Operative Management of Bone Sarcomas and Multiple Myeloma
Key Takeaway
Malignant fibrous histiocytoma, fibrosarcoma, and multiple myeloma represent aggressive primary bone malignancies requiring multidisciplinary intervention. This guide details the evidence-based surgical management of these lesions, emphasizing wide resection principles for sarcomas and prophylactic stabilization techniques for myeloma-induced pathological fractures. Key insights include histopathological differentiation, neoadjuvant protocols, and step-by-step operative approaches to optimize patient survival and functional outcomes.
Comprehensive Introduction and Patho-Epidemiology
The operative management of primary malignant bone sarcomas, specifically Undifferentiated Pleomorphic Sarcoma (UPS)—historically classified as Malignant Fibrous Histiocytoma (MFH)—and fibrosarcoma, alongside systemic plasma cell dyscrasias such as multiple myeloma, represents one of the most complex intersections of orthopedic oncology, biomechanics, and systemic medical management. Although these entities possess distinct cellular origins and systemic behaviors, the orthopedic surgeon is frequently tasked with managing their devastating local effects on the osseous architecture. The evolution of modern pathology has largely subsumed the traditional diagnosis of MFH of bone into the broader category of UPS, reflecting a high-grade spindle cell sarcoma devoid of a specific line of differentiation. Despite this taxonomic shift, the clinical presentation, aggressive local invasion, and propensity for early hematogenous dissemination remain identical, necessitating a unified and highly aggressive surgical and oncological approach.
These high-grade spindle cell sarcomas of bone are relatively rare, constituting approximately 3% to 5% of all primary malignant bone tumors. They exhibit a unique bimodal distribution or, more accurately, a broad age distribution that excludes the first decade of life. A critical distinguishing feature of UPS and fibrosarcoma is their significant propensity to arise as secondary malignancies. Approximately 25% of these tumors develop within a pre-existing osseous abnormality. The most frequently encountered predisposing conditions include Paget disease of bone (where sarcomatous degeneration occurs in roughly 1% of patients and portends a dismal prognosis), prior radiation osteitis (with a latency period typically spanning 5 to 15 years), and chronic medullary bone infarcts. Malignant transformation typically occurs at the periphery of an infarct, presenting a diagnostic challenge that requires a high index of suspicion when a patient with known benign osseous conditions presents with unremitting, non-mechanical pain.


Conversely, multiple myeloma is the most ubiquitous primary malignancy of bone, accounting for over 40% of all primary bone cancers. It is a systemic hematological malignancy characterized by the monoclonal proliferation of malignant plasma cells within the bone marrow space. The pathophysiology of myelomatous bone disease is driven by the uncoupling of normal bone remodeling. Malignant plasma cells secrete osteoclast-activating factors, most notably Receptor Activator of Nuclear Factor Kappa-B Ligand (RANKL), Macrophage Inflammatory Protein-1 alpha (MIP-1α), and Interleukin-6 (IL-6), while simultaneously suppressing osteoblastic activity via the secretion of Dickkopf-1 (DKK-1). This profound disruption results in purely lytic, "punched-out" lesions devoid of reactive osteosclerosis, rendering the affected bone exceptionally vulnerable to catastrophic biomechanical failure. The peak incidence occurs in the fifth to seventh decades of life, demanding that multiple myeloma and metastatic carcinoma remain the primary differential diagnoses for any patient over the age of forty presenting with a new, destructive osseous lesion.
