ABOS Part I Orthopaedic Surgery Review: Humerus Fractures & Hand Infections | Part 22141

Key Takeaway
ABOS Part I Review modules offer advanced multiple-choice questions mirroring the American Board of Orthopaedic Surgery Part I and AAOS OITE examinations. This module focuses on high-yield clinical cases, including midshaft humerus fracture management, radial nerve palsy, and critical care for fight bite hand infections like septic arthritis and osteomyelitis, providing essential preparation for board certification.
ABOS Part I Orthopaedic Surgery Review: Humerus Fractures & Hand Infections | Part 22141
A 72-year-old female presents to the emergency department after a low-energy fall onto her outstretched arm, sustaining a closed, non-comminuted midshaft humerus fracture. She has no neurovascular deficits. Radiographs show a transverse fracture pattern with 15 degrees of varus angulation, 10 degrees of anterior angulation, and 1 cm of shortening. Based on the provided case material, what is the MOST appropriate initial management strategy for this patient?
Correct Answer: C
The case material explicitly states that for the vast majority of closed, non-comminuted midshaft humerus fractures, functional bracing remains a highly effective initial treatment, with union rates often exceeding 90%. The acceptable alignment criteria for non-operative treatment are less than 20 degrees of anterior angulation, less than 30 degrees of varus angulation, and less than 3 cm of shortening. This patient's fracture falls well within these acceptable parameters (15 degrees varus, 10 degrees anterior, 1 cm shortening). Her low-energy mechanism and lack of neurovascular deficit further support non-operative management.
Option A (Immediate ORIF with LCP via posterior approach) is incorrect. While ORIF is an option for certain indications, it is not the most appropriate initial management for a stable, closed fracture within acceptable alignment parameters, especially given the higher complication rates associated with operative management compared to non-operative care for suitable fractures.
Option B (Urgent intramedullary nailing) is incorrect for similar reasons. While IM nailing is a valid operative technique, it is not indicated as the primary treatment for this stable fracture. Furthermore, IM nailing can be associated with shoulder or elbow pain from entry portals.
Option D (Surgical exploration of the radial nerve) is incorrect. The patient has no neurovascular deficits. The case material clearly states that radial nerve palsy in closed humerus fractures should initially be observed, as spontaneous recovery occurs in 70-90% of cases. Immediate exploration is reserved for specific scenarios like open fractures with nerve deficits or evolving palsy with increasing soft tissue compromise, none of which apply here.
Option E (Admission for skeletal traction) is an outdated and generally not indicated primary treatment for midshaft humerus fractures in the modern era, especially for a stable, closed fracture amenable to functional bracing.
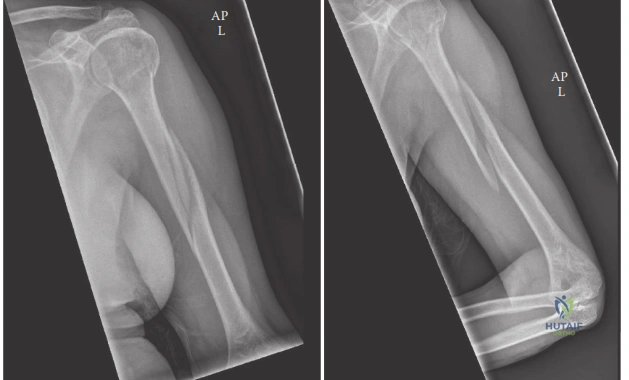
A 35-year-old male sustains a comminuted midshaft humerus fracture after a motor vehicle accident. He presents with a complete radial nerve palsy (wrist drop, finger drop, thumb abduction weakness, and dorsoradial hand sensory loss). Given the fracture pattern and the need for stable fixation, the surgeon plans an open reduction and internal fixation via a posterior approach. During the surgical dissection, as depicted in the image below, which of the following statements accurately describes the critical anatomical relationship of the radial nerve in the midshaft humerus?
