral head and preventing hip dislocation. Key landmarks accessible through this approach include the posterior superior iliac spine (PSIS), greater trochanter, ischial tuberosity, and the greater and lesser sciatic notches. The sciatic notch, formed by the posterior inferior iliac spine superiorly and the ischial spine inferiorly, provides passage for the sciatic nerve and gluteal vessels.
Muscular Anatomy and Internervous Planes
The posterior approach involves dissecting through the gluteal musculature.
The gluteus maximus forms the most superficial layer, and its fibers are typically split rather than incised to preserve muscle function. Deep to the gluteus maximus are the gluteus medius and minimus, which originate from the ilium and insert onto the greater trochanter, primarily responsible for hip abduction. Beneath these lie the short external rotators of the hip: piriformis, superior gemellus, obturator internus, inferior gemellus, and quadratus femoris. These muscles originate from the sacrum and ischium and insert into or near the greater trochanter. The piriformis muscle emerges from the greater sciatic notch and is a key landmark, as the sciatic nerve typically exits the pelvis inferior to it. Dissection through this layer often involves sectioning the short external rotators to gain direct access to the posterior capsule and posterior osseous structures. The internervous plane for the posterior approach is largely between the gluteus maximus (innervated by the inferior gluteal nerve) and the gluteus medius/minimus (innervated by the superior gluteal nerve). The deep dissection then proceeds through the short external rotators.
Neurovascular Structures
The most critical neurovascular structure at risk during the posterior approach is the sciatic nerve. It typically exits the pelvis below the piriformis muscle, running inferiorly and laterally to the ischial tuberosity before descending into the posterior thigh. Vigilant identification and protection of the sciatic nerve are paramount throughout the entire procedure.

Other important structures include the superior and inferior gluteal arteries and nerves, which supply the gluteal muscles. The inferior gluteal artery and nerve emerge inferior to the piriformis, running deep to the gluteus maximus. The obturator internus tendon and its associated neurovascular bundle (pudendal nerve and internal pudendal vessels) are located more medially and inferiorly. Hemostasis of vessels within the deep rotator cuff and around the fracture site is important.
Biomechanical Considerations
The posterior column and wall are critical for the biomechanical stability of the hip joint, particularly in resisting posterior forces and preventing dislocation. Fractures of the posterior wall lead to direct loss of containment, while posterior column fractures disrupt the load-bearing axis of the hemipelvis. Anatomical reduction restores the sphericity of the acetabulum and distributes load across the articular cartilage, minimizing stress concentration. Stable fixation, typically with plates and screws contoured to the posterior column and buttressing the posterior wall fragments, is necessary to withstand early weight-bearing stresses and promote fracture healing. The integrity of the weight-bearing dome (cotyloid fossa and superior articular surface) is crucial for long-term outcomes.
Indications and Contraindications
The selection of the posterior approach for acetabular fractures is guided by the specific fracture pattern, patient factors, and the surgeon's experience. This approach provides excellent visualization and access to the posterior column and posterior wall, making it the workhorse for fractures involving these structures.
Indications for the Posterior Approach
The posterior approach is primarily indicated for reduction and fixation of fracture patterns that predominantly involve the posterior aspects of the acetabulum.

These include:
- Fractures of the Posterior Wall: These are common, often associated with posterior hip dislocations, and directly compromise hip stability.
- Fractures of the Posterior Column: These involve the structural buttress of the posterior hemipelvis, extending from the greater sciatic notch to the ischial tuberosity.
- Associated Posterior Wall and Posterior Column Fractures: A combination injury requiring extensive exposure of the posterior aspect.
- Simple Transverse Fractures (Juxta- and Infratectal): Especially when the primary displacement is posterior, allowing access to the transverse fracture line through the posterior approach.
- Transverse Fractures with Associated Posterior Wall Fractures: A common associated pattern.
- Certain T-type Fractures: When the major displacement is posterior and the primary fracture lines can be addressed effectively from this window.
- Acetabular Fractures with Femoral Head Fractures (Pipkin Type I-IV): When a trochanteric osteotomy and surgical dislocation are performed, the posterior approach can be extended to manage femoral head fractures and associated anterior acetabular pathology.
- Dome Fractures: If a trochanteric osteotomy and surgical dislocation of the hip is used, it can also be used for dome fractures, which often involve complex articular damage.
- Anterior Lip Fractures: Similarly, with extended exposure and surgical hip dislocation, certain anterior lip fractures can be addressed.
Contraindications to the Posterior Approach
While versatile, the posterior approach has limitations and is contraindicated in specific scenarios:
- Extensive Anterior Column or Anterior Wall Involvement: When the primary displacement or comminution is extensive anteriorly, and cannot be adequately addressed even with an extended posterior approach and surgical dislocation.
- Extensive Quadrilateral Surface Impaction: When large fragments of the quadrilateral surface are medially displaced, making reduction difficult from the posterior aspect without significant internal manipulation or counter-pressure that may be challenging to achieve.
