
ABOS Part I Orthopaedic Spine Review: Spondylolisthesis, Disc Herniation & Cauda Equina Syndrome | Part 22305
A 14-year-old competitive gymnast presents with insidious onset low back pain exacerbated by extension and hyperextension activities. Physical examination reveals hamstring tightness and a palpable step-off at L5. AP and lateral radiographs of the lumbar spine show a defect in the pars interarticularis at L5 with an anterior translation of L5 on S1. Which of the following is the most appropriate classification for this condition?
Correct Answer: B
The patient's age, activity (gymnast), pars defect, and anterior translation are classic for an isthmic spondylolisthesis. Wiltse-Newman classification Type II isthmic is characterized by a lesion in the pars interarticularis. Given the insidious onset and high-impact repetitive extension activities, it's most likely a stress fracture (lytic) rather than an acute traumatic fracture (Type IV) or congenital dysplastic anomaly (Type I). Degenerative (Type III) is typically seen in older adults, and pathologic (Type V) is due to bone disease.
Which of the following Meyerding grades of spondylolisthesis indicates a slip of 50-75% of the vertebral body's width?
Correct Answer: C
The Meyerding classification system grades spondylolisthesis based on the percentage of anterior displacement of the superior vertebral body over the inferior one. Grade I is 0-25%, Grade II is 25-50%, Grade III is 50-75%, Grade IV is 75-100%, and Grade V (spondyloptosis) is complete displacement (>100%). Therefore, 50-75% displacement corresponds to Grade III.
A 55-year-old female presents with a long history of low back pain and bilateral leg pain, worse with standing and walking, relieved by sitting or leaning forward. Radiographs show L4-L5 degenerative spondylolisthesis (Grade I) with associated spinal stenosis. She has failed 6 months of comprehensive conservative management including physical therapy, NSAIDs, and epidural steroid injections. Neurological exam reveals mild quadriceps weakness (4+/5) bilaterally but no frank motor deficit. What is the most appropriate next step in management?
Correct Answer: C
For symptomatic degenerative spondylolisthesis with spinal stenosis that has failed conservative management, surgical intervention is often indicated. The Spine Patient Outcomes Research Trial (SPORT) demonstrated superior outcomes for surgical treatment compared to non-operative care in patients with degenerative spondylolisthesis and stenosis. While decompression alone can address stenosis, studies like SPORT have shown that adding fusion to decompression significantly improves outcomes and reduces reoperation rates for degenerative spondylolisthesis, especially in the presence of instability or significant back pain. Quadriceps weakness suggests L4 nerve root compression, making decompression necessary. Anterior fusion alone does not address the posterior decompression requirement. TLIF typically includes decompression. The best option combining decompression and stabilization is decompression with instrumented posterolateral fusion.
Which type of spondylolisthesis is most commonly associated with a sacral spina bifida occulta and a trapezoidal L5 vertebral body?
Correct Answer: A
Type I, or Dysplastic Spondylolisthesis, is a congenital anomaly characterized by malformed sacral facets, an elongated pars, and a trapezoidal L5 vertebral body, often associated with sacral spina bifida occulta. This morphology leads to an inherent instability that predisposes to anterior slippage. The other types have different underlying etiologies.
A 30-year-old male with chronic L5-S1 isthmic spondylolisthesis (Grade II) complains of persistent low back pain and bilateral S1 radiculopathy despite 9 months of conservative treatment. On examination, he has bilateral hamstring tightness and a positive straight leg raise test at 45 degrees. Which of the following imaging modalities is most crucial for evaluating potential nerve root compression and planning surgical decompression?
Correct Answer: C
While plain radiographs define the slip, and CT can better visualize bony stenosis, MRI is superior for evaluating soft tissue structures, including nerve roots, discs, and the spinal cord, and identifying nerve root compression by hypertrophic soft tissue, disc herniation, or foraminal stenosis, which is critical for surgical planning in patients with radiculopathy. EMG assesses nerve function but isn't an imaging modality for structural compression.
What is the primary role of an oblique radiograph in the workup of spondylolisthesis?