Correct Answer: B
The case material explicitly states: "The most critical neurovascular structure in relation to the midshaft humerus is the radial nerve. It spirals obliquely from posterior to lateral across the midshaft humerus within the spiral (radial) groove, accompanied by the profunda brachii artery. Proximally, it lies between the medial and lateral heads of the triceps." The image provided, showing the posterior aspect of the humerus, visually reinforces this anatomical course, highlighting the nerve's vulnerability in this region and its relationship to the triceps muscle.
Option A (The radial nerve lies anterior to the brachialis muscle, accompanied by the brachial artery) is incorrect. The brachial artery and median nerve are typically found anteriorly, medial to the humerus, while the radial nerve is posterior and lateral in the midshaft. The radial nerve lies deep to the brachialis and brachioradialis in the distal third of the arm, not anterior to the brachialis in the midshaft.
Option C (The radial nerve is found in the deltopectoral interval, superficial to the pectoralis major) is incorrect. The deltopectoral interval is an anterior approach to the proximal humerus, and the radial nerve is not found there. The cephalic vein is typically found in this interval.
Option D (The radial nerve pierces the medial intermuscular septum to lie anterior to the medial epicondyle) is incorrect. The radial nerve pierces the lateral intermuscular septum to lie anterior to the lateral epicondyle. The ulnar nerve is the one that passes posterior to the medial epicondyle.
Option E (The radial nerve is typically located between the biceps brachii and brachialis muscles in the midshaft) is incorrect. The musculocutaneous nerve is found between the biceps and brachialis muscles. The radial nerve is posterior and lateral in the midshaft.
A 40-year-old male sustains a highly comminuted midshaft humerus fracture (AO/OTA 12-C3) after a fall from a height. He has no neurovascular deficits. The surgeon opts for operative fixation. Considering the biomechanical principles discussed in the case, which fixation strategy is generally preferred for this fracture pattern to promote secondary bone healing and why?
Correct Answer: D
The case material states that for comminuted fractures, "bridging principles to restore length and alignment without direct compression of fragments" are required. It also highlights that "Plate fixation offers superior resistance to bending and torsional forces, especially with longer plates and more screws (increasing working length). The principle of relative stability (bridging plates) is often employed for comminuted fractures." Furthermore, the summary mentions that "For comminuted midshaft fractures, MIPO plating techniques using LCPs are gaining popularity due to their potential to preserve soft tissue and provide stable fixation with relative stability principles." MIPO with an LCP applying relative stability (bridging) is ideal for comminuted fractures as it preserves periosteal blood supply and allows for secondary bone healing.
Option A (Dynamic compression plating (DCP) with interfragmentary lag screws for absolute stability) is incorrect. Absolute stability with lag screws and compression plating is typically used for simple transverse or short oblique fractures to achieve primary bone healing, not for highly comminuted fractures where direct compression would devitalize fragments and a bridging technique is preferred.
Option B (Intramedullary nailing with static locking, as it is a load-sharing device that resists bending and axial loads effectively) is a plausible option, as IM nailing is a load-sharing device promoting secondary healing. However, the question asks for the generally preferred strategy for a highly comminuted fracture, and the case specifically mentions MIPO plating for comminuted fractures. While nailing is effective for bending and axial loads, it is "less effective against rotational forces unless adequately locked proximally and distally." Plate fixation offers superior resistance to bending and torsional forces, making MIPO plating often preferred for highly comminuted patterns where precise alignment and rotational control are critical, especially when considering the potential for shoulder/elbow pain with nailing.
Option C (External fixation) is generally reserved for open fractures with severe soft tissue damage, highly contaminated wounds, or as a temporary measure in polytrauma, not typically as a definitive fixation for a closed comminuted midshaft humerus fracture.
Option E (Tension band wiring) is primarily used for avulsion fractures or fractures around joints (e.g., olecranon, patella) where muscle pull creates a tension force, converting it into compression. It is not suitable for stabilizing a highly comminuted midshaft humerus fracture.