- High Transverse or Associated Both Column Fractures with Significant Anterior Displacement: Where an ilioinguinal or extended iliofemoral approach would provide superior visualization and reduction capabilities.
- Open Fractures: Depending on the contamination and soft tissue injury, a combined approach or staged procedure might be necessary.
- Severe Osteopenia: While not an absolute contraindication, severe osteopenia can make stable fixation challenging regardless of approach.
- Extreme Patient Morbidity: In severely polytraumatized patients, the duration and invasiveness of complex acetabular surgery must be weighed against their physiological reserve.
Operative vs. Non-Operative Indications
The decision between operative and non-operative management for acetabular fractures is critical and depends on several factors, including fracture stability, articular congruity, patient age, comorbidities, and functional demands.
| Indication Type | Specific Criteria | Rationale |
|---|---|---|
| Operative | - Displaced posterior wall fractures (>2mm displacement, >20% acetabular arc involvement) - Irreducible posterior hip dislocation - Fractures with intra-articular fragments or incarcerated femoral head - Incongruent reduction post-dislocation - Displaced posterior column fractures - Displaced transverse, T-type, or associated fractures primarily amenable to posterior exposure - Unstable hip joint (e.g., positive posterior stress view) |
Restoration of articular congruity and stability to prevent post-traumatic arthritis, avascular necrosis, and persistent instability. Improves long-term functional outcomes and reduces pain. |
| Non-Operative | - Non-displaced or minimally displaced (≤2mm) posterior wall fractures - Stable, concentric reduction of hip dislocation with minimal residual fracture displacement - Posterior column fractures with minimal displacement and stable joint - Elderly, low-demand patients with significant comorbidities precluding surgery - Patients with stable non-operative indications and no incarcerated fragments |
When surgical risks outweigh potential benefits, or when fracture geometry allows for intrinsic stability and good long-term outcomes without intervention. Close follow-up is crucial to monitor for secondary displacement or complications. |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is indispensable for successful acetabular fracture surgery. This includes comprehensive imaging analysis, strategic operative room setup, and precise patient positioning.
Preoperative Imaging and Evaluation
High-quality imaging is the cornerstone of preoperative assessment.

Standard radiographs, including anteroposterior (AP) pelvis, iliac oblique, and obturator oblique views (Judet views), provide initial information about fracture configuration. However, computed tomography (CT) scans with 1mm cuts and 3D reconstructions are mandatory for detailed understanding of the fracture pattern, fragment displacement, articular involvement, and identification of any incarcerated fragments.
3D reconstructions are particularly useful for visualizing the relationship between the femoral head and acetabulum, assessing posterior wall comminution, and planning plate contouring. Preoperative angiography may be considered in cases of suspected vascular injury, though less common for routine posterior approaches. Neurological examination, particularly of the sciatic nerve, is crucial both pre- and postoperatively.
Operative Room Setup and Equipment
The operating room must be prepared with all necessary equipment, including a radiolucent operating table, a high-quality C-arm fluoroscopy unit, a full set of acetabular reduction instruments (e.g., pointed reduction clamps, Farabeuf clamps, ball spike pushers, Hohmann retractors, blunt Homan retractors, dental picks, Kocher clamps, large Lane clamps), and a comprehensive acetabular fixation set (e.g., 3.5mm reconstruction plates, lag screws, cortical screws). Access to a power drill, burr, and oscillating saw (if trochanteric osteotomy is planned) is also essential. Appropriate lighting and magnification are critical.
Patient Positioning
Patient positioning for the posterior approach is vital for optimal exposure, fracture reduction, and sciatic nerve protection.
The choice between lateral decubitus and prone positioning depends on the specific fracture pattern and surgeon preference, as highlighted in the seed content.
Lateral Decubitus Position
This is the most common position for posterior wall and posterior column fractures.
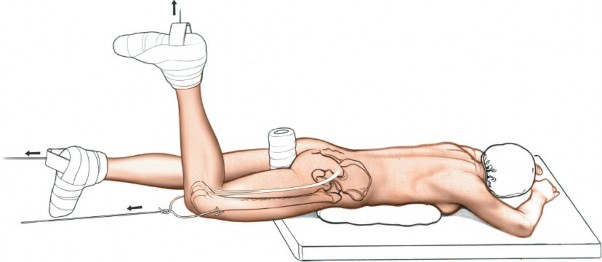
* Procedure: The patient is placed in the lateral decubitus position on a radiolucent table, with the injured side facing upwards.
* Support: The patient is supported anteriorly and posteriorly with beanbag fixators or padded supports at the chest, pelvis, and sacrum to prevent rolling. An axillary roll is placed to protect the brachial plexus.
* Limb Positioning: The ipsilateral upper extremity is abducted on an arm board. The contralateral lower extremity is flexed at the hip and knee, resting on pillows, to allow full range of motion for the operative leg. The operative leg is draped free to allow intraoperative manipulation for reduction maneuvers and assessment of hip stability.