Correct Answer: B
Oblique radiographs are specifically used to visualize the pars interarticularis, which appears as the 'neck' of the 'Scottie dog.' A defect or fracture in the pars ('collar on the Scottie dog') is indicative of an isthmic spondylolysis or spondylolisthesis. Other views (AP/Lateral) are better for alignment, slip percentage, and disc space evaluation.
In a pediatric patient with spondylolysis (pars defect without slip) who is asymptomatic, what is the recommended management?
Correct Answer: C
For asymptomatic spondylolysis without slip, the primary recommendation is observation with activity as tolerated. Most pars defects remain stable and asymptomatic. Surgical intervention is reserved for symptomatic, failed conservative cases. Bracing or activity restriction might be considered for symptomatic spondylolysis to promote healing, but not for asymptomatic lesions. Physical therapy is more relevant for symptomatic individuals.
A 68-year-old male with a history of hypertension and diabetes presents with progressively worsening low back pain and L4-L5 neurogenic claudication. He has a Grade I degenerative spondylolisthesis at L4-L5. His pain is 7/10 on the VAS. He has tried epidural steroid injections, NSAIDs, and physical therapy for 9 months with no sustained relief. What is the strongest indicator for surgical intervention in this patient?
Correct Answer: C
The strongest indicator for surgical intervention in symptomatic degenerative spondylolisthesis is the failure of a prolonged course of conservative management combined with persistent severe symptoms (pain, neurological deficits) impacting quality of life. While neurogenic claudication itself is a symptom, its persistence despite non-operative efforts is the key factor. The grade of slip alone isn't an indication for surgery, nor are comorbidities unless they contraindicate surgery. Age is a factor for surgical risk but not an indication for surgery.
What is the most common neurological complication following reduction of a high-grade spondylolisthesis?
Correct Answer: B
The L5 nerve root is most vulnerable during the reduction of a high-grade L5-S1 spondylolisthesis. This is due to its course over the sacral ala and the potential for stretch injury during the reduction maneuver, especially with attempts to correct lumbosacral kyphosis. While other nerve injuries can occur, L5 radiculopathy/palsy is the most frequently reported neurological complication.
Which of the following describes the anatomical defect in Type IIB isthmic spondylolisthesis?
Correct Answer: A
Wiltse-Newman Type II isthmic spondylolisthesis is subdivided: Type IIA is a lytic (stress) fracture of the pars, Type IIB is an elongated but intact pars (often a healed stress fracture with elongation), and Type IIC is an acute fracture of the pars. Therefore, Type IIB specifically refers to an elongated pars without a clear lytic defect.
A 37-year-old male presents with back and left lower limb pain, suspected 'slipped disc'. During the initial evaluation, which of the following findings would be the MOST concerning red flag, necessitating immediate further investigation for a serious spinal pathology?
Correct Answer: D
The case explicitly lists 'Urinary retention', 'Faecal incontinence', 'Saddle area numbness and loss of anal tone', and 'Widespread neurological signs' as characteristics of Cauda Equina Syndrome (CES). The importance of detecting CES early is highlighted, with early intervention (< 24 hours) shown to improve outcome. Acute onset of urinary retention and saddle anesthesia are hallmark symptoms of CES, representing a surgical emergency requiring immediate investigation and intervention. Options A, B, C, and E are typical signs and symptoms of radiculopathy, which, while requiring appropriate management, do not represent the same level of immediate neurological emergency as CES.
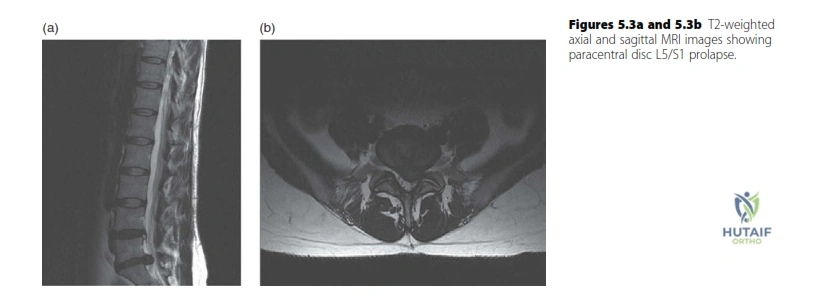
A 37-year-old male presents with left lower limb radiculopathy. An MRI is performed. Review the provided T2-weighted MRI scan of the lumbar spine.
