ABOS Part I & AAOS OITE Orthopaedic Review: Cervical Spine Trauma & Proximal Humerus Fractures | Part 21580

Key Takeaway
This module provides a comprehensive review for the ABOS Part I and AAOS OITE examinations. It features 21 advanced multiple-choice questions covering high-yield topics in cervical spine trauma, including facet dislocations and spinal cord injury management, alongside detailed coverage of proximal humerus fractures, their classification, surgical approaches, and rehabilitation protocols.
ABOS Part I & AAOS OITE Orthopaedic Review: Cervical Spine Trauma & Proximal Humerus Fractures | Part 21580
A 32-year-old male presents to the emergency department after a high-speed motor vehicle collision, sustaining a bilateral C6-C7 facet dislocation. He is neurologically intact but complains of severe neck pain and inability to move his head. Which of the following statements accurately describes the typical mechanism of injury and associated ligamentous damage in this patient's condition?
Correct Answer: C
Bilateral cervical facet dislocations are severe, high-energy injuries typically resulting from a combination of hyperflexion and distraction forces. This mechanism leads to complete, catastrophic disruption of the posterior ligamentous complex (PLC), which includes the ligamentum flavum, interspinous ligaments, supraspinous ligaments, and facet joint capsules. The posterior longitudinal ligament (PLL) and the intervertebral disc annulus are also frequently compromised. This aligns with Stage 3 or Stage 4 of the Allen and Ferguson mechanistic classification for Distraction-Flexion injuries.
Option A describes the typical mechanism for a unilateral facet dislocation, which involves flexion-rotation and generally less severe ligamentous disruption. Option B describes a hyperextension injury, which primarily affects the anterior column and ligaments. Option D describes a burst fracture, which is an axial compression injury. Option E describes a shear injury, which is less common for isolated bilateral facet dislocations.
A 55-year-old male falls from a ladder, sustaining a bilateral C5-C6 facet dislocation with significant anterior translation. He presents with an ASIA C incomplete spinal cord injury. The provided image illustrates the complex anatomical relationships in the cervical spine during a dislocation event.
Considering the biomechanics of this injury, which of the following structures is most critically compromised, leading to the profound instability observed?

Correct Answer: E
The Posterior Ligamentous Complex (PLC) is the primary tension band of the cervical spine, comprising the ligamentum flavum, interspinous ligaments, supraspinous ligaments, and the facet joint capsules. In bilateral cervical facet dislocation, the severe hyperflexion and distraction forces cause complete, catastrophic disruption of the PLC. While the Anterior Longitudinal Ligament (ALL), Posterior Longitudinal Ligament (PLL), and Intervertebral Disc Annulus Fibrosus are also frequently compromised (often stripped or torn), the complete failure of the PLC is the hallmark of this injury, leading to the profound instability and anterior translation of the superior vertebral body. The Ligamentum Flavum (C) is a component of the PLC, but the entire complex's disruption is the most critical factor.
A 28-year-old male is brought to the trauma bay after a diving accident, presenting with a bilateral C4-C5 facet dislocation and an ASIA A complete spinal cord injury. He is intubated and sedated, making a reliable neurological examination impossible. Which of the following is the most appropriate next step in his management regarding imaging and potential reduction?
Correct Answer: C
The timing of magnetic resonance imaging (MRI) in relation to closed reduction is critical. For awake, alert, and cooperative patients, rapid closed reduction via cranial traction can be attempted prior to MRI, provided serial neurological examinations are performed. However, if the patient is uncooperative, intoxicated, or comatose (as in this intubated and sedated patient with an ASIA A injury), MRI must be obtained prior to any reduction attempt. This is to evaluate for a traumatic disc herniation, which occurs in 30-60% of cases. If a massive disc herniation is present, an anterior cervical discectomy must be performed before reduction to prevent catastrophic cord compression from retropulsed disc material.
Option A is incorrect because attempting closed reduction in an obtunded patient without prior MRI carries a high risk of iatrogenic neurological deterioration. Option B is incorrect as further imaging is crucial for surgical planning and safety. Option D (CTA) is important if there's suspicion of vertebral artery injury, but MRI for disc herniation takes precedence before reduction in this scenario. Option E (methylprednisolone) is no longer routinely recommended for acute spinal cord injury due to lack of clear benefit and potential side effects.