Histopathological Characteristics and Cellular Biology
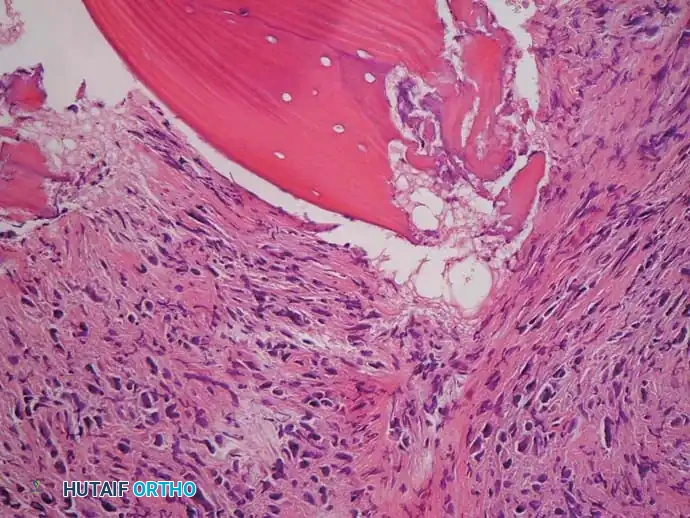
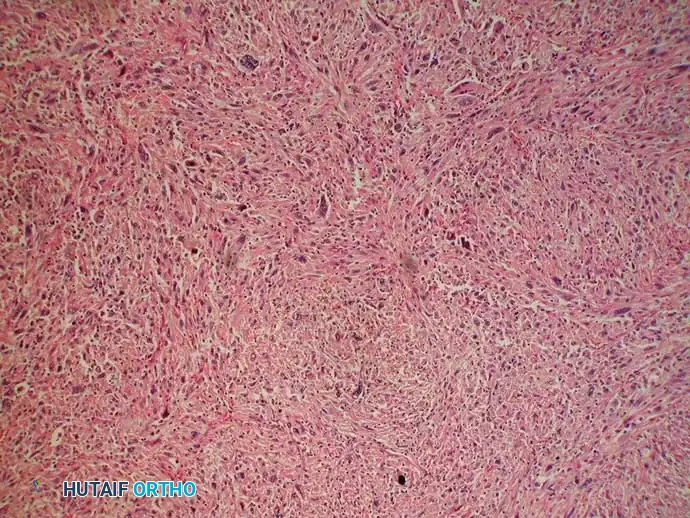
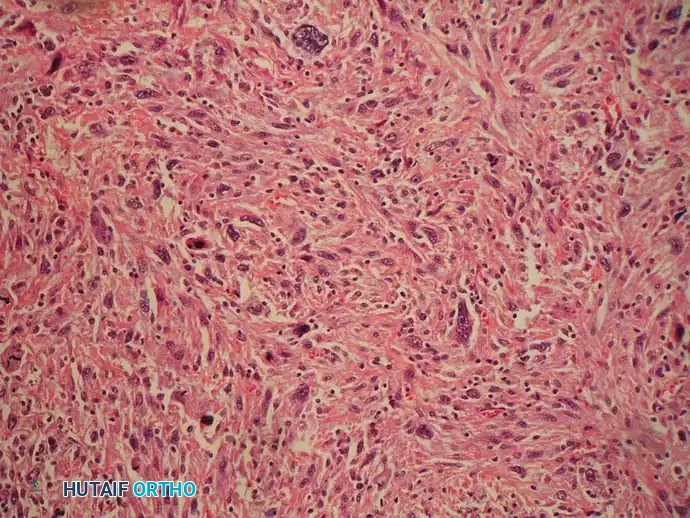
The histological diagnosis of these entities dictates the systemic chemotherapy protocols and surgical timing. UPS classically presents as a high-grade spindle cell sarcoma arranged in a storiform or cartwheel pattern, characterized by profound cellular pleomorphism. The tumor microenvironment is a chaotic admixture of benign and malignant multinucleated giant cells, histiocyte-like cells with large indented nuclei, foamy cells, and a variable inflammatory infiltrate. Fibrosarcoma, in its classic presentation, exhibits a more uniform spindle cell proliferation arranged in an intersecting fascicular or "herringbone" pattern. The absolute defining characteristic of both entities, which differentiates them from osteosarcoma, is the complete absence of malignant osteoid production. Even microscopic foci of malignant osteoid mandate a diagnosis of osteosarcoma.