* Fluoroscopy Access: This position allows excellent access for both AP and oblique Judet views with the C-arm, which can be brought in from the contralateral side.
* Trochanteric Osteotomy: This position is also used if a trochanteric osteotomy and surgical dislocation are planned, as it facilitates the precise execution of the osteotomy and subsequent hip dislocation.
Prone Position
This position can be considered for transverse fractures or specific posterior column patterns where maximum access to the posterior aspect of the ischium is required, and where ipsilateral traction can be beneficial.
* Procedure: The patient is placed prone on a radiolucent table.
* Support: Bolsters or chest rolls are placed longitudinally under the chest and anterior superior iliac spines to allow the abdomen to hang free, minimizing vena caval compression and epidural venous bleeding. The knees are slightly flexed.
* Limb Positioning: The lower extremities are positioned to allow for adequate traction if required.
* Traction Considerations: If skeletal traction is to be used, a distal femoral pin can be placed transversely with the knee flexed to reduce the risk of traction injury to the sciatic nerve. This provides continuous longitudinal traction, which can aid in reduction of displaced transverse fracture components.
* Fluoroscopy Access: AP and oblique views can still be obtained, though positioning the C-arm may be slightly more challenging than in the lateral position.
Regardless of the chosen position, ensuring proper padding at all pressure points to prevent nerve compression or skin breakdown is paramount. The surgical field should be prepped and draped to allow full exposure of the posterior hip and proximal thigh.
Detailed Surgical Approach and Technique
The posterior approach (Kocher-Langenbeck) is a robust and versatile method for addressing posterior acetabular fractures. Its core principles involve meticulous dissection, protection of vital neurovascular structures, anatomical reduction, and stable internal fixation.
Skin Incision and Superficial Dissection
Incision
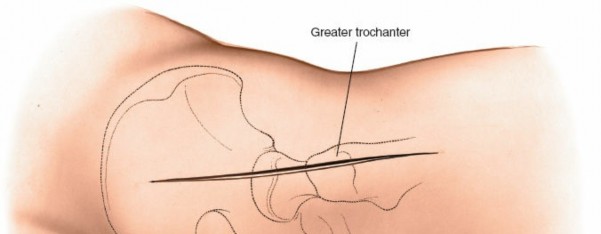
The incision is typically a curved or straight line extending from the posterior superior iliac spine (PSIS) towards the greater trochanter and then distally along the shaft of the femur.
A common variant starts approximately 5cm distal to the PSIS, curving laterally over the greater trochanter, and then extending distally for 10-15 cm along the lateral aspect of the thigh. The length and curvature can be adjusted based on the required exposure and patient habitus.
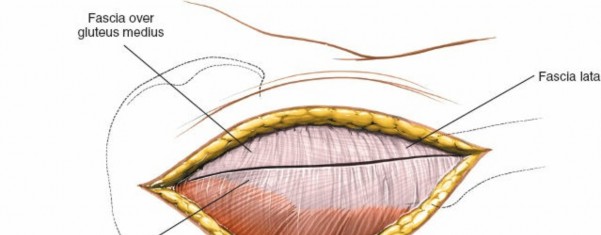
Subcutaneous Dissection
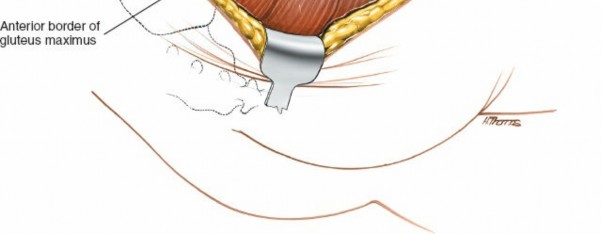
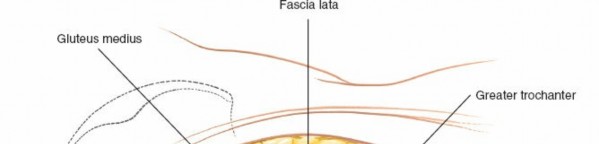
The incision is carried through the skin and subcutaneous tissue. Subcutaneous fat is dissected, and skin flaps are developed as necessary. Careful hemostasis of superficial vessels is maintained. The deep fascia (fascia lata) covering the gluteus maximus is exposed.
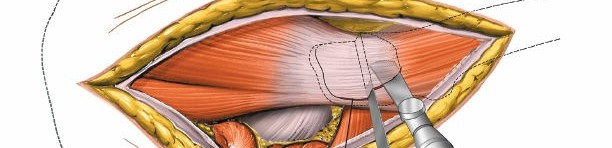
Gluteus Maximus Split
The fibers of the gluteus maximus are separated longitudinally. This muscle receives innervation from the inferior gluteal nerve, which enters its deep surface proximally. Splitting the fibers, rather than transecting them, minimizes muscle damage and preserves function.