A 60-year-old male with a history of morbid obesity and poorly controlled diabetes sustains a closed, segmental midshaft humerus fracture. He is non-compliant with medical advice and has a poor social support system. Initial attempts at functional bracing have failed to maintain acceptable alignment, with radiographs showing progressive varus angulation exceeding 35 degrees. Based on the case material, which of the following is the MOST compelling indication for operative management in this patient?
Correct Answer: E
The case material lists several factors that, individually or in combination, serve as strong indications for operative management:
- Failed non-operative treatment: "Persistent unacceptable alignment, nonunion, or patient intolerance of brace." This patient has progressive varus angulation exceeding 35 degrees, which is well beyond the acceptable 30 degrees.
- Segmental fractures: These are listed as a relative indication for operative intervention.
- Morbid obesity or non-compliant patients: "Where functional bracing is challenging." This patient fits both descriptions.
While poorly controlled diabetes (Option D) is a risk factor for nonunion, it is not listed as a direct indication for operative management itself, but rather a comorbidity that influences the decision-making process and prognosis. However, the combination of failed non-operative treatment, a segmental fracture, and patient factors (morbid obesity, non-compliance) makes operative management the most appropriate choice. Therefore, 'All of the above' (considering the individual factors as contributing to the overall decision) is the best answer.
Option A (The presence of a segmental fracture alone) is a relative indication, but not the sole compelling factor here.
Option B (The patient's morbid obesity and non-compliance) are relative indications, making bracing difficult, but not the only reasons for surgery.
Option C (The failure of non-operative treatment) is a strong indication, but combined with the other factors, the decision is even more robust.
Since all listed factors (A, B, C, and the underlying risk from D) contribute significantly to the decision for operative management, 'All of the above' is the most comprehensive and accurate answer.
A 28-year-old male presents with a closed midshaft humerus fracture after a direct blow. On initial examination, he has a complete radial nerve palsy. Radiographs show a simple transverse fracture with minimal displacement. The orthopedic surgeon decides to initially manage the fracture non-operatively with a functional brace. Three months later, there is no clinical or electrophysiological evidence of radial nerve recovery. Based on the case material, what is the MOST appropriate next step in managing the radial nerve palsy?
Correct Answer: A
The case material states: "The prevailing consensus...is that radial nerve palsy in closed humerus fractures should initially be observed. Spontaneous recovery occurs in 70-90% of cases within 3-6 months. Surgical exploration is indicated if there is no clinical or electrophysiological evidence of recovery after 3-6 months..." In this scenario, 3 months have passed with no clinical or electrophysiological recovery, placing the patient at the threshold for considering exploration. Given the lack of any recovery, immediate surgical exploration is the most appropriate next step to assess the nerve's condition (e.g., entrapment, partial laceration) and potentially perform nerve repair or grafting if indicated.
Option B (Continue observation for another 3 months) is incorrect. While recovery can sometimes extend beyond 6 months, the guideline specifically states exploration is indicated if no recovery is seen after 3-6 months. Waiting longer without any signs of recovery would delay potential intervention and worsen outcomes if the nerve is transected or entrapped.
Option C (Initiate tendon transfers) is incorrect as a primary next step. Tendon transfers are typically considered if recovery does not occur after 9-12 months, after nerve exploration and repair attempts have failed or are deemed not feasible.
Option D (Order a high-resolution MRI) is incorrect. While MRI can visualize nerve continuity, it is not the definitive diagnostic or therapeutic step when clinical and electrophysiological studies indicate no recovery. Surgical exploration remains the gold standard for direct assessment and potential repair.
Option E (Prescribe corticosteroids) is incorrect. Corticosteroids are not indicated for radial nerve palsy in this context and would not promote nerve regeneration or recovery from a mechanical injury.
A 55-year-old male presents with a midshaft humerus fracture following a high-energy trauma. On initial assessment, he has diminished radial pulses and an expanding hematoma in the arm. He also has a complete radial nerve palsy. Which of the following pre-operative imaging studies is MOST critical to obtain immediately for this patient?
