Optimizing Orthopaedic Analgesia: Key Strategies for Relief

Key Takeaway
In this comprehensive guide, we discuss everything you need to know about Optimizing Orthopaedic Analgesia: Key Strategies for Relief. Orthopaedic analgesia orthopaedic involves comprehensive pain management strategies for orthopaedic conditions. It utilizes pharmacological agents like local anesthetics, which block voltage-gated sodium channels to prevent nerve impulses, alongside opioids and sedatives. These interventions ensure effective pain relief, promoting patient comfort and facilitating recovery in an orthopaedic setting.
Introduction and Epidemiology
Orthopaedic surgery inherently involves significant tissue trauma, osseous resection, and nerve manipulation, resulting in profound nociceptive and neuropathic pain profiles. The optimization of orthopaedic analgesia has evolved significantly from traditional opioid-centric monotherapy to sophisticated, multimodal, opioid-sparing pathways. This paradigm shift is driven by the imperative to facilitate Enhanced Recovery After Surgery (ERAS) protocols, minimize opioid-related adverse events, and mitigate the risk of chronic opioid dependence, which remains a critical epidemiological concern in the post-operative orthopaedic population.
The contemporary approach to orthopaedic analgesia requires a comprehensive understanding of neuropharmacology, regional anesthesia, and systemic pain modulation. The fundamental classes of analgesic agents utilized in orthopaedic practice include local anesthetics, vasoconstrictors, opioids, non-steroidal anti-inflammatory drugs (NSAIDs), gabapentinoids, and sedatives such as benzodiazepines. By leveraging synergistic mechanisms of action across the peripheral and central nervous systems, orthopaedic surgeons can achieve superior pain relief, reduce the incidence of post-operative nausea and vomiting (PONV), and accelerate functional rehabilitation.
Surgical Anatomy and Biomechanics
To effectively optimize orthopaedic analgesia, a rigorous understanding of the neuroanatomy and the pharmacodynamic biomechanics of analgesic agents is required. Pain transmission involves transduction at the peripheral nociceptor, transmission along afferent nerve fibers, modulation within the dorsal horn of the spinal cord, and perception in the cerebral cortex.
Neuroanatomy of Peripheral Nerve Fibers
Peripheral nerves are composed of various fiber types, each exhibiting distinct sensitivities to local anesthetics based on their diameter, myelination status, and firing frequency. Local anesthetics act by reversibly binding to the intracellular portion of voltage-gated sodium channels in the axonal membrane, thereby preventing the influx of sodium necessary for action potential propagation.

The blockade is most effective in smaller, myelinated fibers that fire at high frequencies. Consequently, the clinical progression of a neural blockade follows a predictable sequence. Pain and temperature fibers (A-delta and unmyelinated C fibers) are highly sensitive and are blocked first. Pressure and touch fibers (A-beta) follow, while the larger, heavily myelinated motor and proprioceptive fibers (A-alpha) are the most resistant to blockade. This differential sensitivity allows for the clinical phenomenon of sensory-motor dissociation, wherein analgesia can be achieved while preserving motor function—a critical advantage for post-operative ambulation and rehabilitation.
Pharmacodynamics of Local Anesthetics
Local anesthetics are broadly classified into amides (e.g., lidocaine, bupivacaine, ropivacaine) and esters (e.g., procaine, tetracaine) based on their intermediate chain linkage. In orthopaedic practice, amides are predominantly utilized due to their stable shelf life and lower incidence of allergic reactions.
- Lidocaine: A short-acting, highly potent agent with rapid tissue penetration. It is the most widely utilized local anesthetic for local infiltration, regional blocks, spinal, and epidural anesthesia.
- Bupivacaine: A slower-onset, highly potent, and longer-lasting agent compared to lidocaine. By altering the concentration, clinicians can effectively separate motor and sensory blockade. However, it carries an increased risk of cardiac toxicity.
- Ropivacaine: Structurally similar to bupivacaine but formulated as a pure S-enantiomer. It provides comparable analgesic characteristics but is considered a "safer" alternative due to a significantly lower incidence of severe cardiotoxicity.
Neuropharmacology of Opioids
Opioids, derived historically from the seed of the opium poppy (Papaver somniferum), include naturally occurring alkaloids like morphine and codeine, as well as synthetic derivatives. These agents exert their effects by binding to specific G-protein coupled opioid receptors in the central nervous system, primarily the mu ($/mu$), delta ($/delta$), and kappa ($/kappa$) receptors.
