Mastering Musculoskeletal Tumor Biopsy: A Comprehensive Intraoperative Guide

Key Takeaway
This masterclass provides a detailed intraoperative guide to musculoskeletal tumor biopsy. We cover meticulous preoperative planning, essential anatomical considerations, precise step-by-step execution for both needle and open techniques, and strategies for avoiding common pitfalls. Emphasis is placed on preserving future definitive resection options and ensuring accurate histological diagnosis, crucial for optimal oncologic patient care.
Comprehensive Introduction and Patho-Epidemiology
Welcome, fellows, to the operating theater and the foundational stage of orthopedic oncology. Today, we are deeply analyzing a procedure that, while seemingly straightforward to the untrained eye, is arguably the most critical and unforgiving step in the comprehensive management of musculoskeletal tumors: the biopsy. You must regard this intervention not as a mere shortcut to a histological diagnosis, but as the final, definitive diagnostic procedure that dictates all subsequent surgical and oncological planning. A poorly conceived or improperly executed biopsy is not just a minor technical misstep; it is a profound clinical catastrophe. An errant incision or a massive post-operative hematoma can irreparably jeopardize limb salvage, exponentially increase the risk of local recurrence, and severely negatively impact overall patient survival. Our objective in this chapter is to equip you with the advanced oncologic principles, anatomical mastery, and surgical precision required to execute a flawless, oncologically sound biopsy, every single time.
Before we even consider touching the patient or marking an incision, a profound, molecular-level understanding of tumor biology and local anatomy is absolutely paramount. Sarcomas, which form our primary focus in orthopaedic oncology, exhibit distinct, highly predictable growth patterns that differ fundamentally from other malignancies. Unlike carcinomas, which tend to invade surrounding tissues indiscriminately through lymphatic channels, sarcomas generally respect established anatomic borders. They initially proliferate within their specific compartment of origin, taking the path of least resistance through soft tissues or bone marrow spaces, constrained temporarily by fascial septa, periosteum, or articular cartilage.
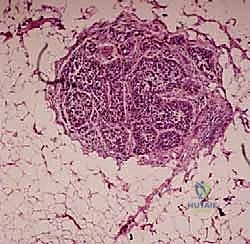
Most sarcomas form a solid, expansile mass that grows centrifugally. As the tumor expands, the periphery of the lesion is typically the most immature, rapidly dividing, and metabolically active portion of the mass. Consequently, this peripheral zone is the ideal and mandatory target for biopsy. This is a critical distinction that many novice surgeons fail to grasp: sampling the deep center of a large, high-grade sarcoma often yields only necrotic tissue, liquefied debris, or old blood, leading to an inconclusive diagnosis—a classic "sampling error." The tumor outgrows its blood supply centrally, leading to necrosis; therefore, the viable, diagnostic cells reside at the advancing edge.
Sarcomas are characteristically enclosed by a reactive zone, often termed a pseudocapsule, rather than a true histologic capsule. This pseudocapsule is not a barrier formed by the tumor itself, but rather a complex layer consisting of compressed normal host tissues, reactive fibrovascular tissue, and dense inflammatory components responding to the advancing malignancy.
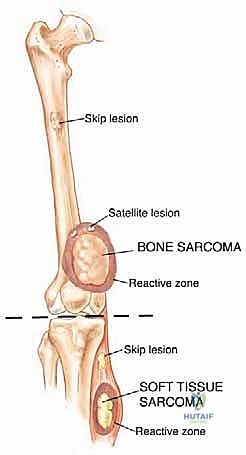
Crucially, aggressive tumor cells can and frequently do break through this pseudocapsule, forming satellite nodules or "skip metastases" within the same anatomic compartment. These are locoregional micrometastases that have not yet entered the systemic venous circulation, but they are highly viable, aggressive tumor cells.