Correct Answer: C
The case material explicitly states under Pre-Operative Planning: "Angiography: Indicated if vascular injury is suspected (e.g., diminished pulses, expanding hematoma)." This patient presents with both diminished radial pulses and an expanding hematoma, which are classic signs of a vascular injury requiring urgent assessment and potential repair. Vascular injury is an absolute indication for operative intervention, and its identification is paramount.
Option A (Standard AP and lateral radiographs) are essential for fracture characterization but will not provide information about the vascular status. While they are always obtained, they are not the *most critical* immediate study for the suspected vascular injury.
Option B (Computed Tomography (CT) scan) is useful for complex comminuted fractures or articular involvement but is not the primary study for acute vascular injury. A CT angiogram (CTA) could be an alternative to conventional angiography, but the question specifically asks about angiography, which is the gold standard for detailed vascular assessment.
Option D (Electromyography (EMG) and nerve conduction studies (NCS)) are used to assess nerve function and prognosis, typically 6-8 weeks after injury, not for acute assessment of vascular compromise. The radial nerve palsy, while present, is secondary to the immediate life-threatening vascular concern.
Option E (Magnetic Resonance Imaging (MRI) of the brachial plexus) is not indicated in the acute setting for a midshaft humerus fracture with suspected vascular injury. It might be considered for complex brachial plexus injuries, but not as the immediate critical study here.
A surgeon is planning an open reduction and internal fixation of a midshaft humerus fracture via a posterior approach (Henry triceps split). The patient is being positioned for surgery. Which of the following patient positions is MOST commonly used for this approach, and what is a key advantage of this position?
Correct Answer: B
The case material explicitly states under 'Patient Positioning': "**Lateral Decubitus Position:** Most commonly used for posterior plating approaches (Henry or triceps splitting). ...Advantages: Excellent access to the entire posterior and posterolateral aspects of the humerus, allowing for easy identification and protection of the radial nerve. Good visualization for direct reduction." This directly matches the description in Option B.
Option A (Supine position with the arm draped over an arm board) is primarily indicated for antegrade intramedullary nailing or anterior plating, not typically for a posterior approach. The advantage listed is for antegrade nailing, not posterior plating.
Option C (Beach chair position) is a variation of the supine position, primarily used for antegrade nailing or shoulder surgery, not for posterior midshaft humerus plating.
Option D (Prone position) can be used for posterior plating but is less common than lateral decubitus due to anesthetic challenges and increased patient risks. While it offers direct posterior access, the claim of 'minimal risk to the brachial plexus' is not a unique advantage over lateral decubitus, and prone positioning has its own set of risks.
Option E (Semi-Fowler position) is similar to the beach chair and is used for shoulder procedures or antegrade nailing, not typically for posterior midshaft humerus plating.
During a posterior approach (Henry triceps split) for open reduction and internal fixation of a midshaft humerus fracture, the surgeon has incised the skin and subcutaneous tissue and is proceeding with deep dissection. What is the MOST critical step to perform next to ensure patient safety and prevent iatrogenic injury?
Correct Answer: B
The case material emphasizes: "**Radial Nerve Protection:** This is the cardinal rule for midshaft humerus fracture surgery. Regardless of the approach, the radial nerve must be identified and protected." Under the 'Posterior Approach Henry Triceps Split' section, it states: "Deep Dissection & Internervous Plane: ...Crucially, identify the radial nerve. It typically lies within the spiral groove, deep to the lateral head of the triceps and medial to the lateral intermuscular septum. Trace the nerve proximally and distally, isolating it with vessel loops. Protect the profunda brachii artery accompanying the nerve. This step is critical and often performed first before further fracture exposure." Therefore, identifying the triceps interval and then the radial nerve is the most critical immediate next step.
Option A (Incise the deep fascia and immediately expose the fracture site) is incorrect because it bypasses the crucial step of radial nerve identification, significantly increasing the risk of iatrogenic injury.
Option C (Reflect the brachialis and biceps brachii muscles medially) describes a step in an anterolateral approach, not a posterior approach.
Option D (Perform a fasciotomy of the forearm) is not indicated unless there is clinical evidence of compartment syndrome, which is not mentioned in the vignette. It is not a routine step in midshaft humerus fracture fixation.