The $/mu$-receptor is the primary mediator of opioid-induced analgesia. Activation of this receptor occurs both presynaptically (inhibiting the release of excitatory neurotransmitters like substance P and glutamate) and postsynaptically (hyperpolarizing the neuron via potassium channel efflux). Furthermore, $/mu$-receptor activation inhibits $/gamma$-aminobutyric acid (GABA)-ergic interneurons in the midbrain periaqueductal gray, disinhibiting descending pain inhibitory pathways that modulate nociceptive signals at the level of the spinal cord.
Indications and Contraindications
The selection of an analgesic modality depends on the surgical site, anticipated tissue trauma, patient comorbidities, and the planned rehabilitation trajectory. Multimodal analgesia is universally indicated for major orthopaedic procedures unless specific contraindications exist.
Indications for Regional and Systemic Analgesia
Regional anesthesia (neuraxial blocks, peripheral nerve blocks) is highly indicated for procedures such as total joint arthroplasty, major ligamentous reconstruction, and complex fracture fixation. Systemic opioids are indicated for breakthrough nociceptive pain but should be titrated judiciously. Vasoconstrictors, primarily epinephrine, are indicated as adjuncts to local anesthetics to prolong the duration of the blockade by decreasing local blood flow, which simultaneously minimizes systemic absorption and reduces local surgical site bleeding.
Contraindications and Anatomical Considerations
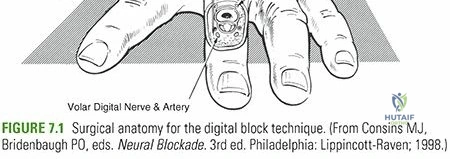
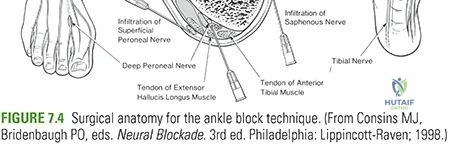
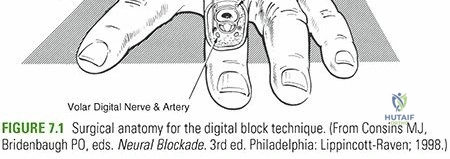
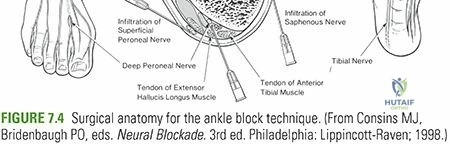
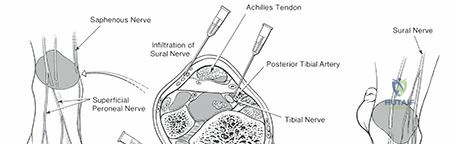
The addition of epinephrine to local anesthetics carries specific contraindications. The classic surgical mnemonic dictates that epinephrine should not be used in areas with terminal vasculature: "nose, hose (penis), fingers, toes." Therefore, epinephrine-containing solutions are traditionally contraindicated for digital blocks, Bier blocks (intravenous regional anesthesia), and ankle blocks, although recent hand surgery literature has challenged the absolute nature of the digital block contraindication in healthy patients. Phenylephrine is occasionally utilized as an alternative vasoconstrictor, primarily in spinal anesthesia formulations.
| Analgesic Modality | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Local Infiltration Analgesia (LIA) | Total knee/hip arthroplasty, soft tissue mass excision, minor fracture fixation. | Documented allergy to amide/ester anesthetics, active local infection at the injection site. | Severe hepatic dysfunction (for amide anesthetics). |
| Peripheral Nerve Blocks | Upper/lower extremity trauma, arthroscopy, joint replacement. | Patient refusal, localized infection, compartment syndrome risk (masks symptoms). | Pre-existing peripheral neuropathy, coagulopathy. |
| Systemic Opioids | Moderate to severe acute post-operative breakthrough pain. | Concurrent use of monoamine oxidase inhibitors (MAOIs), severe respiratory depression. | Obstructive sleep apnea, history of substance use disorder, severe renal impairment. |
| Epinephrine Adjunct | Prolongation of local anesthetic effect, hemostasis in surgical fields. | Intravenous regional anesthesia (Bier block), digital blocks (classic teaching). | Severe peripheral vascular disease, uncontrolled hypertension. |
Pre Operative Planning and Patient Positioning
Pre-operative planning for orthopaedic analgesia begins in the pre-admission testing clinic. The goal is to establish a preemptive analgesic foundation that alters peripheral and central sensitization before the surgical incision is made.