The gluteus maximus can be retracted to expose the deeper structures.
Deep Dissection and Internervous Planes
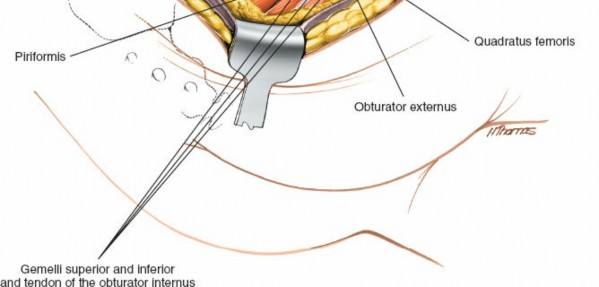
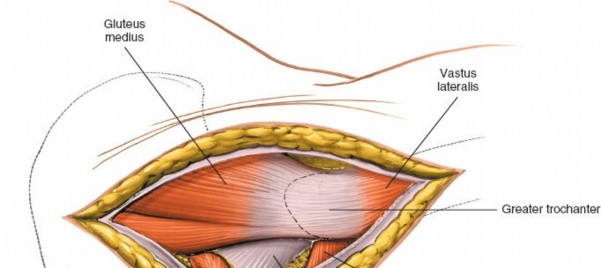
Exposure of Short External Rotators
Deep to the gluteus maximus, the gluteus medius and minimus muscles are encountered superiorly. The short external rotator muscles of the hip are identified. From superior to inferior, these are the piriformis, superior gemellus, obturator internus, inferior gemellus, and quadratus femoris.
Sciatic Nerve Protection
The sciatic nerve is the most critical structure to identify and protect. It typically lies deep to the piriformis muscle, exiting the greater sciatic foramen. It runs inferiorly and laterally, deep to the short external rotators and superficial to the quadratus femoris.
Careful dissection along the inferior border of the piriformis and superior border of the gemelli muscles is performed. The nerve is gently mobilized and protected with a broad, blunt retractor (e.g., a malleable retractor or a specially designed sciatic nerve protector) throughout the procedure. Constant vigilance is maintained to avoid any traction, compression, or direct injury to the nerve.
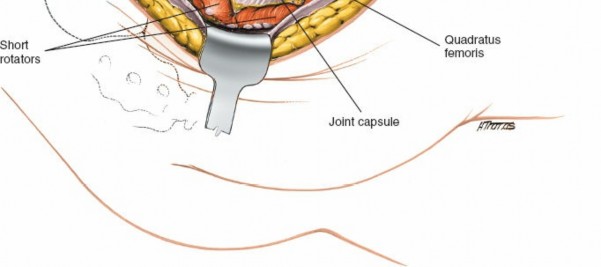
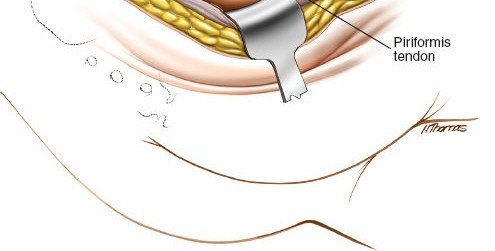
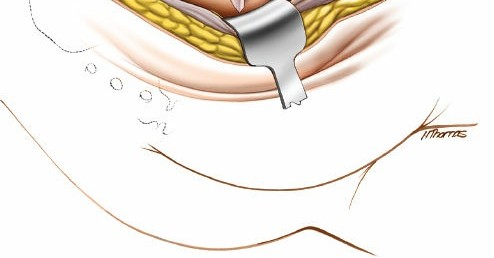
Sectioning of Short External Rotators
To gain direct access to the posterior acetabular wall and capsule, the short external rotators are typically released. The piriformis tendon is often sectioned close to its insertion on the greater trochanter, followed by the superior gemellus, obturator internus tendon, and inferior gemellus. These are tagged with non-absorbable sutures for later repair. The quadratus femoris muscle may also be partially or completely released from its femoral insertion to enhance exposure of the posterior column down to the ischial tuberosity.

Care should be taken during this step to avoid damaging the ascending branch of the medial femoral circumflex artery, which lies deep to the quadratus femoris and supplies the femoral head.
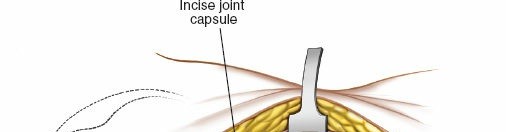
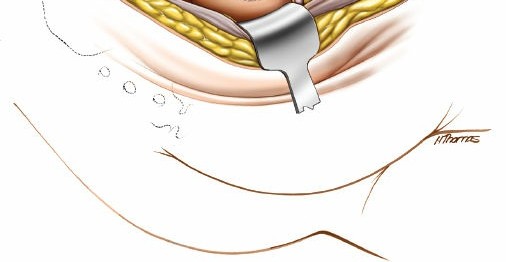
Capsulotomy and Joint Exposure
Once the short external rotators are released and the sciatic nerve is protected, the posterior hip capsule is exposed. A T-shaped or H-shaped capsulotomy is typically performed to visualize the articular surface of the femoral head and acetabulum. The capsular flaps are tagged for later repair. The hip joint can then be dislocated or subluxated posteriorly to gain a more complete view of the fracture lines and articular fragments.
