
ANKLE DISLOCATIONS WITHOUT FRACTURE
Pathoanatomy and Clinical Evaluation
Dislocations of the tibiotalar joint without an associated fracture of the medial malleolus, lateral malleolus, or the anterior/posterior articular lips of the distal tibia are exceedingly rare clinical entities. The inherent stability of the ankle mortise, dictated by its highly congruent osseous architecture and robust ligamentous complexes, typically dictates that extreme forces result in malleolar fractures rather than pure ligamentous dislocations.
When pure dislocations do occur, they are most frequently the result of high-energy trauma involving extreme plantarflexion combined with either forced inversion or eversion. This mechanism leads to sequential failure of the lateral collateral ligaments (anterior talofibular, calcaneofibular, and posterior talofibular ligaments), the medial deltoid ligament complex, and occasionally the anterior tibiotalar ligaments.
Management Principles
The vast majority of pure ankle dislocations can and should be reduced emergently via closed methods in the emergency department. Reduction is achieved by applying longitudinal traction to the foot with the knee flexed (to relax the gastrocnemius-soleus complex), followed by a reversal of the deforming force.
Clinical Pearl: Posterior dislocation of the fibula behind the tibia (a Bosworth-type equivalent without fracture) may severely impede closed reduction. The fibula becomes entrapped behind the posterolateral tibial ridge, often necessitating urgent open reduction to prevent skin necrosis and neurovascular compromise.
Controversy persists regarding the necessity of acute ligamentous repair in the absence of fracture. Historically, conservative management with cast immobilization has yielded good-to-excellent functional outcomes. However, strict attention must be paid to the distal tibiofibular syndesmosis. If post-reduction weight-bearing radiographs or advanced imaging demonstrate syndesmotic instability or mortise widening, operative intervention via syndesmotic screw or suture-button fixation is absolutely indicated to restore the anatomical mortise and prevent rapid-onset post-traumatic arthrosis.
ACUTE DISLOCATIONS OF THE PATELLA
Biomechanics and Presentation
Acute dislocations of the patella represent a significant disruption of the extensor mechanism, predominantly affecting young, active patients. The patella almost universally dislocates laterally, driven by the dominant force vector of the quadriceps (the Q-angle) and the relatively weaker medial restraints. The primary soft-tissue restraint to lateral patellar translation is the medial patellofemoral ligament (MPFL), which is ruptured in over 90% of acute lateral dislocations.
Patients typically present with a gross deformity, a large hemarthrosis, and severe pain. Closed reduction is the immediate treatment of choice and is often easily accomplished: the hip is flexed, the knee is gently extended, and a medially directed force is applied to the lateral margin of the patella.
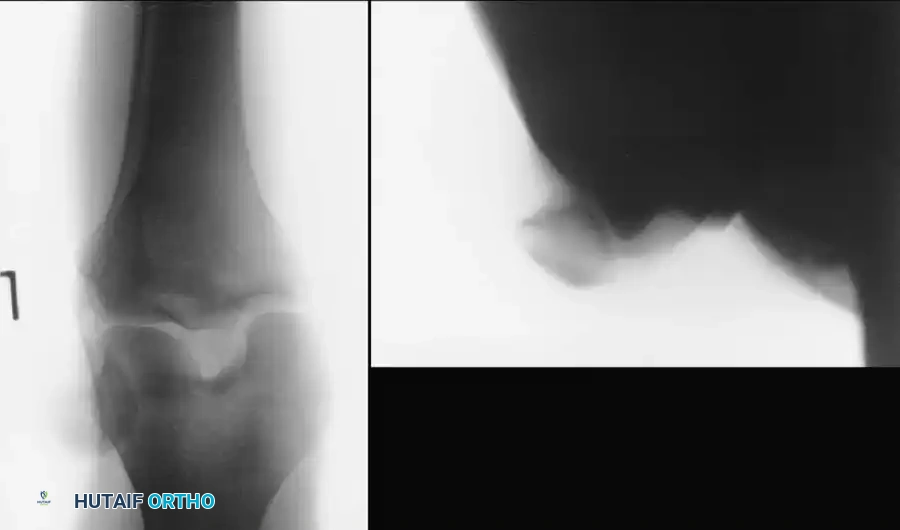
Fig. 57-1 Patellar dislocation. A, Anteroposterior view. B, Sunrise view.