A 40-year-old patient with a C6-C7 bilateral facet dislocation and a large traumatic disc herniation on MRI is scheduled for an anterior cervical discectomy and fusion (ACDF). During the approach, the surgeon identifies the internervous plane. Which anatomical structures define this plane for a standard Smith-Robinson approach?
Correct Answer: B
The standard Smith-Robinson anterior cervical approach utilizes an internervous plane to access the cervical spine. This plane is developed between the sternocleidomastoid muscle and the carotid sheath (containing the common carotid artery, internal jugular vein, and vagus nerve) laterally, and the strap muscles (sternohyoid, sternothyroid, omohyoid), trachea, and esophagus medially. This approach minimizes muscle transection and allows for safe access to the prevertebral fascia and anterior cervical spine.
Option A describes a deeper plane after the prevertebral fascia is exposed. Option C describes the initial incision through superficial layers. Options D and E describe structures within or adjacent to the vertebral column, not the primary internervous plane for the approach.
A 60-year-old patient with a C5-C6 bilateral facet dislocation, without evidence of disc herniation on MRI, undergoes a posterior approach for reduction and stabilization. The surgeon plans to perform lateral mass screw fixation.
Based on the provided image and standard techniques, which of the following describes the Magerl technique for lateral mass screw placement at C5?
Correct Answer: B
The Magerl technique for lateral mass screw placement is a widely accepted method designed to maximize screw purchase while minimizing the risk of neurovascular injury. The starting point is typically 1 millimeter medial and 1 millimeter cephalad to the center of the lateral mass. The trajectory is 25 degrees lateral (to avoid the vertebral artery, which lies anterior and medial to the lateral mass) and parallel to the superior articular facet in the sagittal plane (typically 20 to 30 degrees cephalad, avoiding the exiting nerve root). This trajectory aims to engage the thickest part of the lateral mass.
Option A describes the Roy-Camille technique, which uses a central starting point and a straight anterior trajectory. The other options describe incorrect starting points or trajectories that would increase the risk of vertebral artery or nerve root injury.
A 48-year-old male undergoes an anterior cervical discectomy and fusion (ACDF) for a C5-C6 bilateral facet dislocation. Postoperatively, he develops hoarseness and difficulty swallowing. Which of the following complications is most likely responsible for his symptoms, and what is its typical management?
Correct Answer: C
Hoarseness is a classic symptom of recurrent laryngeal nerve (RLN) palsy, which can occur during an anterior cervical approach due to retraction or direct injury to the nerve. Dysphagia (difficulty swallowing) is also a common complication, often transient, resulting from esophageal retraction and irritation during the anterior approach. Both complications are relatively common (RLN palsy 1-5%, dysphagia 10-30%) and are usually transient, resolving spontaneously within weeks to months. Management is typically conservative, involving speech therapy evaluation for dysphagia and vocal cord assessment for hoarseness. Severe or persistent cases may require further intervention.
Option A (C5 nerve root palsy) presents as deltoid and biceps weakness, not hoarseness or dysphagia. Option B (vertebral artery injury) would present with signs of posterior circulation stroke or significant hemorrhage. Option D (epidural hematoma) would typically cause acute neurological deterioration, not isolated hoarseness and dysphagia. Option E (hardware failure) is a long-term mechanical complication, not an acute postoperative neurological or soft tissue issue.
A 22-year-old patient with an ASIA B C6 incomplete spinal cord injury following a bilateral C6-C7 facet dislocation undergoes successful surgical stabilization within 12 hours of injury. In the immediate postoperative period, what is the most critical hemodynamic management goal to optimize spinal cord perfusion and minimize secondary injury?
Correct Answer: B
Current guidelines for the management of acute spinal cord injury (SCI) emphasize maintaining adequate spinal cord perfusion to minimize the penumbra of ischemic secondary injury. This is achieved by maintaining the Mean Arterial Pressure (MAP) greater than 85 mmHg for at least 7 days post-injury. This hemodynamic target helps ensure sufficient blood flow to the injured spinal cord, which is particularly vulnerable to ischemia.