This biological phenomenon is a primary reason why marginal excisions (shelling out the tumor) universally fail in sarcoma management, leading to local recurrence despite apparently negative macroscopic margins after resection. The presence of these skip lesions mandates wide en bloc resection, taking a cuff of normal tissue to ensure all microscopic satellites are eradicated.

The Biological Imperative of the Advancing Edge
The advancing edge of a musculoskeletal tumor represents the interface between host immune response and malignant proliferation. When performing a biopsy, the surgeon must navigate this interface with extreme care. Breaching the pseudocapsule releases tumor cells, which can immediately seed the surrounding virgin tissue planes. This iatrogenic seeding transforms a contained, intracompartmental lesion into an extracompartmental disaster. Therefore, the biopsy tract itself becomes an extension of the tumor.
The biological behavior of these tumors dictates that any tissue exposed to the biopsy instrument, any hematoma that forms post-operatively, and the entire skin tract must be considered grossly contaminated. If the biopsy is performed through an anatomical plane that cannot be safely resected during the definitive limb-salvage procedure (for example, traversing a major neurovascular bundle or contaminating an adjacent, uninvolved muscle compartment), the surgeon has effectively sentenced the patient to an amputation.
Understanding the microscopic composition of the reactive zone is essential for interpreting frozen sections intraoperatively. The pathologist will often see reactive woven bone, dense fibrosis, and chronic inflammation before reaching the actual tumor cells. The surgeon must be persistent, ensuring that the biopsy instrument passes through this reactive zone and into the viable tumor periphery to secure diagnostic tissue, without plunging so deep as to retrieve only central necrosis.
Detailed Surgical Anatomy and Biomechanics
Understanding how tumors interact with anatomical barriers is the cornerstone of orthopedic oncology. Initially, sarcomas are strictly contained within their compartment of origin. A compartment is defined as an anatomic space bounded by natural barriers to tumor extension. These barriers include major fascial septa, the periosteum of bone, articular cartilage, and dense tendinous insertions. However, at a later stage of disease progression, the walls of that compartment are invariably violated by enzymatic degradation and mechanical pressure, and the tumor breaks into a surrounding, previously uninvolved compartment.

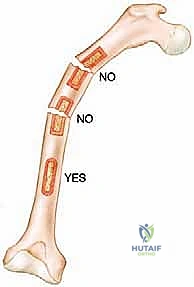
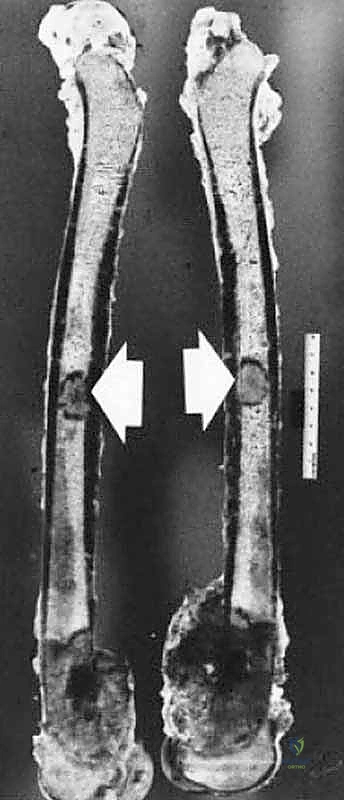
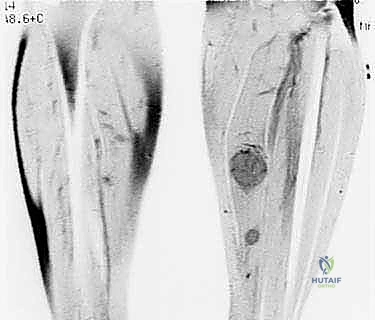
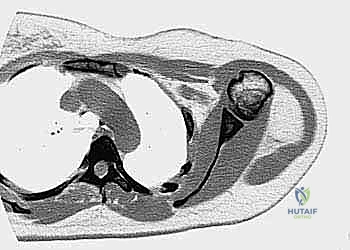
Most primary high-grade bone sarcomas (such as osteosarcoma or Ewing sarcoma) are bicompartmental at the time of clinical presentation. They originate in the medullary canal (the first compartment), aggressively destroy the overlying cortical bone, breach the periosteum, and extend into the adjacent soft tissues (the second compartment). This extraosseous soft tissue mass is critical for the biopsy surgeon; it provides a highly accessible, diagnostic target that precludes the need to create a cortical window in the bone.