Evidence-Based Evaluation and Imaging
Following reduction, the limb is immobilized in a knee immobilizer or hinged brace locked in extension for 10 to 14 days. Early, controlled range of motion is critical to prevent arthrofibrosis and to stimulate the functional alignment of regenerating collagen fibers along lines of physiological stress.
Radiographic evaluation must be meticulous. Standard anteroposterior, lateral, and axial (sunrise/Merchant) views are mandatory to assess for osteochondral shear fractures. The incidence of these fractures is alarmingly high and frequently underdiagnosed on plain radiography:
* Nietosvaara et al. reported a 39% incidence of osteochondral fractures in a pediatric cohort; 50% were capsular avulsions from the medial patellar margin, and 50% were loose intraarticular fragments sheared from the patella or lateral femoral condyle.
* Stanitski and Paletta documented a 71% incidence of osteochondral or chondral injury in 48 patients, noting that only 32% of these lesions were visible on preoperative radiographs.
Magnetic Resonance Imaging (MRI) has become the gold standard for formulating a definitive management plan. Sallay et al. demonstrated that MRI reveals an effusion in 100% of cases, tears at the femoral insertion of the MPFL in 87%, medial patellar bone bruises in 30%, and increased signal intensity in the vastus medialis obliquus (VMO) in 78%. Arthroscopic correlation confirmed osteochondral lesions in 68% of these patients.
Indications for Operative Intervention
The decision to operate acutely depends heavily on the presence of osteochondral fragments and the patient's baseline anatomical predisposition to instability.
Cash and Hughston stratified patients into two distinct cohorts:
1. Anatomical Predisposition: Patients with lateral hypermobility, VMO dysplasia, patella alta, or a history of instability. Nonoperative treatment yielded only 52% good/excellent results, whereas operative repair yielded 91% good/excellent results.
2. No Predisposition: Patients with normal baseline anatomy achieved 75% good/excellent results with nonoperative management.
These data strongly suggest that patients with a congenital predisposition to dislocation, or those with highly demanding athletic profiles, benefit from acute repair of the disrupted medial structures. Furthermore, Stanitski noted that patients without baseline articular hypermobility suffered a 2.5 times higher frequency of severe articular shear lesions compared to hypermobile patients, as the tighter joint required more force to dislocate.
Surgical Warning: Any displaced osteochondral fragment within the joint space is an absolute indication for acute surgical intervention. The surgeon must remove or fix the loose fragment and concomitantly repair the disrupted medial tissues.
🔪 Surgical Technique 57-1: Open Repair of the Medial Patellar Retinaculum
While arthroscopic techniques for medial retinacular repair exist, the open method remains the gold standard for direct visualization and robust anatomical restoration of the MPFL and VMO.
- Positioning and Setup: Place the patient supine on the operating table. Apply a proximal thigh tourniquet. A lateral post or leg holder may be used to allow dynamic assessment of patellar tracking during the procedure.
- Approach: Utilize a medial parapatellar incision, centered over the palpable defect in the medial retinaculum or the medial epicondyle. Carefully dissect through the subcutaneous tissues to expose the traumatic tear in the medial patellar retinaculum and the VMO.
- Intraarticular Assessment: Perform a formal arthrotomy or utilize prior arthroscopic portals to thoroughly irrigate and explore the knee joint. Systematically inspect the lateral femoral condyle and the medial patellar facet. Remove any unsalvageable loose osteochondral fragments. If a large, weight-bearing osteochondral fragment is identified, consider primary fixation with headless compression screws or bioabsorbable pins.
- Anatomical Repair: Identify the disrupted edges of the vastus medialis muscle belly and the medial patellar retinaculum (specifically the MPFL).
- The Femoral Footprint: Pay meticulous attention to the portion of the VMO and MPFL that originates in the region of the adductor tubercle and medial epicondyle (Schöttle's point). If this origin has been avulsed and retracted proximally, the dynamic angle of insertion into the patella is critically altered. Anatomical reattachment of these fibers to the femoral footprint using suture anchors is vital to preventing recurrent lateral subluxation.