Option A is incorrect; maintaining a low SBP would compromise spinal cord perfusion. Option C is incorrect; heart rate is not the primary hemodynamic target for SCI. Option D is incorrect; fluid restriction could lead to hypovolemia and compromise MAP. Option E is incorrect; DVT prophylaxis should be initiated within 72 hours of surgery, provided there is no evidence of expanding epidural hematoma, to prevent thromboembolic complications, which are common in SCI patients.
A 70-year-old patient presents after a ground-level fall with a bilateral C4-C5 facet dislocation. Imaging confirms complete disruption of the posterior ligamentous complex. Neurological examination reveals an ASIA D incomplete spinal cord injury. Based on the Subaxial Cervical Spine Injury Severity (SLIC) score, what is the minimum score assigned to this injury, and what does it indicate regarding management?
Correct Answer: C
The Subaxial Cervical Spine Injury Severity (SLIC) score is a validated algorithm for surgical decision-making. For a bilateral facet dislocation, the score components are:
- Injury Morphology: Bilateral facet dislocation is considered a translational/rotational injury, scoring 3 points.
- Discoligamentous Complex Integrity: Complete disruption of the posterior ligamentous complex scores 2 points.
- Neurological Status: An ASIA D incomplete spinal cord injury scores 3 points.
Therefore, the total SLIC score for this patient is 3 (morphology) + 2 (PLC) + 3 (neurological status) = 8 points. A SLIC score of 5 or greater mandates surgical intervention. Thus, a score of 8 points strongly mandates surgical stabilization.
A patient presents with a bilateral C5-C6 facet dislocation. On lateral cervical spine radiography, which of the following findings is most characteristic of this injury type, indicating profound instability?
Correct Answer: C
Bilateral cervical facet dislocation is characterized by profound instability due to complete disruption of the posterior ligamentous complex. Radiographically, this manifests as significant anterior translation of the superior vertebral body on the inferior one, often exceeding 50% of the vertebral body width on lateral radiography. The inferior articular processes of the superior vertebra translate anteriorly and superiorly over the superior articular processes of the inferior vertebra, ultimately dropping into the intervertebral foramina, creating a locked configuration.
Option A describes less severe instability. Option B describes a purely ligamentous injury without facet dislocation. Option D describes a flexion teardrop fracture, which is a different injury pattern. Option E describes a stable injury, which is not characteristic of a bilateral facet dislocation.
The management of acute spinal cord injury (SCI) associated with bilateral cervical facet dislocation has evolved significantly. Which landmark study provided compelling evidence supporting early surgical decompression (within 24 hours of injury) for improved neurological outcomes in patients with SCI?
Correct Answer: D
The Surgical Timing in Acute Spinal Cord Injury Study (STASCIS) was a pivotal prospective, multicenter cohort study that demonstrated the significant benefit of early surgical decompression (within 24 hours of injury) in patients with acute spinal cord injury. The study found that early intervention resulted in significantly improved neurological outcomes at 6-month follow-up compared to delayed decompression, without an increase in complication rates. This study fundamentally shifted the paradigm towards emergent surgical intervention for spinal cord injuries, including those associated with bilateral facet dislocations.
Option A (Panjabi and White) provided foundational biomechanical understanding of spinal instability. Option B (Allen and Ferguson) developed a mechanistic classification system for cervical spine injuries. Option C (SLIC score) provides a validated algorithm for surgical decision-making. While all these are important contributions to spine trauma, STASCIS specifically addressed the timing of surgery for SCI.