Option E (Apply a distractor to the fracture fragments) is a step in fracture reduction and fixation, which occurs after the nerve has been identified and protected, and the fracture site exposed. It is not the immediate next step after superficial dissection.
A 48-year-old male underwent open reduction and internal fixation with a locking compression plate for a comminuted midshaft humerus fracture 8 months ago. He continues to experience pain at the fracture site, and recent radiographs show no evidence of callus formation with persistent fracture lines. Clinically, there is motion at the fracture site. He is a smoker and has poorly controlled nutrition. What is the MOST appropriate management strategy for this established nonunion?
Correct Answer: C
The case material defines nonunion as "Failure of radiographic healing by 6-9 months post-fracture, often accompanied by pain or instability." This patient meets the criteria (8 months, pain, motion, no callus). The management section for nonunion states: "For established nonunions, revision surgery often involves combining mechanical stabilization (e.g., exchange nailing, conversion from plate to nail, or vice versa, dual plating) with biological augmentation (autogenous bone grafting). Addressing underlying risk factors (e.g., smoking cessation, nutritional optimization) is also crucial." Therefore, revision surgery with exchange nailing (a form of mechanical enhancement) and autogenous bone grafting (biological enhancement), along with addressing smoking and nutrition, is the most comprehensive and appropriate strategy.
Option A (Continue observation) is incorrect. At 8 months with no signs of healing and persistent pain/motion, it is an established nonunion, and further observation without intervention is unlikely to lead to union, especially with risk factors present.
Option B (Initiate bisphosphonates) is incorrect. Bisphosphonates are used for osteoporosis and to reduce fracture risk, not to stimulate healing of an established nonunion. They can even inhibit bone remodeling in some contexts.
Option D (Removal of the existing plate and application of a larger plate without bone grafting) is partially correct regarding mechanical enhancement but critically misses the biological component. For an established nonunion, especially with risk factors like smoking and poor nutrition, biological augmentation with bone grafting is almost always necessary to stimulate healing.
Option E (Aggressive physical therapy) is incorrect. Aggressive mobilization of an unstable nonunion will not promote healing and may exacerbate pain and instability. Activity should be restricted until definitive treatment for the nonunion is performed.
A 30-year-old male undergoes successful open reduction and internal fixation of a midshaft humerus fracture with a locking compression plate. The fixation is deemed stable intraoperatively. According to the post-operative rehabilitation protocols outlined in the case, what is the MOST appropriate initial approach to rehabilitation in the immediate post-operative phase (first 1-2 weeks)?
Correct Answer: C
The case material states under 'Immediate Post-Operative Phase': "**Immobilization:** Initially, a sling or shoulder immobilizer for comfort and protection, especially for the first 1-2 weeks. For highly stable fixation (e.g., well-locked plate, IM nail with good purchase), early gentle active-assisted and passive ROM can begin within days." It also specifies: "**Weight-Bearing:** No weight-bearing or lifting with the affected arm." This aligns perfectly with Option C.
Option A (Complete immobilization in a cast for 6 weeks) is incorrect. While immobilization is initially used, prolonged casting is generally avoided after stable operative fixation to prevent joint stiffness, especially in the humerus where early motion is encouraged.
Option B (Initiate immediate full active range of motion) is incorrect. While early motion is encouraged, 'full active ROM' immediately post-op is too aggressive and could jeopardize the healing fracture or fixation. It should be gentle and active-assisted/passive initially.
Option D (Aggressive isometric strengthening exercises) is incorrect. Isometric strengthening is introduced in the 'Early Healing and Strengthening Phase,' not immediately post-op. Aggressive exercises could disrupt the healing process.
Option E (Unrestricted active rotation) is incorrect. While early ROM is encouraged, 'unrestricted active rotation' is too aggressive, especially for the shoulder, and the case specifically advises: "*Caution is advised with rotation, especially in early IM nailing where rotational stability may be limited.*" Even with plate fixation, unrestricted active rotation is not typically allowed immediately.