Soft tissue sarcomas may arise entirely within a single muscle belly (intracompartmental) or between compartments in areas lacking clear, robust fascial barriers, such as the intermuscular fascial planes, the popliteal fossa, the femoral triangle, or the subcutaneous fat. These are classified as extracompartmental from their inception. They remain within these loose connective tissue planes until they grow large enough to compress and eventually violate adjacent muscular compartments or encase neurovascular structures.



The Biomechanics of Cortical Windows
When an extraosseous mass is absent, and the tumor is confined entirely within the medullary canal, the surgeon must breach the cortical bone to obtain a sample. This introduces a profound biomechanical complication: the creation of a stress riser. The diaphyseal and metaphyseal regions of long bones are subjected to massive torsional and bending forces during normal physiological loading. Creating a cortical window significantly reduces the polar moment of inertia of the bone, drastically increasing the risk of a pathological fracture.
A pathological fracture through a tumor-laden bone is an oncologic emergency and a catastrophic event. The fracture hematoma, heavily seeded with malignant cells, dissects wildly through surrounding tissue planes, contaminating massive areas of the limb that were previously pristine. This often converts a straightforward limb-salvage candidate into an amputation requirement. Therefore, if a cortical window must be made, it should be small, strictly circular or oval (to avoid sharp corners that concentrate stress), and ideally plugged with polymethylmethacrylate (PMMA) bone cement to restore some compressive strength and seal the defect against tumor cell extrusion.