Fracture Reduction Techniques
Achieving anatomical reduction is paramount. This often involves a combination of traction, manipulation, and direct reduction techniques.
Indirect Reduction Maneuvers
- Longitudinal Traction: Applied through the operative limb, often with a traction table or manual traction, to disengage impacted fragments and restore overall length.
- Internal/External Rotation: Manipulating the femoral head can help to realign displaced posterior wall fragments.
- Flexion/Extension: Positioning the hip in different degrees of flexion can tension specific soft tissue structures, aiding in fragment reduction.
Direct Reduction Maneuvers
- Fracture Exploration: Thorough debridement of hematoma and any incarcerated fragments (e.g., bone chips, labrum) is performed.
- Direct Visualization: The fracture lines of the posterior wall and column are identified.
- Reduction Forceps: Pointed reduction clamps (e.g., Jungbluth, Farabeuf) are invaluable for grasping and reducing fragments. For posterior wall fractures, a clamp can be placed from the intact superior acetabular rim to the main posterior wall fragment to reduce it.
- Bone Hooks and Elevators: Small bone hooks or periosteal elevators can be used to lever fragments into position.
- Ball Spike Pushers: These are effective for manipulating larger posterior column fragments.
- Manual Pressure: Digital pressure or external manipulation of the greater trochanter can assist in reducing posterior column fractures.
- Intra-articular Inspection: After preliminary reduction, the hip joint is often gently distracted or subluxated to visually inspect the articular surface for any residual incongruity or incarcerated fragments. Fluoroscopy with various views is used to confirm reduction.
Fixation Strategies
Once anatomical reduction is achieved and maintained, stable internal fixation is performed.
Posterior Wall Fixation
- Lag Screws: For large, simple posterior wall fragments, lag screws perpendicular to the fracture plane can provide excellent compression.
- Buttress Plate: A 3.5mm reconstruction plate is typically contoured and placed along the posterior aspect of the acetabulum, buttressing the reduced posterior wall fragments against the intact acetabular rim. Screws are placed into the ilium superiorly, the ischium inferiorly, and across the fracture fragments. The plate acts as a tension band and a buttress.

- Hardware Placement: Care must be taken to ensure all hardware is extra-articular. Intraoperative fluoroscopy and direct palpation of the articular surface through the capsulotomy are critical to verify screw lengths and positions.
Posterior Column Fixation
- Reconstruction Plates: A 3.5mm or 2.7mm reconstruction plate is contoured to the posterior column, extending from the greater sciatic notch area down to the ischial tuberosity.
- Lag Screws: Lag screws across the column fracture can be supplemented with neutralization plates.
- Positioning: Plates are often placed on the lateral aspect of the column, along the gluteal surface.
- Obturator Oblique View: This fluoroscopic view is essential for confirming plate position and screw length in the posterior column, ensuring screws do not violate the greater sciatic notch or the articular surface.
Associated Fracture Patterns
For complex patterns like transverse or T-type fractures, additional fixation may be needed. A combination of lag screws and plates is often employed. The posterior approach may allow access to both the transverse component and the posterior column/wall.
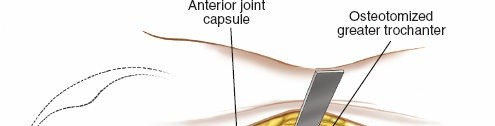
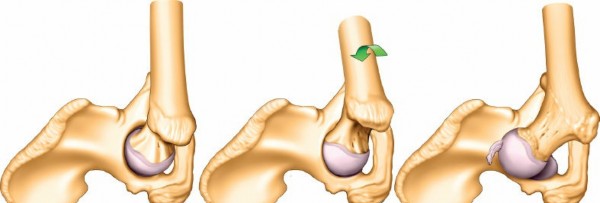
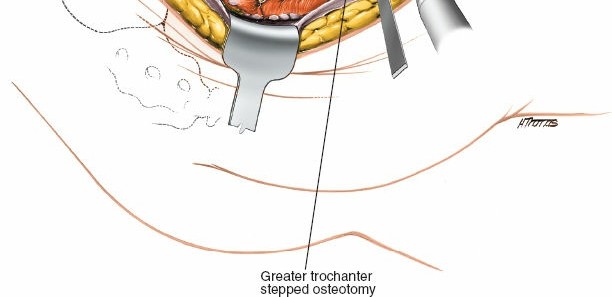
Trochanteric Osteotomy and Surgical Dislocation
For extended exposure, particularly for associated femoral head fractures, dome fractures, or anterior lip fractures that become accessible via a surgical hip dislocation, a trochanteric osteotomy may be performed.