A 22-year-old male sustains an open midshaft humerus fracture (Gustilo-Anderson Type II) with significant soft tissue contamination after a motorcycle accident. He has no neurovascular deficits. Based on the provided case material, which of the following is an absolute indication for operative management in this patient?
Correct Answer: B
The case material clearly lists "**Open fractures:** Require urgent debridement and stabilization to prevent infection" as an **absolute indication** for operative intervention. This patient has an open midshaft humerus fracture (Gustilo-Anderson Type II), which mandates immediate surgical management.
Option A (The patient's young age) is not an absolute indication for surgery. While it might influence the choice of fixation, it does not mandate surgery in itself.
Option C (The high-energy mechanism) often leads to more severe fractures, but it is not an absolute indication for surgery unless it results in specific complications (e.g., open fracture, vascular injury, severe comminution making non-op impossible).
Option D (The absence of neurovascular deficits) is a positive finding, but it does not, by itself, constitute an indication for surgery. In fact, for closed fractures, the absence of deficits often supports non-operative management.
Option E (The potential for a segmental fracture) is listed as a *relative* indication for surgery, not an absolute one. The definitive presence of an open fracture is a much stronger and absolute indication.
A 38-year-old male presents to the emergency department 10 hours after sustaining a laceration over the dorsum of his dominant right hand during an altercation. He admits to striking another individual in the mouth. On examination, a 1.5 cm transverse laceration is noted over the metacarpophalangeal (MCP) joint of the middle finger. There is moderate swelling, tenderness, and pain with passive flexion of the digit. Plain radiographs are obtained and show no fracture or foreign body. Given these findings, which of the following is the most appropriate next step in management?
Correct Answer: C
The patient's presentation (laceration over an MCP joint after striking a mouth, pain with passive flexion, swelling, and tenderness) is highly suspicious for a 'fight bite' with potential septic arthritis of the MCP joint. Even in the absence of a visible foreign body or fracture on X-ray, the mechanism and clinical signs strongly suggest joint capsule penetration and deep infection. Emergent surgical irrigation and debridement with joint exploration is the standard of care for suspected septic arthritis or deep space infection from a human bite. This allows for thorough debridement of devitalized tissue, removal of any missed foreign bodies, and copious irrigation of the joint space. Intravenous broad-spectrum antibiotics should be initiated promptly. Oral antibiotics alone (A) are insufficient for deep infections. Discharging the patient (A, B) without definitive surgical management is dangerous and can lead to rapid joint destruction. While joint aspiration (D) can confirm septic arthritis, it should not delay definitive surgical management once clinically suspected. Primary closure of the wound (E) is contraindicated in contaminated human bite wounds due to the high risk of trapping infection.
A 45-year-old male presents with a 3-day history of worsening pain, swelling, and redness over the dorsum of his hand following a fight. He has a small, punctate wound over the third MCP joint. X-rays show no fracture or foreign body. Examination reveals significant swelling, warmth, and exquisite pain with any passive movement of the third MCP joint. He also reports a fever of 38.8°C. Which of the following is the most appropriate empiric intravenous antibiotic regimen, assuming no known allergies?
Correct Answer: B
The patient's presentation is highly suggestive of septic arthritis of the MCP joint, a severe complication of a fight bite. Empiric intravenous antibiotics are crucial. Amoxicillin-clavulanate (Augmentin) is the first-line empiric antibiotic for human bite infections. It provides excellent broad-spectrum coverage against the characteristic polymicrobial flora of human bites, including common aerobes (Staphylococcus, Streptococcus) and anaerobes (Bacteroides, Fusobacterium, Peptostreptococcus), as well as the fastidious Gram-negative rod Eikenella corrodens. Ciprofloxacin and Rifampin (A) lack adequate anaerobic coverage. Doxycycline and Metronidazole (C) also have gaps in coverage for the typical fight bite pathogens. Cephalexin (D) has good Gram-positive coverage but lacks activity against anaerobes and Eikenella. Vancomycin and Gentamicin (E) are typically reserved for more severe, resistant, or nosocomial infections, with Vancomycin targeting MRSA and Gentamicin providing Gram-negative coverage, but this combination is not optimal for initial empiric human bite coverage.