- Closure and Tracking Assessment: Repair the retinacular defect using heavy, non-absorbable or slowly absorbable sutures (e.g., #2 FiberWire or PDS) in an interrupted, pants-over-vest fashion. Before final tying, take the knee through a full range of motion to ensure the patella tracks centrally within the trochlear groove without excessive medial overtightening.
- Final Steps: Deflate the tourniquet, achieve meticulous hemostasis, close the subcutaneous tissues and skin in layers, and apply a sterile dressing and a hinged knee immobilizer locked in extension.
Postoperative Rehabilitation Protocol
- Phase I (0-2 Weeks): The limb is immobilized in extension. Weight-bearing to tolerance with crutches is permitted immediately. Early isometric quadriceps sets and straight-leg raises are initiated to prevent muscle atrophy.
- Phase II (2-6 Weeks): A patellar stabilizing brace (e.g., Palumbo-type) is applied. Controlled, progressive range of motion is initiated to promote organized collagen healing. Crutches are discontinued once the patient demonstrates a normal, pain-free gait without an extensor lag.
- Phase III (6-12 Weeks): Focus shifts to aggressive quadriceps and core strengthening. Stiff-legged resistance exercises are preferred initially.
Pitfall: Avoid full range of motion open-chain knee extension exercises against heavy resistance during early rehabilitation, as this places excessive shear forces on the healing patellofemoral joint and medial repairs.
- Return to Play: Return to full athletic activity is permitted only when objective isokinetic testing demonstrates quadriceps strength at least 90% of the contralateral, uninvolved limb, typically around 4 to 6 months postoperatively.
INTRAARTICULAR DISLOCATIONS OF THE PATELLA
Pathoanatomy
Intraarticular dislocations of the patella are exceptionally rare and represent a severe disruption of the extensor mechanism. They are broadly classified into two distinct horizontal types:
1. Superior Pole Detachment (Most Common): The patella undergoes a horizontal intraarticular dislocation with detachment of the quadriceps tendon. The patella rotates on its horizontal axis such that its articular surface is directed inferiorly toward the tibial plateau.
2. Inferior Pole Detachment: The patella dislocates horizontally, but the inferior pole is avulsed from the patellar tendon. The patella rotates such that its articular surface faces proximally toward the femur.

Fig. 57-2 Intraarticular horizontal dislocation of patella. Quadriceps mechanism usually remains intact. (From Brady TA, Russell D: Interarticular horizontal dislocation of the patella. A case report, J Bone Joint Surg 47A:1393, 1965.)
These complex dislocations are notoriously difficult to reduce via closed manipulation due to the mechanical block created by the rotated patella wedged within the intercondylar notch. Open reduction and formal repair of the extensor mechanism are almost universally required.
🔪 Surgical Technique 57-2: Open Reduction of Intraarticular Patellar Dislocation
- Approach: Utilize a standard midline or medial parapatellar incision. Dissect down to the extensor mechanism to expose the dislocated patella, which is typically found firmly wedged within the intercondylar notch of the femur.
- Reduction: Carefully lever the patella out of the notch. Avoid excessive force that could cause iatrogenic chondral damage to the femoral condyles.
- Joint Debridement: Thoroughly inspect the intraarticular space. Copiously irrigate the joint and remove any loose osteochondral or cartilaginous fragments generated during the dislocation.
- Extensor Mechanism Repair: Replace the patella into its anatomical bed. Depending on the type of dislocation, reattach the avulsed quadriceps tendon or patellar tendon.
- Technique: Utilize heavy, non-absorbable sutures (e.g., #5 Ethibond or #2 FiberWire). Passing the sutures through longitudinal transosseous tunnels drilled through the patella provides the most biomechanically secure repair. Krackow locking stitches should be used in the tendon ends.
- Closure: Repair the medial and lateral retinacula to ensure watertight closure and balanced tracking. Close the wound in layers.
Aftertreatment: The postoperative protocol mirrors that of an acute lateral dislocation repair, though progression of flexion may be slightly delayed to protect the transosseous extensor mechanism repair.