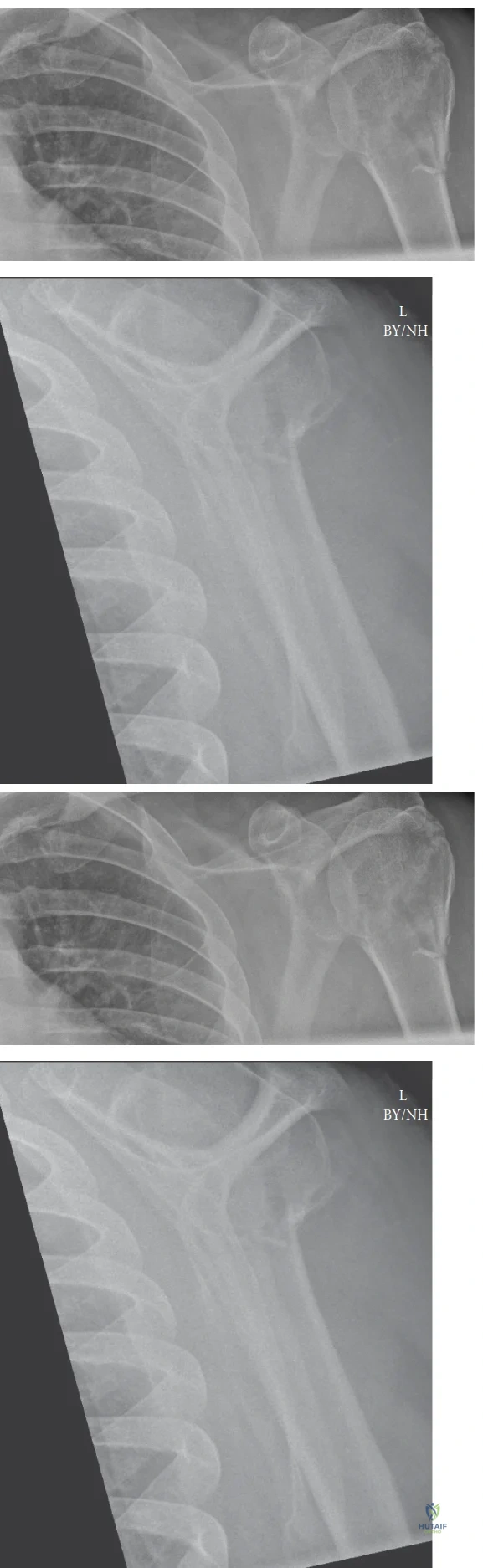
A 72-year-old female presents to the emergency department after a low-energy fall onto her outstretched arm. Radiographs reveal a displaced fracture of the surgical neck of the humerus with the humeral head in a valgus-impacted position, demonstrating less than 1 cm displacement and approximately 30 degrees of angulation. She has a past medical history of well-controlled hypertension and osteoporosis. She lives independently and has moderate functional demands, enjoying gardening and light housework. On examination, she has intact neurovascular status, but significant pain with any shoulder movement.
Based on the Neer classification system and the provided case details, what is the most appropriate initial management strategy for this patient?
Correct Answer: D
The patient presents with a displaced surgical neck fracture, but the description notes it is 'valgus-impacted' with 'less than 1 cm displacement and approximately 30 degrees of angulation.' According to the case content, non-operative management is the treatment of choice for the majority of proximal humerus fractures, particularly one-part fractures, and often for two-part surgical neck fractures in elderly, low-demand patients with minimal displacement. Minimally displaced or nondisplaced fractures are generally defined as <1 cm displacement and <45 degrees angulation. Stable, valgus-impacted fractures also fall under non-operative indications. While she has moderate functional demands, her age, osteoporosis, and the relatively stable, minimally displaced nature of the valgus-impacted fracture make non-operative management a strong initial consideration, especially given the PROXIMAL trial's findings suggesting comparable outcomes for many displaced fractures in older populations.
- Option A (ORIF with a locking plate): While ORIF is indicated for significantly displaced two-part surgical neck fractures, this patient's fracture is described as minimally displaced and valgus-impacted, which are features favoring non-operative care. The PROXIMAL trial specifically questioned the superiority of ORIF over non-operative treatment for many displaced fractures in older adults.
- Option B (Hemiarthroplasty): Hemiarthroplasty is typically reserved for highly comminuted four-part fractures, head-splitting fractures, or severe osteopenia preventing stable fixation, especially in older patients. This is a two-part surgical neck fracture, not a complex four-part or head-splitting injury.
- Option C (Reverse total shoulder arthroplasty): RTSA is increasingly favored for complex four-part fractures in elderly patients, particularly with a compromised or irreparable rotator cuff, or severe osteopenia. It is an overtreatment for a minimally displaced two-part surgical neck fracture.
