Comprehensive Management of Amputation Complications: An Evidence-Based Surgical Guide
Key Takeaway
The management of amputation complications requires a multidisciplinary approach, focusing on meticulous surgical technique, optimized biomechanics, and rigorous postoperative care. Common complications include hematoma, deep space infection, wound necrosis, joint contractures, and residual limb pain. Successful salvage often necessitates advanced interventions such as vacuum-assisted closure, targeted wedge resections, and precise prosthetic modifications to ensure durable soft tissue coverage and functional rehabilitation.
Introduction to Amputation Complications
Amputation must be conceptualized not as a failure of limb salvage, but as the first definitive step in the reconstructive rehabilitation of the patient. The creation of a functional, durable residual limb is paramount to ensuring successful prosthetic fitting and restoring patient mobility. However, the physiological and biomechanical alterations inherent to amputations—particularly those performed for peripheral vascular disease (PVD) or diabetic neuropathy—predispose patients to a unique spectrum of postoperative complications.
This comprehensive guide delineates the pathophysiology, prevention, and evidence-based surgical management of the most frequently encountered amputation complications: hematoma, deep space infection, wound necrosis, joint contractures, complex pain syndromes, and dermatological pathologies.
Hematoma Formation
Pathophysiology and Risks
Hematoma formation within the residual limb is a critical complication that severely compromises the surgical outcome. The accumulation of blood within the dead space creates an ischemic environment that increases local tissue tension, compromises microvascular perfusion to the overlying skin flaps, and delays primary wound healing. Furthermore, the degradation of hemoglobin releases free iron, which serves as a potent culture medium for bacterial proliferation, exponentially increasing the risk of deep space infection.
Prevention Strategies
Prevention begins intraoperatively with meticulous hemostasis. Prior to closure, the pneumatic tourniquet (if utilized) should be deflated to identify and ligate all bleeding vessels.
Surgical Pearl: Meticulous hemostasis is non-negotiable. The use of closed-suction drains placed deep to the fascial layer is highly recommended to evacuate residual oozing. Furthermore, the application of a rigid dressing—such as a rigid removable dressing (RRD) or immediate postoperative prosthesis (IPOP)—provides uniform compression, minimizes dead space, and protects the limb from inadvertent trauma.
Clinical Management
If a hematoma develops, initial management depends on its size and the integrity of the overlying soft tissue envelope. Small, non-expanding hematomas may be managed conservatively with compressive dressings and close observation. However, if the hematoma is associated with delayed wound healing, impending flap necrosis, or clinical signs of infection, conservative management must be abandoned. The patient must be returned to the operating room for formal evacuation, thorough irrigation, and meticulous re-closure over a drain.
Deep Space Infection
Epidemiology and Microbiology
Infection rates are significantly higher in amputations performed for peripheral vascular disease and diabetic foot infections compared to those performed for trauma or oncologic resections. The compromised microcirculation in dysvascular patients blunts the local immune response and impairs the delivery of systemic antibiotics. Infections in this cohort are frequently polymicrobial, involving a synergistic combination of aerobic Gram-positive cocci, Gram-negative bacilli, and obligate anaerobes.
Surgical Management and Open Wound Protocols
Any deep wound infection necessitates immediate surgical intervention. Bedside interventions are inadequate. The patient must be taken to the operating room for aggressive débridement of all necrotic tissue, copious pulsatile lavage, and open wound management.
Empiric broad-spectrum intravenous antibiotics should be initiated immediately following the acquisition of deep intraoperative tissue cultures, and subsequently tailored based on definitive sensitivities.
Delayed primary closure in the setting of an infected amputation stump is notoriously difficult due to progressive tissue edema and the inevitable retraction of the myocutaneous flaps. To address this, Smith and Burgess described a highly effective partial-closure technique.