Preemptive Multimodal Protocols
Preemptive analgesia typically involves the administration of oral agents 1 to 2 hours prior to surgery. A standard orthopaedic pre-operative cocktail may include:
* Acetaminophen: 1000 mg PO (central cyclooxygenase inhibition).
* Gabapentinoids: Gabapentin 300-600 mg PO or Pregabalin 50-75 mg PO (modulates voltage-gated calcium channels, reducing neuropathic pain and central sensitization).
* NSAIDs: Celecoxib 200-400 mg PO (selective COX-2 inhibition to reduce peripheral prostaglandin synthesis without impairing platelet function).

Patient Positioning for Regional Analgesia
Patient positioning is critical for the safe and efficacious administration of regional anesthetic blocks.
* Neuraxial Anesthesia: For spinal or epidural placement, the patient is typically placed in the lateral decubitus position with the knees flexed to the chest, or seated on the edge of the operating table with the lumbar spine maximally flexed to open the interlaminar spaces.
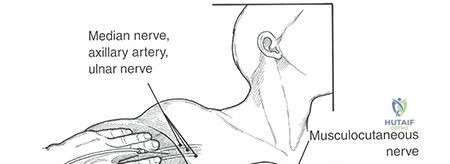
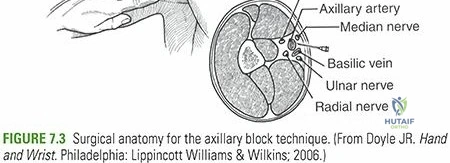
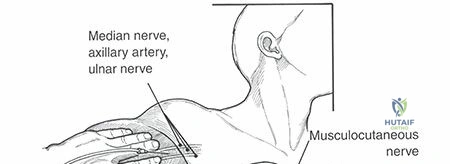
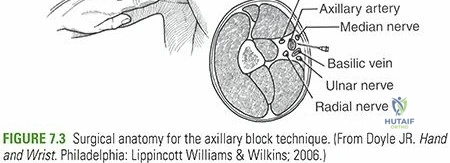
* Upper Extremity Blocks: Interscalene and supraclavicular blocks are performed with the patient supine, head turned to the contralateral side, and the ipsilateral arm adducted.
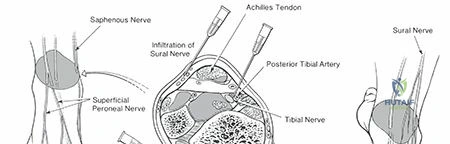
* Lower Extremity Blocks: Femoral and fascia iliaca blocks require the patient to be supine. Popliteal sciatic blocks are optimally performed in the prone or lateral decubitus position to allow adequate access to the posterior thigh.
Detailed Surgical Approach and Technique
The administration of orthopaedic analgesia requires precise technique, meticulous calculation of weight-based dosing, and strict adherence to safety protocols to prevent systemic toxicity.
Local Anesthetic Dosing and Calculations
Surgeons must be intimately familiar with the maximal safe doses of commonly used local anesthetics to prevent iatrogenic toxicity.
* Lidocaine: Maximum dose is 5 mg/kg (7 mg/kg if combined with epinephrine).
* Bupivacaine: Maximum dose is 1.5 mg/kg (3 mg/kg if combined with epinephrine).
Calculation Example for Pediatric Patient:
To determine the allowable volume of 1% lidocaine without epinephrine for a 30-kg child:
1. Convert percentage to concentration: Percent concentration × 10 = mg/mL. Therefore, 1% lidocaine = 10 mg/mL.
2. Calculate maximum total dose: 5 mg/kg × 30 kg = 150 mg allowed.
3. Calculate allowable volume: 150 mg ÷ 10 mg/mL = 15 mL of 1% lidocaine.
Technique Local Infiltration Analgesia
Local Infiltration Analgesia (LIA) has become the gold standard for periarticular pain management in total knee and total hip arthroplasty. The technique involves the systematic injection of a high-volume, dilute local anesthetic cocktail directly into the surgical tissues.
- Preparation: A standard LIA cocktail typically contains ropivacaine or bupivacaine, epinephrine, ketorolac, and normal saline to achieve a volume of 100-120 mL.