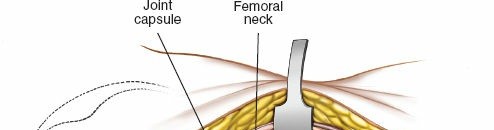
* Technique: A controlled osteotomy of the greater trochanter, typically involving the vastus lateralis insertion, allows superior retraction of the gluteus medius/minimus complex, and access to the joint through the anterior capsule.
* Surgical Dislocation: After osteotomy, the hip can be surgically dislocated anteriorly, providing panoramic visualization of the entire acetabular articular surface and the femoral head. This allows direct inspection and reduction of intra-articular fragments or femoral head chondral lesions.
* Fixation: The osteotomized trochanter is reattached at the end of the procedure, typically with cancellous screws or a tension band wiring technique.

Final Checks and Closure
- Stability Assessment: After fixation, the hip is taken through a full range of motion to ensure stability, especially in cases of posterior wall fractures. Any impingement or instability should prompt re-evaluation of reduction and fixation.
- Fluoroscopy: Final fluoroscopic images (AP, iliac oblique, obturator oblique) are obtained to confirm satisfactory reduction and hardware placement.
- Joint Lavage: The joint is thoroughly irrigated to remove any bone debris or foreign material.
- Capsular Repair: The posterior hip capsule is meticulously repaired.
- Rotator Repair: The sectioned short external rotators are repaired to their origins or insertions.
- Muscle Repair: The gluteus maximus is allowed to fall back into position, and the deep fascia is closed.
- Drainage: A suction drain may be placed in the deep wound, particularly if significant bleeding was encountered.
- Wound Closure: Subcutaneous tissues and skin are closed in layers.


Complications and Management
Acetabular fracture surgery via the posterior approach is associated with several potential complications. Proactive identification and appropriate management are crucial for mitigating adverse outcomes.
Neurological Injury
Sciatic Nerve Injury: This is the most common and feared neurological complication, with an incidence ranging from 5% to 15%, potentially higher in cases with preoperative sciatic nerve palsy.
* Etiology: Direct trauma during dissection, traction injury (especially with prolonged retraction or excessive limb manipulation), compression from hematoma, or iatrogenic hardware placement.
* Prevention: Meticulous identification and protection of the sciatic nerve throughout the procedure. Use of blunt retractors, limiting traction, and avoiding prolonged direct pressure on the nerve. Intraoperative nerve monitoring may be considered for high-risk cases.
* Management: If intraoperative injury is suspected (e.g., sudden drop in nerve conduction during monitoring), the cause must be immediately identified and rectified. Postoperatively, a new or worsened deficit requires immediate investigation (CT to rule out hematoma or screw impingement) and consideration for surgical exploration and nerve repair if a laceration is suspected. Most traction injuries recover partially or fully over time.
Vascular Injury
Injury to the superior or inferior gluteal vessels or branches of the medial femoral circumflex artery can occur, leading to significant hemorrhage.
* Prevention: Careful dissection and meticulous hemostasis. Awareness of vascular anatomy, especially around the sciatic notch.
* Management: Direct ligation or repair of injured vessels. Transfusion may be required.
Infection
Surgical site infection (SSI) rates for acetabular fractures range from 1% to 5%.
* Etiology: Contamination during surgery, prolonged operative time, extensive soft tissue dissection, patient comorbidities.
* Prevention: Strict aseptic technique, prophylactic antibiotics, meticulous soft tissue handling, and adequate wound irrigation.
* Management: Superficial infections can often be managed with antibiotics and wound care. Deep infections typically require surgical debridement, implant retention if stable and infection controlled, or staged removal and revision.
Heterotopic Ossification (HO)
HO, the formation of ectopic bone in soft tissues, is common after acetabular fracture surgery, particularly with the posterior approach, with reported rates as high as 60% without prophylaxis and clinically significant HO in 10-20%.
* Etiology: High-energy trauma, extensive soft tissue dissection, muscle damage, prolonged surgery, certain genetic predispositions.
* Prevention: Prophylactic measures include a single dose of postoperative radiation (7-8 Gy) within 72 hours, or NSAIDs (e.g., indomethacin) for 3-6 weeks postoperatively.
* Management: Clinically significant HO causing pain or range of motion restriction may require surgical excision after skeletal maturity.
Avascular Necrosis (AVN) of the Femoral Head
Incidence ranges from 5% to 15%, significantly higher if there was a traumatic hip dislocation or fracture-dislocation.
* Etiology: Disruption of femoral head blood supply during the initial trauma, particularly with posterior dislocation, or iatrogenic injury to the medial femoral circumflex artery during surgery.
* Prevention: Gentle handling of soft tissues around the femoral neck, meticulous reduction of hip dislocations (within 6 hours if possible), and avoiding excessive capsular stripping.