- Option E (Urgent closed reduction and percutaneous pinning): While percutaneous pinning can be used for some two-part fractures, the description of 'valgus-impacted' and 'minimally displaced' suggests inherent stability that may not require surgical reduction and pinning, especially as an urgent initial step over non-operative assessment.
A 58-year-old male sustains a high-energy fall, resulting in a Neer three-part fracture of the proximal humerus involving the surgical neck and greater tuberosity, with significant displacement of both fragments relative to the humeral head. He is otherwise healthy and has high functional demands. During surgical planning, the orthopedic surgeon is particularly concerned about the risk of avascular necrosis (AVN) of the humeral head. Which of the following anatomical structures is most critical for the primary blood supply to the humeral head and its disruption significantly increases the risk of AVN?
Correct Answer: B
The case content explicitly states: 'The blood supply to the humeral head is predominantly from the ascending branch of the anterior circumflex humeral artery, forming the arcuate artery, which penetrates the head near the bicipital groove. The posterior circumflex humeral artery also contributes. Disruption of these vessels, particularly in multi-part fractures with significant displacement, is a major risk factor for AVN.'
- Option A (Posterior circumflex humeral artery): While the posterior circumflex humeral artery does contribute to the humeral head's blood supply, the anterior circumflex humeral artery and its ascending branch are described as the 'predominant' supply.
- Option C (Thoracoacromial artery): The thoracoacromial artery supplies the pectoralis major, deltoid, and clavicle, but not directly the humeral head.
- Option D (Suprascapular artery): The suprascapular artery supplies the supraspinatus and infraspinatus muscles and the shoulder joint, but is not the primary supply to the humeral head itself.
- Option E (Subscapular artery): The subscapular artery is a branch of the axillary artery that supplies the subscapularis, latissimus dorsi, and teres major muscles, but not the humeral head's primary vascularity.
A 35-year-old male undergoes open reduction and internal fixation (ORIF) of a displaced two-part surgical neck fracture of the humerus via a deltopectoral approach. Post-operatively, the patient complains of numbness and weakness in his shoulder. On examination, he has difficulty initiating abduction and has sensory loss over the lateral aspect of his deltoid. Which of the following nerves was most likely injured during the surgical procedure or due to the initial trauma?
Correct Answer: D
The case content states: 'Axillary Nerve: Most commonly injured nerve in PHFs or during surgical approaches. It wraps around the surgical neck, approximately 5-7 cm distal to the acromion, innervating the deltoid and teres minor.' The symptoms described—difficulty initiating abduction (deltoid weakness) and sensory loss over the lateral aspect of the deltoid (axillary nerve sensory distribution)—are classic signs of axillary nerve injury.
- Option A (Musculocutaneous nerve): This nerve supplies the biceps and brachialis, responsible for elbow flexion and forearm supination. Injury would present with weakness in these movements and sensory loss over the lateral forearm.
- Option B (Radial nerve): The radial nerve is located more distally and posteriorly in the spiral groove. It innervates the triceps and wrist/finger extensors. Injury would cause wrist drop and sensory loss over the posterior forearm and hand.
- Option C (Ulnar nerve): The ulnar nerve primarily innervates intrinsic hand muscles and flexor carpi ulnaris. Injury would result in claw hand deformity and sensory loss over the medial hand.
- Option E (Median nerve): The median nerve innervates forearm flexors and thenar muscles. Injury would cause 'ape hand' deformity and sensory loss over the radial aspect of the palm and fingers.
A 68-year-old female with severe osteoporosis presents with a comminuted Neer four-part proximal humerus fracture. She is scheduled for surgical management. During pre-operative planning, the surgeon emphasizes the critical importance of achieving and maintaining medial calcar support during fixation. What is the primary biomechanical reason for this emphasis?
Correct Answer: C
The case content explicitly highlights the importance of the medial calcar under the 'Biomechanics' section: 'Medial Calcar: This dense trabecular bone region acts as a crucial weight-bearing structure, resisting varus collapse and providing critical support for internal fixation. Loss of medial calcar support significantly increases the risk of screw cutout and construct failure.' It is also mentioned under 'Complications' that 'inadequate medial support (calcar screws)' is a risk factor for screw cutout.