The Smith and Burgess Technique
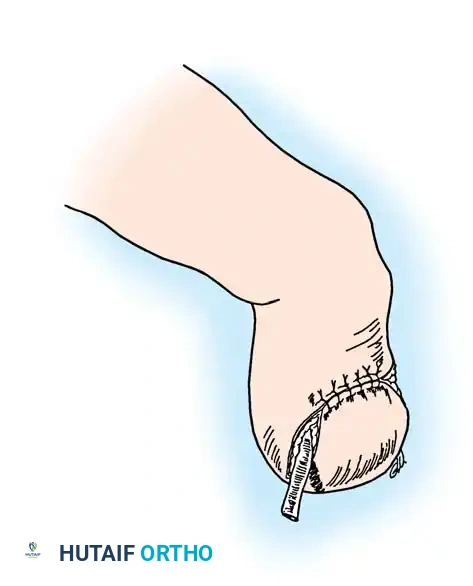
When managing an infected transtibial amputation, attempting to close the entire wound under tension will inevitably lead to marginal necrosis and recurrent infection. The Smith and Burgess method advocates for a strategic, partial closure:
1. The central one-third of the wound (directly overlying the distal tibia) is loosely approximated to protect the bone and maintain the length of the flaps.
2. The medial and lateral gutters of the wound are packed open.
3. This configuration allows for continuous open wound management, dependent drainage, and serial débridement while preserving adequate flap length for eventual definitive coverage.
Fig. 9-4 Partial closure of infected transtibial amputation. (From Smith DG, Burgess EM: Amputations. In Skinner HB, ed: Current diagnosis and treatment in orthopaedics, Norwalk, Conn, 1995, Appleton & Lange.)
Wound Necrosis and Soft Tissue Failure
Preoperative Optimization and Patient Selection
The most critical step in managing wound necrosis is preventing it through accurate preoperative selection of the amputation level. Clinical assessment of pulses is insufficient. Objective hemodynamic parameters must be evaluated:
* Transcutaneous Oxygen Tension (TcPO2): A TcPO2 > 30 mm Hg suggests adequate healing potential, whereas levels < 20 mm Hg are associated with a high rate of failure.
* Nutritional Status: Malnutrition severely impairs collagen synthesis and immune function. A serum albumin level < 3.5 g/dL or a total lymphocyte count (TLC) < 1500 cells/mL significantly increases the risk of wound failure. Aggressive nutritional supplementation is mandatory in these patients.
* Smoking Cessation: Tobacco use is an absolute contraindication to elective amputation and a major risk factor in emergent cases. Nicotine induces profound peripheral vasoconstriction, while carbon monoxide competitively binds to hemoglobin, drastically lowering tissue oxygen tension. Studies by Lind et al. demonstrated that the risk of infection and reamputation is 2.5 times higher in smokers.
Management of Marginal Necrosis
Necrosis of the skin edges measuring less than 1 cm can often be managed conservatively. The necrotic eschar can be allowed to demarcate, followed by gentle local débridement and open wound management.
Clinical Pitfall: While some authors advocate for continued weight-bearing rehabilitation using a total-contact prosthesis during the healing of minor necrosis, this risks exacerbating the tissue injury. It is highly recommended to discontinue prosthetic use until the soft tissue envelope has completely healed and matured.
Advanced Surgical Management: Wedge Resection
For more severe necrosis with poor coverage of the distal bone end, conservative measures will fail. While vacuum-assisted closure (VAC) therapy is an excellent adjunct to stimulate granulation tissue and manage exudate, definitive surgical revision is often required.
Rather than performing a formal reamputation at a higher level (which significantly increases the energy expenditure of future ambulation), a wedge resection may be indicated. As described by Hadden et al., the basic biomechanical principle of a wedge resection is to conceptualize the end of the amputation stump as a hemisphere.
Local resection of a necrotic ulcer produces uneven tension across already compromised tissues. Conversely, resecting a full-diameter wedge allows for the reformation of a smooth, hemispherical stump, thereby minimizing local peak pressures and evenly distributing tension across the closure line.