Multiple myeloma, in stark contrast, is diagnosed via the identification of dense sheets of malignant, monoclonal plasma cells within the marrow space. These cells are classically described as small, round blue cells with eccentric "clock-face" nuclei and abundant basophilic cytoplasm containing a prominent perinuclear halo representing the Golgi apparatus. Immunohistochemical staining is paramount for definitive diagnosis; myelomatous cells typically exhibit strong positivity for CD138 (syndecan-1) and CD56, while demonstrating light chain restriction (either kappa or lambda) indicative of monoclonality. The presence of amyloid deposition within the bone tissue, barring patients on long-term hemodialysis, is virtually pathognomonic for multiple myeloma and further complicates the local tissue biomechanics.
Detailed Surgical Anatomy and Biomechanics
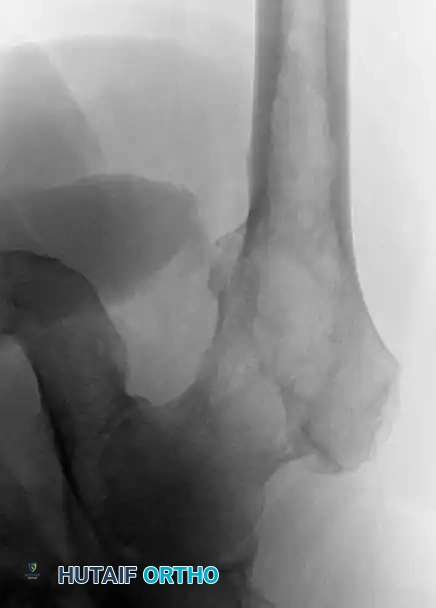
A profound understanding of compartmental anatomy and local biomechanics is non-negotiable when planning the operative management of bone sarcomas and myelomatous lesions. Bone sarcomas such as UPS and fibrosarcoma most frequently arise in the appendicular skeleton, with a strong predilection for the distal metaphysis of the femur and the proximal metaphysis of the tibia. The anatomical constraints of these regions dictate the feasibility of limb-salvage surgery. In the distal femur, the tumor frequently breaches the posterior cortex, entering the popliteal fossa. The critical anatomical relationship is the proximity of the tumor pseudocapsule and its surrounding reactive zone to the superficial femoral artery and vein as they transition through the adductor hiatus to become the popliteal vessels. Achieving a wide oncological margin requires dissecting outside this reactive zone, often necessitating the sacrifice of adjacent musculature (e.g., vastus intermedius, portions of the adductor magnus) while meticulously skeletonizing and preserving the neurovascular bundle.

The biomechanical consequences of these malignancies are profound and dictate the urgency of surgical intervention. Bone sarcomas produce aggressive, permeative osteolysis with a wide zone of transition. The destruction of cortical bone significantly reduces the bone's load-bearing capacity. According to the principles of solid mechanics, the torsional strength of a tubular bone is proportional to the fourth power of its radius. Therefore, even a seemingly small cortical defect acts as a massive stress riser, drastically reducing the torque required to induce a spiral fracture. In the setting of UPS or fibrosarcoma, a pathological fracture is a disastrous event; it contaminates the surrounding soft tissue compartments with microscopic disease, potentially converting a limb-salvage candidate into an obligate amputee.
Biomechanics of Myelomatous Osteolysis
In multiple myeloma, the biomechanical failure is systemic and multifocal. The purely lytic nature of myeloma lesions, combined with the complete absence of reactive bone formation (sclerosis), renders the bone mechanically incompetent. The proximal femur is particularly vulnerable due to the complex interplay of compressive forces on the medial calcar and immense tensile forces on the lateral cortex during normal gait. When a myelomatous lesion involves the lateral cortex of the subtrochanteric region, the risk of a transverse or short oblique fracture under tensile loading is extraordinarily high.