* Management: Early stages may be managed conservatively. Later stages usually require joint salvage procedures (e.g., core decompression) or total hip arthroplasty.
Post-Traumatic Arthritis (PTA)
This is the most common long-term complication, occurring in 20-50% of patients.
* Etiology: Residual articular incongruity (even small steps or gaps), cartilage damage at the time of injury, infection, AVN, or HO.
* Prevention: Anatomical reduction of the articular surface (ideally <1mm step or gap), stable fixation, and appropriate postoperative rehabilitation.
* Management: Conservative management initially. For symptomatic, advanced PTA, total hip arthroplasty (THA) is the definitive treatment, though it can be technically challenging in post-traumatic settings.
Nonunion or Malunion
Rare in properly fixed acetabular fractures, but possible.
* Etiology: Inadequate reduction, unstable fixation, infection, patient factors (e.g., poor bone quality, smoking).
* Management: Revision surgery with open reduction and internal fixation, bone grafting, or in cases of severe malunion, potentially a salvage THA.
Thromboembolic Events
Deep vein thrombosis (DVT) and pulmonary embolism (PE) are significant risks in pelvic and acetabular trauma patients.
* Prevention: Pharmacological prophylaxis (LMWH, fondaparinux) and mechanical prophylaxis (intermittent pneumatic compression devices) are standard. Early mobilization is also important.
* Management: Anticoagulation for DVT/PE.
| Complication | Typical Incidence | Salvage Strategies / Management |
|---|---|---|
| Sciatic Nerve Injury | 5-15% (up to 30% with pre-op palsy) | Intra-op: Identify and relieve compression. Post-op: Neurological evaluation, imaging (CT/MRI) for hematoma/hardware impingement, nerve conduction studies/EMG. Exploration/repair for severe lesions. Physical therapy. |
| Vascular Injury | <1% | Intra-op: Direct ligation/repair, tamponade. Post-op: Imaging for hematoma, transfusion, embolization for persistent bleeding. |
| Surgical Site Infection | 1-5% | Superficial: Oral/IV antibiotics, wound care. Deep: Surgical debridement, intravenous antibiotics. Implant retention or removal based on stability, organism, and timing. |
| Heterotopic Ossification | Clinical: 10-20% Radiographic: up to 60% | Prophylaxis: Postoperative NSAIDs (e.g., Indomethacin) or single-dose radiation. Symptomatic HO: Surgical excision after maturation (usually 12-18 months). |
| Avascular Necrosis (AVN) | 5-15% (higher with dislocation) | Conservative for early stages. Core decompression, vascularized fibula graft for pre-collapse. Total Hip Arthroplasty (THA) for advanced collapse. |
| Post-Traumatic Arthritis (PTA) | 20-50% | Conservative management (NSAIDs, PT, injections). Activity modification. Total Hip Arthroplasty (THA) for end-stage arthritis causing significant pain and functional impairment. |
| Nonunion/Malunion | Rare (<5%) | Revision ORIF with bone grafting. Corrective osteotomy. Salvage THA if severe deformity or pain and articular destruction. |
| Thromboembolic Events (DVT/PE) | 1-5% (without prophylaxis) | Prophylaxis: Pharmacological (LMWH, Factor Xa inhibitors) and mechanical. DVT: Anticoagulation. PE: Anticoagulation, possibly IVC filter. |
| Hardware Impingement/Prominence | Variable | Revision surgery for hardware removal if symptomatic, or if causing soft tissue irritation or joint impingement. |
Post Operative Rehabilitation Protocols
Postoperative rehabilitation following acetabular fracture fixation via the posterior approach is crucial for optimizing functional outcomes, minimizing complications, and safely returning the patient to activity. Protocols are individualized based on fracture stability, fixation strength, and surgeon preference.
Immediate Postoperative Period (Days 0-7)
- Pain Management: Aggressive multimodal pain management strategies are initiated to facilitate early mobilization and patient comfort.
- Thromboembolism Prophylaxis: Pharmacological (LMWH or oral anticoagulants) and mechanical (foot pumps, pneumatic compression devices) prophylaxis are continued.
- Weight Bearing:
- Non-weight bearing (NWB) on the operative extremity is typically mandated for 8-12 weeks, especially for posterior column fractures or severely comminuted posterior wall fractures, to protect the delicate reduction and fixation construct.
- Toe-touch weight bearing (TTWB) may be initiated earlier (e.g., 6 weeks) for very stable, simple posterior wall fractures.
- Range of Motion (ROM):
- Passive ROM (PROM) exercises within protected ranges are started early to prevent stiffness.
- Active-assisted ROM (AAROM) and gentle Active ROM (AROM), particularly hip flexion and abduction, avoiding extremes of internal rotation and adduction to prevent undue stress on the posterior capsule and repair.
- Hip precautions: Patients are typically instructed to avoid hip flexion beyond 90 degrees, adduction past neutral, and internal rotation to protect the posterior structures. This is particularly critical in cases of repaired posterior wall or column fractures and surgical hip dislocations.