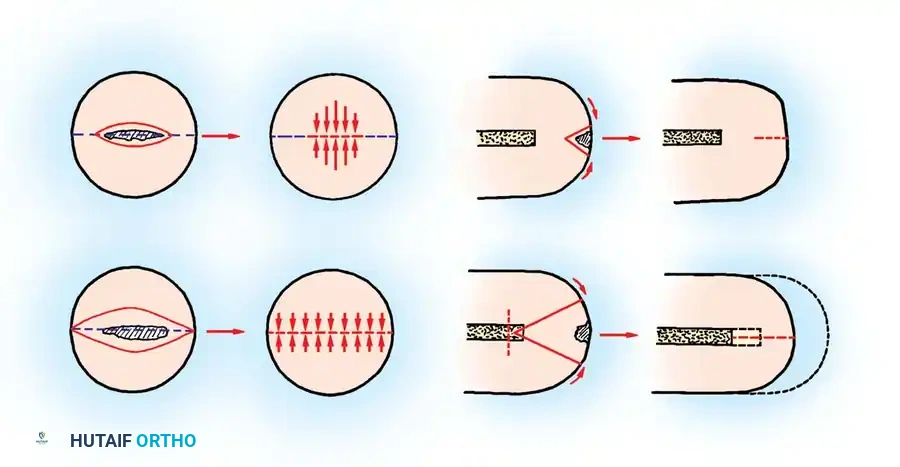
Fig. 9-5 Diagrams of end-on and side views of amputation stumps. Local resection produces uneven tension; this is reduced and evenly distributed after wedge resection. (From Hadden W, Marks R, Murdoch G, et al: Wedge resection of amputation stumps, a valuable salvage procedure, J Bone Joint Surg 69B:306, 1987.)
Adjunctive therapies, including hyperbaric oxygen therapy (HBOT) and transcutaneous electrical nerve stimulation (TENS), have demonstrated efficacy in promoting microvascular angiogenesis and accelerating wound healing in recalcitrant cases.
Joint Contractures
Biomechanics and Pathoanatomy
Joint contractures are a devastating complication that can render an otherwise perfect amputation stump un-prosthesizable. They arise from an imbalance in muscle forces following the transection of antagonist muscle groups, combined with prolonged static positioning.
* Transtibial Amputations: Prone to knee flexion contractures due to the unopposed pull of the hamstrings.
* Transfemoral Amputations: Prone to hip flexion and abduction contractures due to the unopposed pull of the iliopsoas and gluteus medius, respectively.
Prevention and Treatment Protocols
Prevention is paramount. Postoperatively, the stump must be positioned correctly. For transtibial amputees, placing a pillow under the knee is strictly forbidden. Early implementation of gentle passive stretching and active strengthening of the antagonist muscles (e.g., quadriceps in transtibial amputees) is essential.
Mild to moderate contractures can often be managed with aggressive physical therapy and prosthetic modifications (e.g., aligning the socket in initial flexion to accommodate the contracture). Severe, fixed contractures may require serial wedging casts or formal surgical release of the contracted capsuloligamentous and musculotendinous structures.
Pain Syndromes in the Amputee
Post-amputation pain is a complex, multifactorial entity. Accurate diagnosis is the cornerstone of effective management. The clinician must differentiate between residual limb pain, phantom limb pain, and referred pain from distant pathology.
Referred Pain and Spine Pathology
Mechanical low back pain is significantly more prevalent in amputees than in the general population due to altered gait biomechanics and compensatory pelvic kinematics. In a study by Smith et al., amputees frequently rated back pain as more debilitating than phantom or residual limb pain. Treatment requires optimizing prosthetic alignment to minimize abnormal stresses on the lumbar spine, core strengthening, and standard conservative spine care.
Residual Limb Pain and Neuromas
Residual limb pain is localized to the remaining physical limb. The most common cause is a poorly fitting prosthesis leading to abnormal pressure distribution over bony prominences.
The "Choking" Phenomenon: If the distal stump is not completely seated within the prosthetic socket, the proximal socket brim acts as a venous tourniquet. This leads to distal stump edema, a condition known as "choking," which can rapidly progress to ulceration, verrucous hyperplasia, or gangrene. Immediate socket modification is required.
Symptomatic Neuromas: A neuroma is an inevitable physiological consequence of nerve transection, representing frustrated axonal sprouting. However, it only becomes painful when subjected to mechanical pressure or traction.
* Prevention: Intraoperatively, nerves should be isolated, placed under gentle distal traction, sharply transected, and allowed to retract deep into healthy, well-vascularized soft tissue or bone, away from the surgical scar and future prosthetic contact areas.
* Diagnosis: A painful neuroma is typically palpable, exquisitely tender, and exhibits a strongly positive Tinel sign. High-resolution ultrasound can help differentiate a neuroma from recurrent tumor or abscess.