- Posterior Capsule Injection: Prior to component implantation, the posterior capsule and collateral ligaments are infiltrated, taking care to avoid direct injection into the neurovascular bundle (e.g., popliteal vessels and tibial nerve).
- Periosteal and Retinacular Infiltration: Following component seating, the periosteum, deep fascial layers, and extensor retinaculum are infiltrated.
- Subcutaneous Infiltration: The final volume is distributed into the subcutaneous adipose tissue prior to final skin closure.
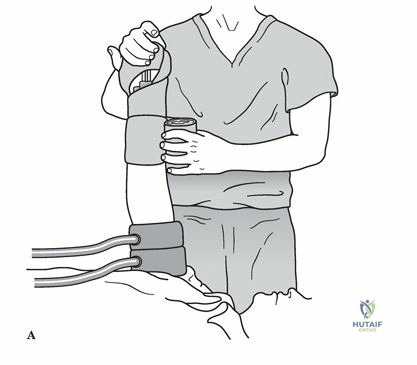
Intravenous Regional Anesthesia Bier Block
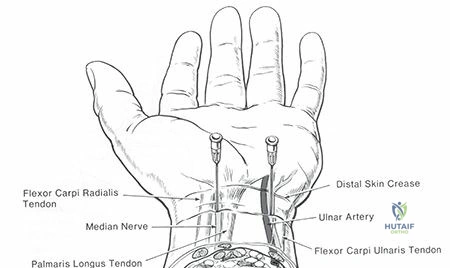
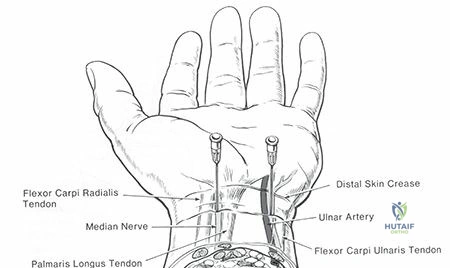
The Bier block is a highly effective technique for short-duration procedures of the distal upper extremity, such as closed reduction of distal radius fractures or carpal tunnel release.
1. Preparation: An intravenous cannula is placed in the dorsum of the operative hand.
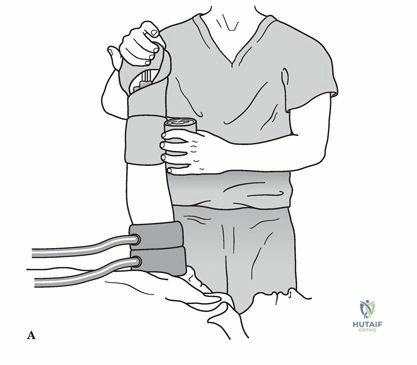
2. Exsanguination: The limb is elevated and exsanguinated using an Esmarch bandage.
3. Tourniquet Inflation: A double pneumatic tourniquet is applied to the proximal arm. The proximal cuff is inflated to 250 mmHg (or 100 mmHg above systolic pressure).
4. Injection: 40-50 mL of 0.5% lidocaine (strictly without epinephrine) is injected slowly. Analgesia is achieved within 5 minutes.
5. Tourniquet Management: If tourniquet pain develops, the distal cuff (now overlying anesthetized tissue) is inflated, and the proximal cuff is subsequently deflated. The tourniquet must remain inflated for a minimum of 20 minutes to prevent rapid systemic bolus of the anesthetic upon deflation.
Systemic Opioid Administration
When systemic opioids are required, morphine remains the oldest and most thoroughly studied naturally occurring agent in this class. Adult dosing typically involves an initial intravenous loading dose of 0.05 to 0.10 mg/kg, followed by maintenance dosing of 0.8 to 10.0 mg IV titrated to clinical effect. Transition to oral equivalents (e.g., oxycodone, hydrocodone) should occur as soon as gastrointestinal function allows.
Complications and Management
The administration of potent analgesic agents is not without significant risk. Orthopaedic surgeons must be prepared to rapidly diagnose and manage systemic and localized complications arising from anesthetic and analgesic administration.

Local Anesthetic Systemic Toxicity
Local Anesthetic Systemic Toxicity (LAST) is a life-threatening complication resulting from inadvertent intravascular injection or rapid systemic absorption, leading to high plasma concentrations of the drug. The pathophysiology involves the blockade of inhibitory pathways in the central nervous system, leading to unopposed excitatory activity, followed by global CNS and cardiovascular depression.