The evaluation of impending pathological fractures in these patients relies heavily on Mirels' criteria, a scoring system that evaluates the site of the lesion (upper extremity, lower extremity, peritrochanteric), the nature of the lesion (blastic, mixed, lytic), the size of the lesion (<1/3, 1/3-2/3, >2/3 of the cortical diameter), and the presence of mechanical pain. A Mirels' score of 9 or greater is a strong indication for prophylactic stabilization. Because myeloma patients often suffer from profound systemic debilitation, the chosen orthopedic construct must bypass the areas of structural deficit entirely, providing immediate, load-sharing stability that permits unrestricted weight-bearing without relying on the host bone for primary mechanical support or healing.
Exhaustive Indications and Contraindications
The decision-making algorithm for operative intervention in bone sarcomas and multiple myeloma requires a multidisciplinary consensus involving orthopedic oncology, medical oncology, radiation oncology, and musculoskeletal pathology. The overarching goal in sarcoma surgery is overall survival via the achievement of wide, negative oncological margins, with limb salvage being a secondary, albeit highly desirable, objective. Conversely, in multiple myeloma, the primary goal is the immediate restoration of mechanical stability and the palliation of pain to maximize the patient's quality of life during systemic therapy.
For primary bone sarcomas (UPS and fibrosarcoma), the absolute indication for surgery is the presence of a localized, resectable tumor. Neoadjuvant chemotherapy is the standard of care to eradicate micrometastatic disease and induce tumor necrosis, which facilitates subsequent surgical resection. Limb-salvage surgery with endoprosthetic reconstruction is indicated when a wide margin can be achieved while preserving a functional neurovascular bundle and adequate soft tissue coverage. Amputation remains a critical, life-saving procedure and is strictly indicated when these criteria cannot be met.
Summary of Operative Parameters
| Clinical Scenario | Primary Indications for Surgical Intervention | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| UPS / Fibrosarcoma (Limb Salvage) | Localized disease; Intact major neurovascular bundle; Ability to achieve wide margins; Adequate soft tissue for coverage. | Major neurovascular bundle encasement precluding wide resection; Inability to achieve negative margins; Severe systemic sepsis. | Pathological fracture with massive soft tissue contamination; Poor response to neoadjuvant chemotherapy; Extensive skin involvement. |
| UPS / Fibrosarcoma (Amputation) | Inability to achieve wide margins with limb salvage; Neurovascular encasement; Massive recurrence post-limb salvage; Palliation of fungating, painful mass. | Refusal of consent by a competent patient. | Severe cardiopulmonary instability precluding major anesthesia (requires optimization). |
| Multiple Myeloma (Prophylactic Fixation) | Mirels' score $/ge$ 9; Lesion >2.5 cm or >50% cortical destruction in weight-bearing bone; Unremitting mechanical pain post-radiation. | Active, uncontrolled local infection; Patient is actively dying (life expectancy < 4 weeks) where surgery offers no palliative benefit. | Severe, uncorrectable coagulopathy (thrombocytopenia common in myeloma); Extreme hypercalcemia requiring prior medical management. |
| Multiple Myeloma (Fracture Fixation) | Completed pathological fracture in an appendicular long bone or acetabulum; Spinal instability with progressive neurological deficit. | Medical instability precluding anesthesia; Active local infection. | Life expectancy < 6 weeks; Inability to tolerate rehabilitation. |
The contraindications for surgical intervention must be carefully weighed against the morbidity of non-operative management. In a patient with a completed pathological fracture due to myeloma, non-operative management often condemns the patient to bed rest, rapid deconditioning, pneumonia, deep vein thrombosis, and an accelerated demise. Therefore, unless the patient is actively transitioning to hospice care with a life expectancy measured in days, surgical stabilization is almost universally indicated to facilitate nursing care and pain control.