ACUTE KNEE DISLOCATIONS (TIBIOFEMORAL)
The Orthopaedic Emergency
Tibiofemoral knee dislocations—whether anterior, posterior, medial, lateral, or posterolateral—are true orthopaedic emergencies. They are characterized by catastrophic, multi-ligamentous damage (typically involving both cruciate ligaments and at least one collateral complex) and carry a devastating potential for limb-threatening vascular complications.
Vascular and Neurological Assessment
Prompt evaluation and early repair of vascular damage are universally mandated. The incidence of popliteal artery injury in knee dislocations is highly variable but alarmingly common, ranging from 21% (Sisk and King) to 40% (Shields, Mital, and Cave).
Surgical Warning: The presence of a warm foot does NOT rule out a popliteal artery injury. Kennedy famously reported observing a patient's foot remaining warm and well-perfused via collateral circulation while a massive thrombus was actively forming in the popliteal artery.
While some trauma centers rely on Ankle-Brachial Indices (ABI < 0.9) to screen for vascular injury, formal CT angiography or conventional arteriography is strongly recommended for any knee dislocation that required reduction, regardless of pedal pulses.
Ischemic Time is Critical:
* Arterial repair performed within 6 to 8 hours of injury yields the best limb salvage rates, with an amputation rate of approximately 11%.
* If revascularization is delayed beyond 8 hours, the amputation rate skyrockets to 86%.
* Danger signals demanding immediate vascular exploration include: absent pedal pulses; expanding popliteal hematoma; severe popliteal tenderness; and a cold, cyanotic extremity. Continued observation in the face of these signs inevitably leads to disaster.
Neurological injuries, particularly to the common peroneal nerve, occur in 16% to 43% of knee dislocations. The prognosis for functional recovery of a complete peroneal nerve palsy is highly guarded. Meyers et al. noted that 12 out of 14 patients with peroneal nerve injuries had no return of function at long-term follow-up.
Initial Management and Temporization
Acute knee dislocations can usually be reduced satisfactorily in the emergency department via closed longitudinal traction. Following reduction:
1. Aspirate the massive hemarthrosis under strict sterile technique to relieve capsular tension and pain.
2. Immobilize the knee in full extension using a well-padded rigid splint or brace.
3. Admit the patient for continuous, serial neurovascular monitoring for a minimum of 5 to 7 days.
4. In cases of profound instability where the joint cannot be maintained in a reduced position in a splint, temporary external fixation or the placement of a large transarticular Steinmann pin through the intercondylar notch of the tibia into the femur may be required to protect the neurovascular bundle until definitive multi-ligamentous reconstruction can be performed.
📚 Medical References
- Patellar dislocation following total knee replacement, J Bone Joint Surg 67A:1321, 1985.
- Mont MA, Waldman B, Banerjee C, et al: Multiple irrigation, debridement, and retention of components in infected total knee arthroplasty, J Arthroplasty 12:426, 1997.
- Murdock LE, Hofmann AA, Friedman R, et al: The role of duplex ultrasonography in the detection of deep-vein thrombosis in asymptomatic, postoperative total hip and knee arthroplasty patients, Orthop Trans 16:710, 1992.
- Nazarian DG, Booth Jr RE: Extensor mechanism allografts in total knee arthroplasty, Clin Orthop Relat Res 367:123, 1999.
- Ortiguera CJ, Berry DJ: Patellar fracture after total knee arthroplasty, J Bone Joint Surg 84A:532, 2002.
- Rand JA, Morrey BF, Bryan RS: Patellar tendon rupture after total knee arthroplasty, Clin Orthop Relat Res 244:233, 1989.
- Ritter MA, Keating EM, Faris PM, et al: Rush rod fi xation of supracondylar fractures above total knee arthroplasties, J Arthroplasty 10:213, 1995.
- Ritter MA, Pierce MJ, Zhou H, et al: Patellar complications (total knee arthroplasty), Clin Orthop Relat Res 367:149, 1999.
- Ritter MA, Thong AE, Keating EM, et al: The effect of femoral notching during total knee arthroplasty on the prevalence of postoperative femoral fractures and on clinical outcome, J Bone Joint Surg 87A:2411, 2005.
- Rorabeck CH, Angliss RD, Lewis PL: Fractures of the femur, tibia, and patella after total knee arthroplasty: decision making and principles of management, Instr Course Lect 47:449, 1998.