Furthermore, the anatomical approach must meticulously avoid contaminating joint spaces. Intra-articular biopsy of a peri-articular tumor is strictly forbidden unless the joint is already grossly involved by the tumor. The synovial fluid acts as a rapid transport medium, and contaminating a joint means the entire joint capsule, synovium, and articular surfaces must be resected en bloc during the definitive procedure, severely complicating reconstruction and functional outcomes.
Exhaustive Indications and Contraindications
The decision to perform a biopsy must be made systematically, following a strict algorithmic approach. A biopsy is never an emergency procedure. It is the final step in the diagnostic workup, performed only when all non-invasive diagnostic modalities have been exhausted, and a definitive histological diagnosis is required to initiate neoadjuvant chemotherapy, radiation, or plan the definitive surgical resection.
The primary indication for a biopsy is the presence of an indeterminate or suspicious bone or soft tissue lesion identified on advanced imaging, where the diagnosis cannot be confidently established as a benign "leave-alone" lesion (e.g., non-ossifying fibroma, simple bone cyst, classic osteochondroma) based on radiographic criteria alone. In modern practice, image-guided core needle biopsy (CNB) is the gold standard and first-line approach due to its high diagnostic accuracy (exceeding 90% in experienced centers), minimal tissue contamination, and low complication rate. Open incisional biopsy is reserved for cases where CNB is non-diagnostic, or when sufficient tissue architecture is required for complex molecular and cytogenetic profiling that cannot be obtained via needle.
Absolute and Relative Contraindications
The absolute contraindications to biopsy are as critical as the indications. The most paramount contraindication is performing a biopsy prior to completing the full local and systemic staging workup. Biopsy superimposes real and artificial radiologic changes—such as hemorrhage, edema, and inflammation—that completely obscure the true anatomical margins of the tumor on subsequent MRI, rendering accurate surgical planning impossible.
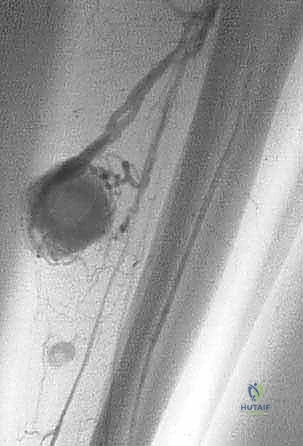
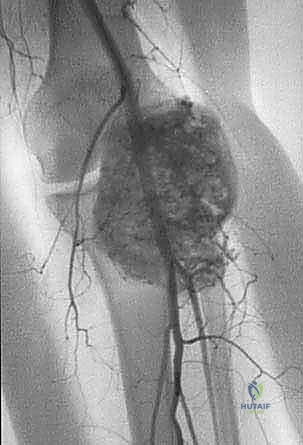
Another absolute contraindication is the suspicion of a purely fluid-filled, highly vascular lesion, such as an aneurysmal bone cyst (ABC) or a massive hemangioma, without proper precautions. Plunging a biopsy needle into an un-embolized, highly active ABC can lead to uncontrollable, life-threatening hemorrhage. Similarly, a biopsy should never be performed by a surgeon or at an institution that is not fully equipped to perform the definitive oncologic resection. The surgeon who performs the biopsy should ideally be the one performing the definitive surgery, as they must take ownership of the biopsy tract.
| Category | Specific Indications | Specific Contraindications |
|---|---|---|
| Clinical Status | Suspicious, growing, or painful mass lacking benign radiographic features. | Patient medically unstable for anesthesia (if open biopsy required). |
| Imaging Status | Complete local (MRI) and systemic (CT, PET) staging finished. | ABSOLUTE: Incomplete imaging/staging. MRI not yet performed. |
| Lesion Type | Solid mass, aggressive periosteal reaction, cortical destruction. | Suspected active infection (requires culture protocols, not just oncologic biopsy). Suspected severe vascular malformation (without angio backup). |
| Logistics | Performed at a tertiary sarcoma referral center by the treating oncologic surgeon. | ABSOLUTE: Performed by an inexperienced surgeon in a non-specialized center. |
Pre-Operative Planning, Templating, and Patient Positioning
The biopsy is the culmination of a rigorous, multidisciplinary diagnostic process. It must always be preceded by a thorough clinical evaluation and comprehensive imaging studies. Remember the diagnostic triad: clinical findings, pathological findings, and imaging findings. All three must perfectly coincide. If the pathologist reports a low-grade benign lesion, but the MRI shows massive cortical destruction and a huge soft tissue mass, you must question the diagnosis and consider a repeat biopsy. The surgeon is the ultimate arbiter of the clinical picture.
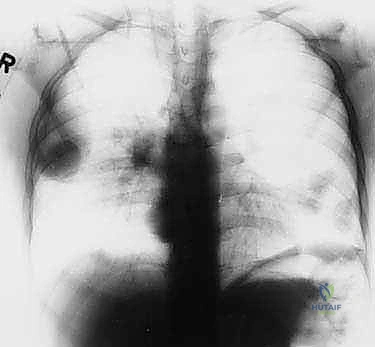
Biopsy should only be performed after complete staging. This means obtaining all necessary imaging—specifically, a contrast-enhanced MRI of the entire involved bone or compartment, high-resolution CT of the chest to rule out pulmonary metastases, and potentially a bone scan or PET-CT to identify skeletal metastases. This exhaustive dataset informs the critical questions we must answer before making an incision: What specific part of the lesion needs to be biopsied? What is the safest, most direct anatomic route to that location that avoids major neurovascular structures?