Pre-Operative Planning, Templating, and Patient Positioning
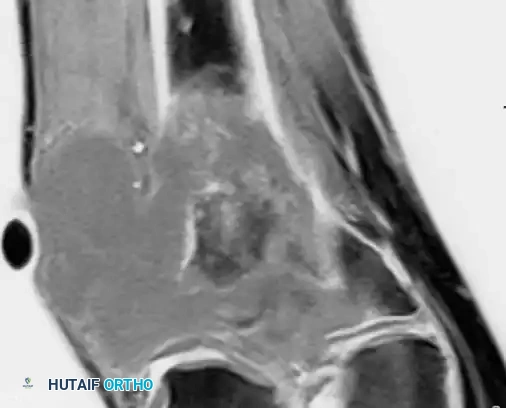
Meticulous preoperative planning is the cornerstone of successful orthopedic oncology surgery. The margin of error is virtually nonexistent; an unplanned positive margin in sarcoma surgery drastically increases the rate of local recurrence and negatively impacts overall survival. Advanced imaging is mandatory. Magnetic Resonance Imaging (MRI) of the entire involved bone is the gold standard for local staging. It precisely delineates the intraosseous extent of the tumor, identifies "skip" metastases within the same medullary canal, and maps the extraosseous soft-tissue extension relative to critical neurovascular structures. T1-weighted longitudinal images are critical for determining the level of the osteotomy, which is typically planned 3 to 5 centimeters beyond the proximal-most extent of the marrow signal abnormality.
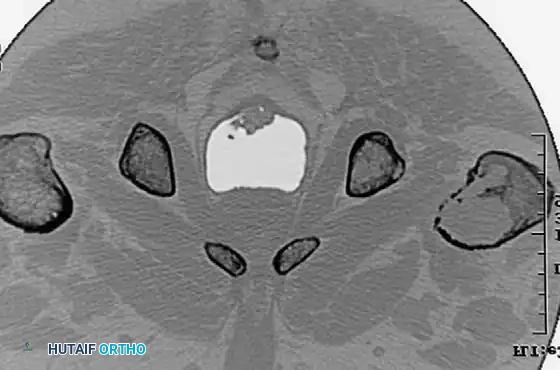

For multiple myeloma, while MRI is useful for evaluating spinal cord compression, whole-body low-dose Computed Tomography (CT) or a complete skeletal survey is the preferred modality for identifying impending pathological fractures. CT scans provide unparalleled detail regarding the exact degree of cortical osteolysis, allowing the surgeon to template the size and length of the required intramedullary device. Because myeloma lesions do not provoke a blastic response, technetium-99m bone scans are notoriously unreliable and frequently yield false-negative results.
Biopsy Principles and Digital Templating
The biopsy is the final, critical step in preoperative planning and must be performed by the surgeon who will execute the definitive resection. The biopsy tract is considered contaminated with tumor cells and must be excised en bloc with the primary specimen. Therefore, the incision must be strictly longitudinal, meticulously hemostatic, and placed directly in line with the planned standard surgical approach. Transverse incisions or multi-compartmental contamination during biopsy are catastrophic errors that may necessitate amputation.
Digital templating is performed using calibrated orthogonal radiographs and CT/MRI data. For limb-salvage megaprostheses, the surgeon must calculate the exact resection length to order the appropriate modular components (stems, intercalary segments, articular surfaces). For prophylactic stabilization of myeloma lesions, templating ensures the selected cephalomedullary nail spans the entire bone, bypassing all lytic defects. The diameter of the nail must be carefully selected; the profound cortical thinning in myeloma bone makes iatrogenic fracture during reaming a significant risk, often necessitating the use of slightly undersized nails augmented with polymethylmethacrylate (PMMA) bone cement.