- Option A (To prevent impingement of the rotator cuff tendons): While proper plate positioning is important to prevent impingement, the medial calcar's primary role is not impingement prevention but structural support.
- Option B (To ensure adequate blood supply to the humeral head and prevent avascular necrosis): The integrity of the medial calcar metaphyseal extension and its periosteal attachments is vital for vascularity, but the primary biomechanical reason for supporting the calcar is to resist varus collapse, not directly to ensure blood supply. The main blood supply is from the anterior circumflex humeral artery.
- Option D (To facilitate early active range of motion and reduce post-operative stiffness): While stable fixation generally allows for earlier rehabilitation, the direct biomechanical role of the medial calcar is not to facilitate early ROM but to provide structural stability to the construct.
- Option E (To protect the axillary nerve from iatrogenic injury during screw placement): The axillary nerve is at risk during lateral plate placement and screw insertion, but the medial calcar's role is not nerve protection.
A 78-year-old active female presents with a complex, comminuted four-part proximal humerus fracture with significant displacement and severe osteopenia. She has a pre-existing rotator cuff tear that was symptomatic prior to her fall. She is physiologically fit for surgery and desires the best possible functional outcome. Considering the patient's age, fracture pattern, bone quality, and pre-existing rotator cuff pathology, which surgical option is most likely to provide predictable pain relief and functional improvement?
Correct Answer: E
The case content, particularly the 'Summary of Key Literature / Guidelines' section, strongly supports RTSA in this scenario: 'Reverse Total Shoulder Arthroplasty (RTSA) has gained significant traction, especially in elderly patients with complex PHFs, pre-existing rotator cuff dysfunction, or severe osteopenia. Multiple studies demonstrate more predictable pain relief and functional outcomes with RTSA compared to hemiarthroplasty or ORIF in this specific demographic, as it bypasses the need for tuberosity healing and relies on the deltoid for elevation.' This patient fits all these criteria: elderly, complex four-part fracture, severe osteopenia, and pre-existing rotator cuff tear.
- Option A (ORIF with a locking plate and suture augmentation): While LPO is the gold standard for many complex PHFs, severe osteopenia and a pre-existing rotator cuff tear significantly increase the risk of fixation failure (screw cutout, nonunion of tuberosities) and poor functional outcomes, as the rotator cuff is essential for ORIF success.
- Option B (Hemiarthroplasty with tuberosity repair): Hemiarthroplasty has historically been an option for complex four-part fractures in older patients. However, outcomes can be variable and are often limited by tuberosity healing and rotator cuff function. Given the pre-existing rotator cuff tear, tuberosity healing and function would be severely compromised, making RTSA a superior choice.
- Option C (Non-operative management with sling immobilization): For a complex, comminuted four-part fracture with significant displacement in an active patient, non-operative management would likely lead to severe malunion, pain, and very poor function.
- Option D (Intramedullary nailing): Intramedullary nailing is less common for complex PHFs and is typically used for select two-part surgical neck fractures. It would be inadequate for a comminuted four-part fracture, especially with tuberosity involvement and osteopenia.
A 55-year-old male is undergoing open reduction and internal fixation of a displaced three-part proximal humerus fracture via a deltopectoral approach. The surgical team has positioned the patient as shown in the image below. During the approach, the surgeon identifies the cephalic vein in the deltopectoral groove. Which of the following statements accurately describes the management of the cephalic vein and the anatomical plane it defines?
Correct Answer: C
The case content describes the deltopectoral approach: 'Identify the cephalic vein running in the deltopectoral groove. This is the key internervous plane. The deltoid muscle is lateral (innervated by the axillary nerve), and the pectoralis major muscle is medial (innervated by the medial and lateral pectoral nerves). The cephalic vein is typically retracted laterally with the deltoid, but can be ligated and divided if necessary for better exposure...'
- Option A: While the vein can be ligated, it's typically retracted first. More importantly, it does not lie between the pectoralis minor and coracobrachialis.
- Option B: The cephalic vein is typically retracted laterally with the deltoid, not medially with the pectoralis major. The internervous plane description is correct, but the retraction direction is wrong.
- Option D: The cephalic vein is retracted laterally with the deltoid, but the plane is between the deltoid and pectoralis major, not deltoid and teres major.