- Mobility: Transfers to and from bed, sitting, and ambulation with appropriate assistive devices (walker or crutches) are initiated under the guidance of physical therapy, strictly adhering to weight-bearing restrictions.
- Wound Care: Monitoring of incision for signs of infection.
Early Rehabilitation Phase (Weeks 2-6)
- Progression of ROM: Gradually increase hip flexion, abduction, and gentle external rotation, while still respecting hip precautions. Avoid forceful stretching.
- Strengthening: Isometric exercises for gluteal muscles (gluteal sets), quadriceps (quad sets), and hamstrings. Progress to gentle isotonic exercises within protected ranges, focusing on hip abductors, extensors, and external rotators.
- Core Stability: Initiation of core strengthening exercises to improve trunk stability.
- Gait Training: Continued non-weight bearing or partial weight bearing gait training, focusing on proper technique and minimizing compensatory movements.
Intermediate Rehabilitation Phase (Weeks 6-12)
- Imaging: Follow-up radiographs are typically obtained around 6-8 weeks to assess fracture healing and hardware integrity.
- Weight Bearing Progression: If radiographic evidence of healing is satisfactory and clinical stability is good, gradual progression to partial weight bearing (PWB) may be allowed, transitioning to full weight bearing (FWB) over several weeks, guided by pain and tolerance.
- Advanced Strengthening: Progress to more challenging isotonic exercises, resistance bands, and light weights. Focus on functional movements.
- Balance and Proprioception: Incorporate exercises to improve balance and proprioception.
- Discontinuation of Hip Precautions: Depending on fracture healing and stability, hip precautions may be gradually relaxed, typically after 8-12 weeks.
Late Rehabilitation and Return to Activity (Months 3+)
- Full Weight Bearing: Generally achieved by 12-16 weeks if healing is adequate.
- Sport-Specific Training: For active individuals, a gradual return to sport-specific activities, focusing on agility, plyometrics, and higher-impact exercises, under the guidance of a physical therapist.
- Functional Progression: Emphasis on restoring full strength, endurance, and flexibility.
- Long-Term Monitoring: Patients are followed for signs of post-traumatic arthritis, heterotopic ossification, or avascular necrosis.
Close communication between the surgeon, physical therapist, and patient is essential to tailor the rehabilitation protocol to individual needs and optimize long-term outcomes. Regular reassessments are necessary to adjust the program based on patient progress and fracture healing status.
Summary of Key Literature and Guidelines
The surgical management of acetabular fractures has been significantly influenced by key literature and established guidelines, primarily driven by the AO Foundation principles of anatomical reduction, stable fixation, preservation of blood supply, and early mobilization. The posterior approach, specifically the Kocher-Langenbeck, remains a foundational technique, supported by decades of clinical experience and outcomes data.
Early seminal works by Judet and Letournel established the anatomical classification of acetabular fractures and detailed surgical approaches, including the posterior approach. Their extensive series demonstrated the correlation between anatomical reduction and improved long-term outcomes, particularly in preventing post-traumatic arthritis. This fundamental principle remains central to modern acetabular fracture surgery.
Current guidelines emphasize the importance of high-quality preoperative imaging, especially 3D CT reconstructions, for accurate fracture characterization and surgical planning. Literature consistently highlights the critical role of timely surgical intervention, especially for irreducible dislocations or those with incarcerated fragments, to minimize the risk of avascular necrosis and improve long-term functional results. While the "golden six-hour rule" for hip dislocation reduction is widely accepted, the optimal timing for definitive fixation of acetabular fractures remains a topic of debate, with many centers favoring early fixation within 5-7 days, provided the patient is physiologically stable.
Studies on the posterior approach specifically report excellent to good results in 70-90% of cases for posterior wall and posterior column fractures, particularly when anatomical reduction (<1mm step-off) is achieved. However, the literature also consistently reports higher rates of heterotopic ossification with the posterior approach, necessitating routine prophylaxis with NSAIDs or single-dose radiation. Sciatic nerve palsy remains a significant concern, with reported incidences varying but generally ranging from 5-15%, often associated with the initial trauma but also with iatrogenic injury.
The development of the extended posterior approaches, such as the trochanteric flip osteotomy, as described by Ganz et al., has expanded the utility of the posterior approach, allowing for surgical hip dislocation and comprehensive visualization of the entire acetabular articular surface and femoral head. This modification is particularly valuable for complex associated injuries, such as femoral head fractures or dome impaction.
In summary, the posterior approach to the acetabulum, as detailed in the original seed content, is an indispensable tool in the orthopedic trauma surgeon's armamentarium. Its efficacy for posterior column and wall fractures is well-established, though meticulous technique, rigorous preoperative planning, and careful management of potential complications are paramount for achieving optimal patient outcomes, in line with modern principles of acetabular fracture management.
Clinical & Radiographic Imaging
You Might Also Like