Patient positioning is dictated by the planned approach. For distal femoral resections and proximal femoral nailing, the patient is typically positioned supine. A radiolucent table or a fracture table is utilized to allow unobstructed fluoroscopic access. In sarcoma surgery, a sterile tourniquet is applied to the proximal limb but is strictly left uninflated. Tourniquet ischemia alters the visual characteristics of the tissues, making it exceedingly difficult to differentiate the tumor pseudocapsule and reactive zone from normal, viable muscle. The tourniquet is reserved solely for catastrophic, life-threatening hemorrhage.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution requires a dual proficiency in aggressive oncological resection and complex biomechanical reconstruction. The techniques diverge significantly based on whether the pathology is a primary sarcoma requiring wide margins or a systemic myelomatous lesion requiring palliative stabilization.
Wide Resection of the Distal Femur for UPS/Fibrosarcoma
When limb-salvage is feasible for a distal femoral UPS or fibrosarcoma, an en bloc resection with modular endoprosthetic reconstruction is the standard of care.
- Incision and Exposure: A standard anterior or anteromedial utility incision is utilized. The incision must incorporate the previous biopsy tract in an elliptical fashion, ensuring the tract remains in continuity with the underlying tumor mass. Skin flaps are raised, maintaining a thick layer of subcutaneous tissue to preserve vascularity.
- Vascular Dissection: The vastus medialis is elevated off the adductor intermuscular septum. The superficial femoral artery and vein are identified at the apex of the femoral triangle and traced distally to the adductor hiatus. The vessels are meticulously dissected free from the tumor pseudocapsule. If the tumor abuts the vessels, the adventitia may need to be carefully peeled away, or a vascular bypass may be required if encasement is present.
- Muscular Resection: The quadriceps mechanism is evaluated. The vastus intermedius is almost universally sacrificed en bloc with the distal femur. The rectus femoris is preserved if uninvolved. The medial and lateral hamstrings are retracted or transected depending on posterior tumor extension.
- Osteotomy and Margin Assessment: Based on preoperative MRI measurements, the femoral osteotomy site is marked. Retractors are placed to protect the surrounding soft tissues, and the osteotomy is performed using a heavy-duty oscillating saw. Immediately, a marrow sample from the remaining proximal femur is extracted and sent to pathology for frozen section analysis to unequivocally confirm a negative intramedullary margin.
- Joint Resection: The knee joint is entered via a medial parapatellar arthrotomy. If the tumor is strictly extra-articular, the cruciate and collateral ligaments are transected, and the distal femur is delivered from the field. If intra-articular contamination is suspected, an extra-articular resection is performed, removing the entire knee joint (distal femur, patella, and proximal tibia) en bloc without breaching the capsule.
- Megaprosthetic Reconstruction: A modular distal femoral replacement is assembled on the back table to match the exact resection length. The femoral canal is prepared, and the stem is typically cemented using antibiotic-impregnated PMMA to provide immediate fixation and allow early weight-bearing. The tibial baseplate is similarly cemented. The modular hinge mechanism is engaged.
- Soft Tissue Coverage and Closure: The extensor mechanism is reconstructed. If a significant portion of the quadriceps was resected, the remaining tendon is advanced and sutured to the megaprosthesis using heavy non-absorbable tape. A medial gastrocnemius rotational flap is frequently utilized to provide robust, vascularized soft-tissue coverage over the metallic prosthesis, mitigating the risk of infection and wound breakdown.
Prophylactic Cephalomedullary Nailing for Multiple Myeloma
For extensive lytic lesions of the proximal femur secondary to multiple myeloma, the goal is immediate, durable stabilization. The procedure seamlessly continues from the initial prompt's description.
- Positioning and Reduction: The patient is placed supine on a fracture table. Gentle traction is applied to align the mechanical axis, even if a fracture has not yet completed, to ensure proper nail trajectory.
- Approach and Debulking: A minimally invasive lateral approach proximal to the greater trochanter is utilized. If the subtrochanteric lesion is massive, a small lateral cortical window is created. The gross tumor volume is aggressively curetted. This achieves two goals: it reduces the local tumor burden and creates a massive void for cement augmentation.