Based on the image and the case description, what is the most likely diagnosis and affected nerve root?
Correct Answer: C
The case explicitly states that the MRI shows 'a paracentral disc prolapse at the L5/S1 level'. The background knowledge section on 'Exiting nerve roots in the cervical and lumbar spine' further clarifies that for a common 'paracentral' disc prolapse at the L5/S1 level, it is the S1 'traversing' nerve root that is most commonly compressed. Therefore, an L5/S1 paracentral disc prolapse affecting the S1 nerve root is the most accurate diagnosis based on the provided information.
A 37-year-old male is diagnosed with a left L5/S1 paracentral disc prolapse. Based on the expected S1 nerve root compression, which combination of physical exam findings is most consistent with this diagnosis?
Correct Answer: C
The candidate's expected findings for an L5/S1 disc prolapse are explicitly stated: 'I would expect the pain, paraesthesia and numbness to be in an S1 distribution (posterior calf, heel and lateral border of the foot) on the left. There may be an associated subjective decreased sensation in the same distribution, a decreased ankle jerk on that side...' The S1 nerve root primarily innervates the muscles responsible for ankle plantarflexion and mediates the Achilles reflex (ankle jerk). Sensory distribution for S1 includes the posterior calf, heel, and lateral border of the foot. Therefore, weakness in ankle plantarflexion, numbness over the lateral foot/heel, and a diminished Achilles reflex are the classic findings for S1 radiculopathy.
A 45-year-old patient presents with acute low back pain and bilateral leg weakness. To definitively diagnose Cauda Equina Syndrome, which of the following clinical findings is considered a hallmark symptom?
Correct Answer: D
The case explicitly lists 'Urinary retention' and 'Faecal incontinence' as key characteristics of Cauda Equina Syndrome. These symptoms, along with saddle area numbness and loss of anal tone, are considered hallmark signs of CES, indicating significant compression of the sacral nerve roots. While options A, B, C, and E can be present in various spinal pathologies, including severe radiculopathy, new onset urinary retention or overflow incontinence is a critical red flag that mandates immediate investigation for CES.
A 50-year-old patient presents with a 12-hour history of saddle anesthesia, new-onset urinary retention, and progressive bilateral lower extremity weakness. An MRI confirms a large acute disc prolapse causing Cauda Equina Syndrome. What is the most appropriate immediate management strategy?
Correct Answer: C
The case emphasizes the critical importance of timely intervention for Cauda Equina Syndrome, stating: 'The importance of detecting cauda equina syndrome early is that early intervention (< 24 hours) has been shown to improve outcome.' Given the acute onset of hallmark CES symptoms (saddle anesthesia, urinary retention, bilateral weakness) and MRI confirmation, urgent surgical decompression is indicated to prevent permanent neurological deficits. Options A, B, D, and E represent conservative or delayed management strategies that are inappropriate and potentially harmful in the setting of acute CES.
A 62-year-old patient presents with symptoms consistent with an L4/L5 paracentral disc prolapse. Based on the typical anatomical relationships described in the case, which nerve root is most commonly affected by this type of disc herniation?
Correct Answer: C
The 'Exiting nerve roots in the cervical and lumbar spine' section explicitly clarifies the anatomical relationship: 'The knowledge that the L4 nerve root exits the spinal canal below the L4 pedicle may (incorrectly) lead the candidate to expect the L4 nerve root to be compressed when a disc prolapse occurs below the L4 vertebra in the L4/5 interspace. It is best to think of this nerve root as ‘already having left the canal’ and therefore it is the L5 ‘traversing’ nerve root that is most commonly compressed by the common ‘paracentral’ disc prolapse. ... Thus an L4/5 disc prolapse commonly affects the L5 nerve root.'