Biopsy Site Selection and Tract Planning
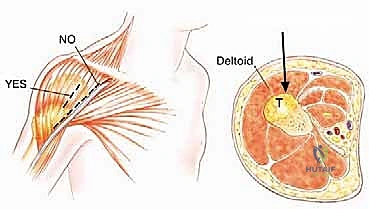
This is where true oncologic surgical planning shines. The biopsy incision, the needle puncture site, and the entire three-dimensional tract leading to the tumor must be meticulously planned so they can be completely excised en bloc with the tumor during the definitive resection. This means the biopsy tract must lie perfectly within the planned surgical incision site for the future limb-sparing surgery.

If you place the biopsy tract transversely, or far away from the standard extensile surgical approaches, you force a wider, vastly more morbid resection. You may be forced to resect an excessive amount of skin, preventing primary closure, or you may contaminate a critical muscle group required for flap reconstruction.
For soft tissue sarcomas, the periphery of the lesion is the target. For bone sarcomas, if there is an extraosseous component, biopsy that component exclusively. It is equally representative of the tumor's highest grade and completely avoids violating the bone cortex.
Patient positioning must replicate the planned positioning for the definitive resection. If the definitive surgery will be performed in the lateral decubitus position, the biopsy should ideally be performed in that same position to ensure the skin and muscle planes align perfectly with the future surgical approach. Gravity-assisted exsanguination should be used if a tourniquet is applied; Esmarch bandages are strictly contraindicated as the mechanical compression can squeeze tumor cells into the systemic circulation.
Step-by-Step Surgical Approach and Fixation Technique
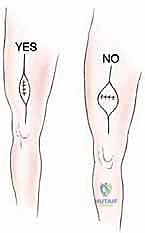
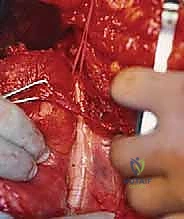
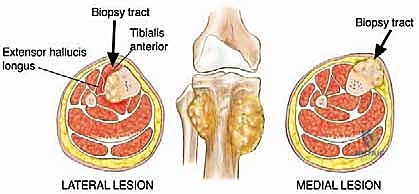
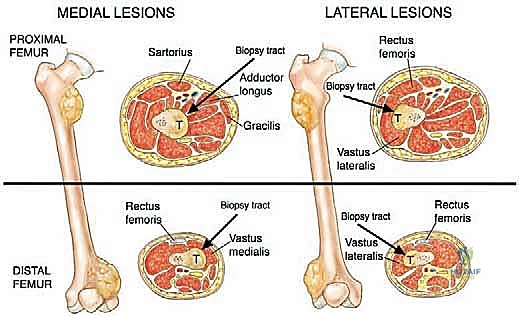
The execution of an open incisional biopsy demands extreme discipline. The incision must be strictly longitudinal, parallel to the long axis of the extremity. Transverse incisions are universally condemned in orthopedic oncology. A longitudinal incision allows for easy extension during the definitive resection and minimizes the width of skin that must be sacrificed when the tract is excised en bloc (typically requiring a 1-2 cm margin of normal skin around the biopsy scar).

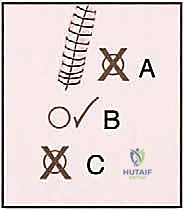
The dissection must proceed directly through the underlying muscle tissue, splitting the muscle fibers longitudinally, rather than dissecting through intermuscular or internervous planes. While standard orthopedic trauma approaches utilize internervous planes to spare muscle function, oncologic biopsy avoids these planes because contaminating a fascial plane between two muscles requires the resection of both muscle compartments during definitive surgery. By going directly through a single muscle belly, contamination is confined to that specific muscle, which will be resected anyway.
Tissue Sampling and Absolute Hemostasis
Once the pseudocapsule is identified, it is sharply incised. A generous wedge of tissue is taken from the periphery of the mass. It is imperative to send a sample for immediate intraoperative frozen section. The purpose of the frozen section is not to obtain a definitive final diagnosis—which is notoriously difficult on frozen tissue—but rather to confirm that the surgeon has obtained viable, diagnostic lesional tissue and not merely necrotic debris or reactive host tissue.