- Rosenberg AG, Andriacchi TP, Barden R, et al: Patellar component failure in cementless total knee arthroplasty, Clin Orthop Relat Res 238:106, 1988.
- Rosenberg AG, Haas B, Barden R, et al: Salvage of infected total knee arthroplasty, Clin Orthop Relat Res 226:31, 1988.
- Salvati EA, Robinson RP, Zeno SM, et al: Infection rates after 3175 total hip and total knee replacements performed with and without a horizontal unidirectional fi ltered air-fl ow system, J Bone Joint Surg 64A:525, 1982.
- Scher DM, Pak K, Lonner JH, et al: The predictive value of indium 111 leukocyte scans in the diagnosis of infected total hip, knee, or resection arthroplasties, J Arthroplasty 15:295, 2000.
- Schoifet SD, Morrey BF: Treatment of infection after total knee arthroplasty by debridement with retention of the components, J Bone Joint Surg 72A:1383, 1990.
- Segreti J, Nelson JA, Trenholme GM: Prolonged suppressive antibiotic therapy for infected orthopedic prosthesis, Clin Infect Dis 27:711, 1998.
- Silva M, Tharani R, Schmalzried TP: Results of direct exchange or debridement of the infected total knee arthroplasty, Clin Orthop Relat Res 404:125, 2002.
- Stulberg SD, Stulberg BN, Hamati Y, et al: Failure of mechanisms of metal-backed patellar components, Clin Orthop Relat Res 236:88, 1988.
- Teller RE, Christie MJ, Martin W, et al: Sequential indiumlabeled leukocyte and bone scans to diagnose prosthetic joint infection, Clin Orthop Relat Res 373:241, 2000.
- Thompson NW, Wilson DS, Cran GW, et al: Dislocation of the rotating platform after low contact stress total knee arthroplasty, Clin Orthop Relat Res 425:207, 2004.
- Tremaine MD, Choroszy CJ, Gordon GH, et al: Diagnosis of deep venous thrombosis by compression ultrasound in knee arthroplasty patients, J Arthroplasty 7:187, 1992.
- Vernace JV, Rothman RH, Booth RE, et al: Arthroscopic management of the patellar clunk syndrome following posterior stabilized total knee arthroplasty, J Arthroplasty 4:179, 1989.
- Waldman BJ, Hostin E, Mont MA, et al: Infected total knee arthroplasty treated with arthroscopic irrigation and debridement, J Arthroplasty 15:430, 2000.
- Westrich GH, Haas SB, Mosca P, et al: Meta-analysis of thromboembolic prophylaxis after total knee arthroplasty, J Bone Joint Surg 82B:795, 2000.
- Westrich GH, Menezes A, Sharrock N, et al: Thromboembolic disease prophylaxis in total knee arthroplasty using intraoperative heparin and postoperative pneumatic foot compression, J Arthroplasty 14:651, 1999.
- Westrich GH, Sculco TP: Prophylaxis against deep venous thrombosis after total knee arthroplasty: pneumatic plantar compression and aspirin compared with aspirin alone, J Bone Joint Surg 78A:826, 1996.
- White J, Kelly M, Dunsmuir R: C-reactive protein level after total hip and total knee replacement, J Bone Joint Surg 80B:909, 1998.
- Wilson MG, Kelley K, Thornhill TS: Infection as a complication of total knee-replacement arthroplasty, J Bone Joint Surg 72A:878, 1990.
- Wilson MG, Pei LF, Malone KM, et al: Fixed low-dose versus adjusted higher-dose warfarin following orthopedic surgery: a randomized prospective trial, J Arthroplasty 9:127, 1994.
- Windsor RE, Insall JN, Urs WK, et al: Two-stage reimplantation for the salvage of total knee arthroplasty complicated by infection, J Bone Joint Surg 72A:272, 1990.
- Woolson ST, Pottorff G: Venous ultrasonography in the detection of proximal vein thrombosis after total knee arthroplasty, Clin Orthop Relat Res 273:131, 1991.
- Woolson ST, Robinson RK, Khan NQ, et al: Deep venous thrombosis prophylaxis for knee replacement: warfarin and pneumatic compression, Am J Orthop 27:299, 1998.