A 48-year-old patient presents with right arm pain and weakness. MRI reveals a disc prolapse at the C5/C6 level. According to the anatomical principles outlined in the case, which nerve root is most likely compressed?
Correct Answer: C
The 'Exiting nerve roots in the cervical and lumbar spine' section details the unique nomenclature in the cervical spine: 'In the cervical spine, a prolapsed disc typically affects the exiting nerve root at that level (there is no traversing nerve root because the roots leave the spinal cord and exit the canal almost horizontally). But there is a nomenclature change in the cervical spine. Because the C6 nerve root exits above (not below) the C6 vertebra this double change means a prolapsed cervical disc at the C5/C6 level most commonly affects the C6 nerve root.'
A patient's MRI report describes a disc herniation where the displaced disc material has a narrow 'neck' at its base but remains in continuity with the parent disc. According to the nomenclature provided, how would this specific type of disc herniation be classified?
Correct Answer: C
The 'Nomenclature' section defines different types of disc herniation. It states: 'A focal disc herniation may be described as a protrusion or extrusion. An extruded disc has a narrow ‘neck’ at its base. Extruded disc material is sequestrated if it is no longer in continuity with the disc.' The description in the question, 'displaced disc material has a narrow 'neck' at its base but remains in continuity with the parent disc,' perfectly matches the definition of an extrusion.
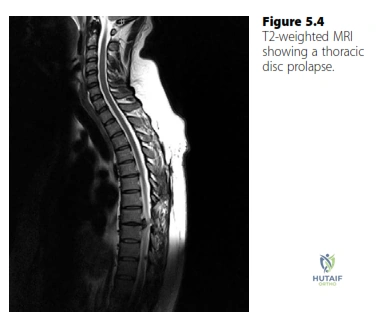
A 55-year-old patient presents with progressive upper extremity weakness, gait disturbance, and thoracic back pain. MRI reveals a calcified thoracic disc prolapse at T8/T9 causing spinal cord compression. Based on the case information, what is the recommended surgical approach for this condition?
Correct Answer: C
The 'Disc prolapse background knowledge' section specifically addresses thoracic disc prolapse: 'A thoracic disc prolapse (rare) will typically present with symptoms and signs of spinal cord compression associated with thoracic back pain... The discs are usually calcified and require decompression from the front. Treatment therefore is via a thoracotomy and partial vertebrectomy.' This indicates that an anterior approach via thoracotomy and partial vertebrectomy is the standard surgical treatment for thoracic disc prolapse causing spinal cord compression.
A 37-year-old male with a left L5/S1 paracentral disc prolapse causing S1 radiculopathy has been managed conservatively for 8 weeks with physical therapy and NSAIDs. His symptoms have shown minimal improvement, and he continues to experience significant pain and functional limitation. What is the most appropriate next step in his management?
Correct Answer: B
The candidate's proposed treatment plan for a lumbar disc prolapse states: 'Initially conservatively as the natural history of most lumbar disc prolapses is that they resolve with time. If it has not resolved after 6–12 weeks of conservative management I would offer the patient microdiscectomy.' Given that the patient has undergone 8 weeks of conservative management with minimal improvement, he falls within the 6-12 week window where surgical intervention (microdiscectomy) would be offered. While epidural steroid injections (Option E) are a common non-surgical intervention, the case specifically outlines microdiscectomy as the next step after 6-12 weeks of failed conservative management. Continuing conservative management for another 6 months (Option A) would be excessively prolonged given the persistent symptoms. Options C and D are not the primary next steps in this scenario.
In classical degenerative spondylolisthesis at this typical level, which of the following anatomic factors is most strongly predictive of progression?
A 45-year-old male presents with acute severe back pain, bilateral sciatica, and new-onset urinary retention. Imaging confirms a massive L4-L5 central disc extrusion. What is the most appropriate next step in management?
A 65-year-old male with neurogenic claudication is found to have an L4-L5 degenerative spondylolisthesis. Which of the following findings on dynamic flexion-extension radiographs is the most widely accepted threshold to define dynamic instability, thereby strongly supporting the addition of fusion to a surgical decompression?
None
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding abos-part-i-comprehensive-review-batch-101-2