- Canal Preparation: A ball-tipped guide wire is passed down the femoral canal, ensuring it remains centrally located within the thinned cortices. Sequential reaming is performed with extreme caution. The osteoporotic and infiltrated nature of myeloma bone makes it highly susceptible to iatrogenic blowout.
- Cement Augmentation (The Composite Construct): Antibiotic-loaded PMMA bone cement is mixed. Once it reaches a doughy, viscous state, it is injected directly into the curetted lytic defect via the lateral window or down the intramedullary canal using a chest tube or specialized cement delivery system.
- Nail Insertion: Before the cement polymerizes, a long cephalomedullary nail is immediately passed over the guide wire, through the curing cement, spanning the entire femur to the intercondylar notch. The nail acts as internal rebar within the PMMA mantle.
- Locking: Proximal reconstruction screws are placed into the femoral head, and distal interlocking screws are placed to control rotation. The curing cement provides massive surface area interlock, creating a composite construct that is biomechanically vastly superior to the nail alone in osteoporotic bone.
- Arthroplasty Considerations: If the articular surface or femoral neck is completely destroyed by myelomatous infiltration, internal fixation is doomed to failure. In these instances, a cemented bipolar hemiarthroplasty or total hip arthroplasty using a long-stem revision component is mandatory. The long stem must bypass the most distal lytic lesion by a minimum of two cortical diameters to prevent periprosthetic stress fractures.

Complications, Incidence Rates, and Salvage Management
The operative management of these pathologies carries a formidable complication profile. The combination of massive surgical dissection, implantation of large volumes of foreign material (megaprostheses, PMMA), and the immunosuppressive effects of systemic chemotherapy and radiation creates a perfect storm for adverse events. The orthopedic oncologist must be hyper-vigilant and prepared to execute complex salvage procedures.
Infection is the most dreaded complication following limb-salvage surgery. Deep periprosthetic joint infection (PJI) occurs in approximately 10% to 15% of megaprosthesis reconstructions. The risk is significantly elevated in patients receiving neoadjuvant chemotherapy, which induces profound neutropenia and impairs wound healing. Aseptic loosening and structural failure of the implant are also common, particularly in younger, more active sarcoma survivors. The 10-year survival rate of a distal femoral megaprosthesis is roughly 70%, with failure modes including bushing wear, stem fracture, and periprosthetic fracture.
Local recurrence of the sarcoma is a catastrophic event, occurring in 5% to 10% of patients despite negative margins. It is often an indicator of aggressive tumor biology and systemic micrometastatic escape. In the setting of multiple myeloma, systemic complications such as deep vein thrombosis (DVT), pulmonary embolism (PE), and acute renal failure (exacerbated by surgical stress and cement monomer release) are the primary causes of perioperative morbidity and mortality.
Complication Profile and Salvage Strategies
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management Strategy |
|---|---|---|---|
| Deep Periprosthetic Infection | 10% - 15% (Sarcoma) | Immunosuppression, large dead space, prolonged operative time, radiation. | Two-stage revision with antibiotic spacer; Suppressive antibiotics; Amputation if eradication fails or soft tissue envelope is destroyed. |
| Aseptic Loosening | 15% - 20% at 10 years | Stress shielding, osteolysis, high mechanical demand, poor initial fixation. | Revision arthroplasty with longer stems, structural allograft, or custom 3D-printed metaphyseal cones. |
| Local Tumor Recurrence | 5% - 10% | Positive surgical margins, poor histologic response to chemotherapy, aggressive biology. | Restaging; Radical re-resection if feasible; Often necessitates amputation to achieve local control. |
| Structural Implant Failure | 5% - 10% at 10 years | Fatigue failure of modular junctions, stem fracture, bushing wear. | Component exchange; Revision of broken stems using trephines and extended trochanteric/femoral osteotomies. |
| VTE (DVT / PE) | 10% - 20% (Myeloma) | Hypercoagulable state of malignancy, immunomodulatory drugs (Thalidomide/Lenalidomide), immobility. | Aggressive chemical prophylaxis (LMWH or DOACs); IVC filter if anticoagulation is strictly contraindicated. |
Salvage management requires a highly individualized approach. For an infected megaprosthesis, a two-stage revision utilizing a custom-molded, articulating antibiotic cement spacer is the standard of care. This maintains soft tissue tension and joint space while delivering high local concentrations of antibiotics (typically Tobramycin and Vancomycin). If the infection is recalcitrant, or if the soft tissue envelope is irreparably compromised, an above-knee amputation or hip disarticulation becomes necessary to save the patient's life from overwhelming sepsis.