- Option E: While the vein can be ligated, it lies in the deltopectoral groove, superficial to the deeper structures, but the axillary nerve is deeper and more distal, wrapping around the surgical neck. The vein is not directly superficial to the axillary nerve in the groove.
A 42-year-old male presents with a displaced greater tuberosity fracture of the proximal humerus after a snowboarding accident. Radiographs show the greater tuberosity fragment displaced superiorly by 8 mm. He is an active individual with high functional demands. During surgical planning for open reduction and internal fixation (ORIF), the surgeon considers the deforming forces acting on the fracture fragments. Which muscle is primarily responsible for the superior displacement of the greater tuberosity fragment?
Correct Answer: D
The case content, under 'Biomechanics - Deforming Forces,' explicitly states: 'Supraspinatus: Pulls the greater tuberosity superiorly and posteriorly.' The greater tuberosity is the insertion site for the supraspinatus, infraspinatus, and teres minor tendons. Superior displacement is a classic sign of supraspinatus pull.
- Option A (Subscapularis): The subscapularis inserts into the lesser tuberosity and pulls it anteriorly and medially.
- Option B (Pectoralis major): The pectoralis major inserts more distally on the humerus and contributes to adduction and internal rotation of the shaft.
- Option C (Deltoid): The deltoid pulls the humeral shaft proximally and laterally.
- Option E (Latissimus dorsi): The latissimus dorsi inserts more distally on the humerus and contributes to adduction, extension, and internal rotation of the shaft.
A 62-year-old male undergoes open reduction and internal fixation (ORIF) with a locking plate for a displaced three-part proximal humerus fracture. Post-operatively, radiographs show good reduction and hardware placement. However, at his 6-month follow-up, he presents with increasing pain, loss of reduction, and new varus collapse of the humeral head, with screws appearing to have migrated through the superior aspect of the humeral head. Which of the following is the most likely primary cause of this complication?
Correct Answer: B
The patient's presentation of 'loss of reduction, and new varus collapse of the humeral head, with screws appearing to have migrated through the superior aspect of the humeral head' is a classic description of screw cutout and construct failure due to varus collapse. The case content explicitly states under 'Complications': 'Screw Cutout / Implant Failure... Etiology / Risk Factors: Osteoporotic bone, inadequate medial support (calcar screws), varus collapse, premature weight-bearing, poor screw purchase, poor reduction.' Inadequate medial calcar support is a critical factor in resisting varus collapse and preventing screw cutout.
- Option A (Iatrogenic axillary nerve injury during surgery): Axillary nerve injury would cause deltoid weakness and sensory loss, but not directly lead to varus collapse or screw cutout.
- Option C (Development of a deep surgical site infection): While infection is a serious complication, it typically presents with signs of inflammation, fever, and wound drainage, and while it can lead to nonunion or implant loosening, it's not the primary mechanism for acute varus collapse and screw cutout as described.
- Option D (Premature and aggressive post-operative rehabilitation): While this can contribute to implant failure, the fundamental structural weakness often stems from inadequate initial fixation, particularly medial support, which allows the varus collapse to initiate.
- Option E (Failure to repair the rotator cuff tendons to the plate): Suture augmentation of tuberosities is important for tuberosity healing and stability, but its absence is less directly linked to varus collapse of the humeral head and screw cutout than the lack of medial calcar support.
A 28-year-old male sustains a high-energy Neer four-part fracture-dislocation of the proximal humerus. He is scheduled for urgent open reduction and internal fixation. During pre-operative planning, the surgeon reviews the imaging, including a CT scan with 3D reconstructions. What is the primary advantage of using a CT scan with 3D reconstructions in this specific fracture pattern?
Correct Answer: C
The case content, under 'Pre-Operative Planning - Imaging,' states: 'Computed Tomography (CT) Scan: Indispensable for complex fractures, particularly three- and four-part fractures, fracture-dislocations, and head-splitting injuries. Provides detailed information on comminution, articular involvement, glenoid impression fractures, and precise tuberosity displacement. 3D reconstructions are invaluable for understanding fracture morphology and planning reduction maneuvers.'