- Revision Total Knee Arthroplasty Babis GC, Trousdale RT, Morrey BF: The effectiveness of isolated tibial insert exchange in revision total knee arthroplasty, J Bone Joint Surg 84A:64, 2002.
- Barrack RL, Jennings RW, Wolfe MW, et al: The value of preoperative aspiration before total knee revision, Clin Orthop Relat Res 345:8, 1997.
- Barrack RL, Rorabeck C, Burt M, et al: Pain at the end of the stem after revision total knee arthroplasty, Clin Orthop Relat Res 367:216, 1999.
- Barrack RL, Smith P, Munn B, et al: Comparison of surgical approaches in total knee arthroplasty, Clin Orthop Relat Res 356:16, 1998.
- Berger RA, Rubash HE, Seel MJ, et al: Determining the rotational alignment of the femoral component in total knee arthroplasty using the epicondylar axis, Clin Orthop Relat Res 286:40, 1993.
- Bertin KC, Freeman MAR, Samuelson KM, et al: Stemmed revision arthroplasty for aseptic loosening of total knee replacement, J Bone Joint Surg 67B:242, 1985.
- Booth RE Jr, Lotke PA: The results of spacer block technique in revision of infected total knee arthroplasty, Clin Orthop Relat Res 248:57, 1989.
- Bourne RB, Crawford HA: Principles of revision total knee arthroplasty, Orthop Clin North Am 29:331, 1998.
- Bradley GW: Revision total knee arthroplasty by impaction bone grafting, Clin Orthop Relat Res 371:113, 2000.
- Brand MG, Daley RJ, Ewald F, et al: Tibial tray augmentation with modular metal wedges for tibial bone stock defi ciency, Clin Orthop Relat Res 248:71, 1989.
- Callahan CM, Drake BG, Heck DA, et al: Patient outcomes following unicompartmental or bicompartmental knee arthroplasty: a meta-analysis, J Arthroplasty 10:141, 1995.
- Coonse K, Adams JD: A new operative approach to the knee joint, Surg Gynecol Obstet 77:344, 1943.
- Coyte PC, Hawker G, Croxford R, et al: Rates of revision knee replacement in Ontario, Canada, J Bone Joint Surg 81A:773, 1999.
- Dennis DA: Structural allografting in revision total knee arthroplasty, Orthopedics 17:849, 1994.
- Dolin MG: Osteotomy of the tibial tubercle in total knee replacement, J Bone Joint Surg 65A:704, 1983.
- Ecker ML, Lotke PA, Windsor RE, et al: Long-term results after total condylar knee arthroplasty: signifi cance of radiolucent lines, Clin Orthop Relat Res 216:151, 1987.
- Ellingsen DE, Rand JA: Intramedullary arthrodesis of the knee after failed total knee arthroplasty, J Bone Joint Surg 76A:870, 1994.
- Engh GA, Ammeen DJ: Bone loss with revision total knee arthroplasty: defect classifi cation and alternatives for reconstruction, Instr Course Lect 48:167, 1999.
- Engh GA, Koralewicz LM, Pereles TR: Clinical results of modular polyethylene insert exchange with retention of total knee arthroplasty components, J Bone Joint Surg 82A:516, 2000.
- Fehring TK, Griffi n WL: Revision of failed cementless total knee implants with cement, Clin Orthop Relat Res 356:34, 1998.
- Fehring TK, McAvoy G: Fluoroscopic evaluation of the painful total knee arthroplasty, Clin Orthop Relat Res 331:226, 1996.
- Fehring TK, Valadie AL: Knee instability after total knee arthroplasty, Clin Orthop Relat Res 299:157, 1994.
- Friedman RJ, Poss R: Revision total knee arthroplasty in patients with osteoarthritis, Rheum Dis Clin North Am 14:537, 1988.
- Goldberg VM, Figgie MP, Figgie HE III, et al: The results of revision total knee arthroplasty, Clin Orthop Relat Res 226:86, 1988.
- Gustilo T, Comadoll JL, Gustilo RB: Long-term results of 56 revision total knee replacements, Orthopedics 19:98, 1996.