Phased Post-Operative Rehabilitation Protocols
Rehabilitation following orthopedic oncology surgery is an arduous process that must be carefully tailored to the specific surgical construct and the patient's systemic oncological treatment plan. The protocols differ drastically between a patient who has undergone a distal femoral replacement for a sarcoma and a patient who has received a prophylactic cephalomedullary nail for multiple myeloma.
Phase I: Immediate Post-Operative Period (Weeks 0-2)
For patients with a distal femoral megaprosthesis, the primary goal in Phase I is wound healing and the prevention of contractures. Weight-bearing is typically allowed as tolerated immediately, as the cemented stem provides rigid fixation. However, range of motion (ROM) is strictly protected. Because the extensor mechanism has been detached and reconstructed, active knee extension is strictly prohibited for 4 to 6 weeks to prevent extensor lag or catastrophic rupture of the repair. Patients are placed in a hinged knee brace locked in extension for ambulation.
For the multiple myeloma patient post-prophylactic nailing, the goal is immediate, unrestricted mobilization. Because the construct relies on the intramedullary nail and PMMA cement rather than biological bone healing, patients are encouraged to bear full weight immediately. This rapid mobilization is critical for preventing pulmonary complications and minimizing the deconditioning associated with prolonged bed rest in this fragile population.
Phase II: Intermediate Rehabilitation (Weeks 2-6)
In the sarcoma cohort, once the surgical incision has healed and the sutures/staples are removed, gentle passive and active-assisted ROM of the knee is initiated. The brace is unlocked gradually, typically allowing 0 to 30 degrees of flexion initially, progressing to 90 degrees by week 6. Chemotherapy is usually resumed during this phase (typically 2 to 3 weeks post-operatively), which can cause profound fatigue, nausea, and neutropenia, significantly hindering physical therapy efforts. The therapist must monitor blood counts and adjust the intensity of the sessions accordingly.
For the myeloma patient, Phase II focuses on gait training, core strengthening, and restoring independence in activities of daily living (ADLs). Pain management is paramount, as these patients often have multiple other painful lytic lesions throughout their axial and appendicular skeleton. Radiation therapy to the operative site may commence during this phase to eradicate residual local microscopic disease, which can cause localized erythema and fatigue but generally does not alter the structural integrity of the cemented construct.
Phase III: Advanced Rehabilitation and Maintenance (Weeks 6+)
For megaprosthesis patients, active knee extension is cautiously introduced after 6 weeks, focusing on closed-chain kinetic exercises to protect the patellofemoral articulation. The ultimate goal is independent ambulation without assistive devices, though many patients will permanently require a cane for long distances due to altered joint kinematics and loss of proprioception. High-impact activities (running, jumping) are permanently restricted to prevent premature aseptic loosening and catastrophic failure of the modular hinge mechanism.
For the myeloma patient, rehabilitation transitions into a maintenance phase. The focus shifts to energy conservation, fall prevention, and accommodating the systemic progression of the disease. The orthopedic surgeon continues to monitor the patient radiographically at regular intervals to ensure the integrity of the fixation and to screen for new