- CNS Symptoms: Early signs include perioral tingling, tongue numbness, metallic taste, dizziness, tinnitus, and nystagmus. This can rapidly progress to muscle twitching and tonic-clonic seizures.
- Cardiovascular Symptoms: Initial hypertension and tachycardia are followed by profound myocardial depression, weaker ventricular contraction, arteriolar dilatation, and severe bradycardia. High doses, particularly of bupivacaine, can precipitate ventricular fibrillation, which is notoriously refractory to standard advanced cardiac life support (ACLS) resuscitation.
- Management: Immediate cessation of the local anesthetic. Airway management and oxygenation are paramount to prevent acidosis, which exacerbates toxicity. Seizures are managed with benzodiazepines. The definitive reversal agent is 20% Intralipid (lipid emulsion therapy), which acts as a "lipid sink" to sequester the lipophilic anesthetic molecules away from myocardial and cerebral tissue.
Opioid Related Adverse Events
Opioids exert profound systemic effects beyond analgesia, driven by peripheral and central receptor activation.
* Central Nervous System: Euphoria, sedation, respiratory depression (decreased sensitivity of the medullary respiratory center to hypercapnia), cough suppression, miosis, and nausea.
* Cardiovascular: Bradycardia and mild hypotension due to histamine release (particularly with morphine).
* Gastrointestinal: Decreased peristaltic motility leading to severe constipation, and constriction of the biliary tree (sphincter of Oddi spasm).
* Genitourinary: Decreased renal function and increased urinary sphincter tone, frequently resulting in post-operative urinary retention (POUR).
Localized Neurotoxicity
In extremely high concentrations, local anesthetics can cause direct chemical damage to peripheral nerve fibers, leading to prolonged or permanent neuropathy. This risk is minimized by strictly adhering to recommended concentration limits and avoiding intraneural injection during regional blocks.
| Complication | Incidence Rate | Clinical Presentation | Salvage Strategy and Management |
|---|---|---|---|
| Local Anesthetic Systemic Toxicity (LAST) | < 0.1% of regional blocks | Tongue numbness, tinnitus, seizures, ventricular arrhythmias. | Airway support, Benzodiazepines for seizures, 20% Intralipid emulsion bolus and infusion. |
| Opioid-Induced Respiratory Depression | 1 - 3% (dose-dependent) | Respiratory rate < 8 breaths/min, hypoxia, somnolence, pinpoint pupils. | Supplemental oxygen, stimulation, Naloxone (0.04 - 0.4 mg IV) titrated to effect. |
| Post-Operative Urinary Retention (POUR) | 10 - 30% (higher with spinal anesthesia) | Inability to void, suprapubic distension, bladder volume > 400 mL on ultrasound. | Early mobilization, warm compresses, intermittent straight catheterization. |
| Peripheral Nerve Injury (Block-related) | 0.02 - 0.04% | Persistent paresthesia, motor deficit beyond expected duration of block. | Neurologic evaluation, EMG at 3-4 weeks, Gabapentinoids for neuropathic pain. |
Post Operative Rehabilitation Protocols
Optimal orthopaedic analgesia is not merely about pain scores; it is the critical enabler of post-operative rehabilitation. Uncontrolled pain leads to muscle guarding, delayed mobilization, increased risk of deep vein thrombosis (DVT), and the development of arthrofibrosis, particularly following major joint surgery.
Integration with Physical Therapy
ERAS pathways mandate early mobilization, often on the day of surgery (Post-Operative Day 0). The analgesic protocol must therefore balance pain relief with the preservation of motor function.
* Transitioning Modalities: Intravenous opioids and continuous regional infusions should be rapidly weaned in favor of oral multimodal agents.
* Cryotherapy and Elevation: Non-pharmacologic adjuncts, including continuous cold therapy units and strict limb elevation, synergistically reduce edema and nociceptive firing, decreasing the overall reliance on chemical analgesia.
* Neuromuscular Electrical Stimulation (NMES): Can be utilized adjunctively to overcome arthrogenic muscle inhibition, particularly of the quadriceps following knee surgery, while concurrent analgesia facilitates patient tolerance of the stimulation.
Summary of Key Literature and Guidelines
The management of orthopaedic pain is heavily guided by evidence-based literature and societal consensus statements designed to optimize patient outcomes while mitigating the risks of the opioid epidemic.
- American Academy of Orthopaedic Surgeons (AAOS) Guidelines: Emphasize the routine use of multimodal analgesia, including
Clinical & Radiographic Imaging