During surgical exploration of a 'fight bite' over the fifth MCP joint, purulent material is found tracking along the extensor digitorum communis tendon into the wrist. This finding is most indicative of which specific complication?
Correct Answer: C
Purulent material tracking along a tendon, especially into the wrist, is a classic sign of tenosynovitis, which is an infection of the tendon sheath. The extensor digitorum communis tendon is involved here. While other pathologies like septic arthritis (B) and osteomyelitis (D) can coexist or develop from tenosynovitis, the direct observation of pus within the tendon sheath extending proximally confirms tenosynovitis. Cellulitis (A) is a superficial soft tissue infection. A localized abscess (E) would be a circumscribed collection of pus, but its extension along a tendon sheath points specifically to tenosynovitis.
A patient is undergoing surgical exploration for a fight bite over the third MCP joint. To best expose potential joint capsule violation and aid in thorough debridement and irrigation, what position should the finger be held in during the initial assessment?
Correct Answer: D
For a suspected 'fight bite' over an MCP joint, the finger should be held in full flexion (the clenched fist position) during initial assessment and irrigation. The injury typically occurs with the hand clenched in a fist, which causes the skin and extensor tendon to shift proximally relative to the MCP joint capsule. When the hand is then extended, the damaged joint capsule and any penetrating wound tract move distally and are no longer aligned with the initial skin laceration, effectively sealing off the wound and potentially trapping bacteria within the joint. Flexing the finger realigns the entry portal, allowing for thorough irrigation and exploration of the joint capsule. Full extension (A) or neutral (B) will obscure the primary injury tract and make it difficult to assess the joint capsule. Hyperextension (C) is anatomically incorrect for this purpose.
Following surgical debridement and intravenous antibiotics for a septic MCP joint secondary to a fight bite, which of the following splinting positions is most appropriate for initial immobilization?
Correct Answer: B
The 'intrinsic plus' or 'safe position' splint is generally recommended for hand immobilization following injury or surgery, especially for infections, to prevent joint contractures. This position involves placing the wrist in 20-30 degrees of extension, the MCP joints in approximately 70-90 degrees of flexion, and the IP joints in full extension. This position maintains the collateral ligaments of the MCP joints in their elongated state, preventing shortening contractures, and avoids shortening of the IP collateral ligaments. Full extension of MCPs (A, C) can lead to MCP collateral ligament shortening. Full flexion of IP joints (A, D) can lead to IP collateral ligament shortening. Active range of motion (E) is generally not indicated initially for a severe infection requiring immobilization.
A 22-year-old male presents with a persistent discharging sinus tract over the third metacarpal following a poorly managed fight bite 6 weeks ago. Plain radiographs reveal cortical irregularity and lucency of the metacarpal head. What is the most likely diagnosis?
Correct Answer: C
A persistent discharging sinus tract, especially following a human bite with radiographic evidence of cortical irregularity and lucency of the bone, is highly suggestive of chronic osteomyelitis. The fight bite can directly inoculate bacteria into the bone or lead to septic arthritis which then spreads to the bone. Chronic tenosynovitis (A) would primarily involve the tendon sheath and typically not present with bone changes. Septic non-union (B) would be if there was a fracture that failed to heal and became infected, but the question describes bone changes not specifically related to a fracture non-union. Reactive arthritis (D) is a sterile inflammatory arthritis following infection elsewhere. Chronic cellulitis (E) is a soft tissue infection that typically would not present with bone changes or a persistent sinus tract for this duration.
A 60-year-old diabetic patient presents with a fight bite over the fifth MCP joint, 24 hours after injury. Clinically, there is significant erythema, swelling, and purulent discharge. He has a history of penicillin allergy (anaphylaxis). Which intravenous antibiotic combination is most appropriate for initial empiric coverage?