- Haas SB, Insall JN, Montgomery W III, et al: Revision total knee arthroplasty with use of modular components with stems inserted without cement, J Bone Joint Surg 77A:1700, 1995.
- Hanssen AD: Bone-grafting for severe patellar bone loss during revision knee arthroplasty, J Bone Joint Surg 83A:171, 2001.
- Insall JN, Thompson FM, Brause BD: Two-stage reimplantation for the salvage of infected total knee arthroplasty, J Bone Joint Surg 65A:1087, 1983.
- Jeffery RS, Orton MA, Denham RA: Wedged tibial components for total knee arthroplasty, J Arthroplasty 9:381, 1994.
- Karbowski A, Eckardt A, Schwitalle M, et al: Revision resurfacing knee arthroplasty for aseptic loosening, Arch Orthop Trauma Surg 117:256, 1998.
- Kurtz S, Mowat F, Ong K, et al: Prevalence of primary and revision total hip and knee arthroplasty in the United States from 1990 through 2002, J Bone Joint Surg 87A:1487, 2005.
- McAuley JP, Engh GA, Ammeen DJ: Treatment of the unstable total knee arthroplasty, Instr Course Lect 53:237, 2004.
- Meek RM, Greidanus NV, McGraw RW, et al: The extensile rectus snip exposure in revision of total knee arthroplasty, J Bone Joint Surg 85B:1120, 2003.
- Murray PB, Rand JA, Hanssen AD: Cemented long-stem revision total knee arthroplasty, Clin Orthop Relat Res 309:116, 1994.
- Nelson CL, Lonner JH, Lahiji A, et al: Use of a trabecular metal patella for marked patella bone loss during revision total knee arthroplasty, J Arthroplasty 18(7 suppl 1):37, 2003.
- Pagnano MW, Trousdale RT, Rand JA: Tibial wedge augmentation for bone defi ciency in total knee arthroplasty: a follow-up study, Clin Orthop Relat Res 321:151, 1995.
- Partington PF, Sawhney J, Rorabeck CH, et al: Joint line restoration after revision total knee arthroplasty, Clin Orthop Relat Res 367:165, 1999.
- Peters CL, Hennessey R, Barden RM, et al: Revision total knee arthroplasty with a cemented posterior-stabilized or constrained condylar prosthesis, J Arthroplasty 12:896, 1997.
- Rand JA: Bone defi ciency in total knee arthroplasty: use of metal wedge augmentation, Clin Orthop Relat Res 271:63, 1991.
- Rand JA: Modular augments in revision total knee arthroplasty, Orthop Clin North Am 29:347, 1998.
- Ritter MA: Screw and cement fi xation of large defects in total knee arthroplasty, J Arthroplasty 1:125, 1986.
- Scott RD, Siliski JM: The use of a modifi ed V-Y quadricepsplasty during total knee replacement to gain exposure and improve fl exion in the ankylosed knee, Orthopedics 8:45, 1985.
- Sculco TP, Choi JC: The role and results of bone grafting in revision total knee replacement, Orthop Clin North Am 29:339, 1998.
- Smith PN, Parker DA, Gelinas J, et al: Radiographic changes in the patella following quadriceps turndown for revision total knee arthroplasty, J Arthroplasty 19:714, 2004.
- Stuart MJ, Larson JE, Morrey BF: Reoperation after condylar revision total knee arthroplasty, Clin Orthop Relat Res 286:168, 1993.
- Trousdale RT, Hanssen AD, Rand JA, et al: V-Y quadricepsplasty in total knee arthroplasty, Clin Orthop Relat Res 286:48, 1993.
- Whaley AL, Trousdale RT, Rand JA, et al: Cemented long-stem revision total knee arthroplasty, J Arthroplasty 18:592, 2003.
- Whiteside LA, Ohl MD: Tibial tubercle osteotomy for exposure of the diffi cult total knee arthroplasty, Clin Orthop Relat Res 260:6, 1990.
- Windsor RE, Insall JN: Exposure in revision total knee arthroplasty: the femoral peel, Tech Orthop 3:1, 1988.
- Windsor RE, Insall JN, Urs WK, et al: Two-stage reimplantation for the salvage of total knee arthroplasty complicated by infection, J Bone Joint Surg 72A:272, 1990.
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding ankle-2