- Option A (To assess for rotator cuff integrity and associated ligamentous injuries): MRI is generally better for assessing soft tissue structures like the rotator cuff and ligaments.
- Option B (To evaluate for brachial plexus pathology): While CT can show bony impingement, MRI or electrodiagnostic studies are more definitive for brachial plexus pathology.
- Option D (To confirm the presence of a fracture-dislocation, which is typically missed on standard radiographs): While CT can confirm, standard radiographs (AP, scapular Y, axillary lateral) are usually sufficient for initial diagnosis of fracture-dislocation. CT provides more detail, not just confirmation.
- Option E (To determine the extent of avascular necrosis (AVN) of the humeral head): AVN is a complication that develops over time. While CT can show signs of AVN in later stages, it's not the primary acute indication for CT in a fresh fracture-dislocation.
A 70-year-old female undergoes open reduction and internal fixation of a displaced two-part surgical neck fracture. She is placed in the beach chair position for the procedure, as depicted in the general surgical setup shown in the image. Which of the following is a critical precaution to take when positioning a patient in the beach chair position for shoulder surgery?
Correct Answer: B
The case content, under 'Patient Positioning - Beach Chair Position,' explicitly states: 'Precautions: Ensure adequate padding to all pressure points, especially the contralateral elbow, sacrum, and heels. Monitor blood pressure closely for potential cerebral hypoperfusion ('beach chair hypotension').'
- Option A (Ensuring the operative arm is tightly adducted to prevent nerve stretch): The operative arm is typically draped free to allow full manipulation, and tight adduction is not a standard precaution; rather, care is taken to avoid excessive traction or positioning that could stretch nerves.
- Option C (Placing an axillary roll under the dependent axilla to prevent brachial plexus compression): An axillary roll is a critical precaution for the lateral decubitus position, not typically for the beach chair position where the patient is semi-recumbent.
- Option D (Maintaining the patient in a steep Trendelenburg position to improve venous return): The beach chair position often involves a reverse Trendelenburg (head up) to reduce blood loss, not a steep Trendelenburg.
- Option E (Securing the head in maximal extension to facilitate airway management): The head is typically secured in a neutral or slightly flexed position, often in a horseshoe headrest, to protect the cervical spine and prevent nerve injury, not maximal extension.
A 65-year-old male underwent open reduction and internal fixation (ORIF) of a two-part surgical neck fracture 3 weeks ago. He is now in the initial phase of his post-operative rehabilitation. Which of the following activities is most appropriate for him at this stage, according to the general principles of proximal humerus fracture rehabilitation?
Correct Answer: C
The case content, under 'Post-Operative Rehabilitation Protocols - Phase I Immobilization and Early Passive Motion,' states: 'Goals: Protect surgical repair, minimize pain and swelling, initiate early passive range of motion (PROM) to prevent stiffness... Exercises: Pendulum Exercises: Gentle, gravity-assisted swings... Initiated early, often within the first week... Passive Range of Motion (PROM): Forward Elevation (Flexion): Supine patient, therapist assists arm into flexion, staying below 90 degrees initially... Precautions: No active shoulder movement. No lifting, pushing, or pulling.'
- Option A (Active resistive strengthening exercises with light weights): This belongs to Phase III (Progressive Strengthening), much later in rehabilitation, after radiographic fracture union is confirmed.
- Option B (Full active range of motion (AROM) exercises, including overhead lifting): Full AROM and overhead lifting are typically not introduced until Phase II or III, and certainly not at 3 weeks post-op, as active movement and lifting are contraindicated in Phase I.
- Option D (Return to light recreational activities, such as golf or swimming): Return to light recreational activities is typically in Phase III, 4-6 months post-op, after full strength and range of motion are achieved.
- Option E (Manipulation Under Anesthesia (MUA) to address early stiffness): MUA is a surgical intervention for significant, persistent stiffness, usually considered much later (e.g., several months) if conservative therapy fails, not an early rehabilitation activity.
A 30-year-old male sustains a burst fracture of the atlas (Jefferson fracture) after a diving accident. On the open-mouth odontoid radiograph, the combined overhang of the C1 lateral masses on C2 is measured at 8 mm. What does this measurement indicate regarding the integrity of the stabilizing ligaments?
None