* Treatment: Initial management involves socket modification to relieve pressure. If conservative measures fail, surgical intervention is warranted. Options include simple excision with higher proximal retraction, centrocentral anastomosis, or modern techniques such as Targeted Muscle Reinnervation (TMR) or Regenerative Peripheral Nerve Interfaces (RPNI) to provide a physiological target for the regenerating axons.
Phantom Limb Sensations and Pain
Phantom Limb Sensation: The non-painful perception of the amputated limb is nearly universal and should be considered a normal physiological phenomenon. Patients must be educated preoperatively to prevent psychological distress. Over the first year, patients often experience "telescoping," where the perceived phantom limb gradually shortens toward the end of the residual limb.
Phantom Limb Pain (PLP): Characterized by severe, burning, or shooting pain in the absent limb. While some literature overestimates its prevalence, truly debilitating PLP affects less than 10% of amputees. It is more common in proximal amputations (e.g., forequarter or hindquarter) and in patients who experienced severe pre-amputation pain (suggesting central nervous system sensitization).
Management of PLP requires a multimodal approach. While the efficacy of preemptive epidural anesthesia remains debated, established PLP is notoriously difficult to treat. A multidisciplinary strategy utilizing gabapentinoids, tricyclic antidepressants, NMDA receptor antagonists, TENS, biofeedback, mirror therapy, and occasionally dorsal column stimulators offers the best chance for symptomatic relief.
Dermatological Pathologies
The microenvironment within a prosthetic socket—characterized by elevated temperatures, moisture, and friction—predisposes the residual limb to various dermatological issues.
Hygiene and Contact Dermatitis
Meticulous hygiene is critical. The stump and the prosthetic socket must be washed daily with mild soap and thoroughly dried before donning.
Contact dermatitis presents as intense itching, burning, and erythema, often mimicking cellulitis. Common sensitizers include residual laundry detergents in stump socks, nickel, leather chromates, rubber antioxidants, and topical creams. Management involves identifying and removing the offending irritant, applying topical corticosteroids, and utilizing compressive dressings.
Folliculitis and Epidermoid Cysts
Bacterial folliculitis frequently occurs in hairy, oily regions of the stump subjected to friction. Poor hygiene and shaving exacerbate the condition. Treatment includes improved hygiene, antibacterial washes, and socket modifications to relieve pressure. If cellulitis or an abscess develops, systemic antibiotics and surgical incision and drainage are required.
Epidermoid cysts commonly develop at the socket brim due to chronic friction and occlusion of hair follicles. These are typically late-onset complications. Initial treatment is socket modification to relieve brim pressure; recalcitrant cysts require complete surgical excision.
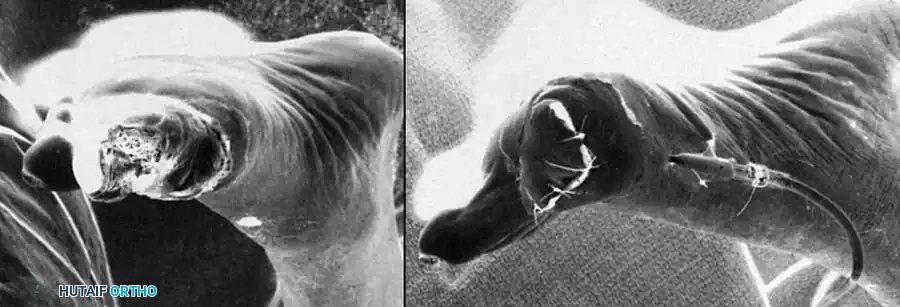
Verrucous Hyperplasia
Verrucous hyperplasia is a wart-like, hyperkeratotic overgrowth of the skin at the distal end of the stump. It is a direct biomechanical consequence of the aforementioned "choking" phenomenon. Proximal constriction prevents the stump from fully seating, leading to a lack of distal contact. The resulting dependent edema causes epidermal thickening, fissuring, and secondary bacterial infection.
> Surgical Warning: Verrucous hyperplasia cannot be cured with topical treatments alone. While secondary infections must be treated and salicylic acid used to soften the keratin, the definitive cure is mandatory socket modification. The prosthesis must be redesigned to ensure total contact, thereby restoring distal pressure, resolving the edema, and preventing recurrence.
You Might Also Like