Correct Answer: C
Given the patient's history of penicillin allergy (anaphylaxis), beta-lactam antibiotics like Ampicillin-sulbactam (A) and Piperacillin-tazobactam (D) are contraindicated. Cefazolin (B) is a first-generation cephalosporin, which has some cross-reactivity risk with penicillin, and when combined with Metronidazole, lacks full Gram-negative coverage for organisms like Eikenella. Clindamycin provides good coverage against anaerobes and Gram-positives (Staph/Strep). Ciprofloxacin provides good coverage against Gram-negatives, including Eikenella corrodens. This combination (Clindamycin and Ciprofloxacin) is a suitable and commonly used alternative for a penicillin-allergic patient with a severe human bite infection. Vancomycin (E) would cover MRSA and Gram-positives, and Aztreonam covers Gram-negatives including Eikenella, but this combination is often reserved for resistant organisms or specific scenarios. Clindamycin and Ciprofloxacin is a common and effective alternative.
A 25-year-old male presents with a painful, swollen, and red index finger following a fight bite 36 hours ago. The wound is over the MCP joint. During surgical exploration, the extensor digitorum communis tendon is found to be partially lacerated. What is the most appropriate management for the partially lacerated tendon in this acutely infected field?
Correct Answer: B
In an acutely infected wound, primary repair of a partially or completely lacerated tendon is generally contraindicated due to the high risk of infection of the repair site, leading to tendon necrosis, rupture, and adhesion formation. The most appropriate management is thorough irrigation and debridement of the tendon ends and surrounding tissue, followed by leaving the tendon unrepaired. Definitive repair, if necessary, should be delayed until the infection is completely resolved and the wound is clean. Excising the tendon (C) would result in significant functional deficit. Covering with a flap (D) is premature and risky in an infected field. Corticosteroids (E) are contraindicated in active infection.
What is the primary differentiating feature between cellulitis and a deep-seated infection (e.g., septic arthritis) in a hand with a fight bite?
Correct Answer: C
While redness and warmth (A), elevated WBC count (B), and duration of symptoms (E) can be present in both cellulitis and deep infections, significant pain with passive range of motion (PROM) of the affected joint, especially if disproportionate to superficial findings, is the hallmark sign differentiating a deep-seated joint infection (septic arthritis) from isolated cellulitis. Cellulitis primarily involves the superficial soft tissues, while septic arthritis directly affects the joint capsule, making any movement excruciating due to stretching of the inflamed synovium. The size of the laceration (D) is not a reliable differentiator for depth of infection.
A patient presents with a fight bite over the fifth MCP joint. The x-ray shows a fracture of the fifth metacarpal neck (Boxer's fracture). What implications does this fracture have on managing the bite wound?
Correct Answer: C
A fracture of the fifth metacarpal neck associated with a fight bite means the fracture is an open fracture (communicating with the outside environment through the bite wound). This significantly complicates management. The bite wound requires meticulous debridement and copious irrigation, and the fracture must be treated as an open, contaminated injury. Definitive fracture stabilization (e.g., with internal hardware) is often delayed until the infection is controlled and the wound is clean, or performed with external fixation if immediate stability is required and internal fixation is deemed too risky in the acute infected setting. Primary closure of the bite wound (A) is contraindicated. Immediate definitive internal fixation (B) is dangerous in an infected field due to high risk of hardware infection. A fracture does not negate infection risk (D); in fact, it increases the risk of osteomyelitis. Ignoring the fracture (E) is malpractice.
On initial presentation, she has a completely normal neurovascular examination. Following a closed reduction and splinting attempt in the emergency department, she suddenly loses active wrist and thumb extension. What is the most appropriate next step in management?
To safely protect the radial nerve during this exposure, the surgeon must understand its anatomical course. At what approximate distance proximal to the lateral epicondyle does the radial nerve typically pierce the lateral intermuscular septum?
During an extensile posterior approach to the humerus for fracture fixation, identifying and protecting the radial nerve is critical. Based on standard anatomical landmarks, where does the radial nerve predictably cross the posterior aspect of the humerus before piercing the lateral intermuscular septum?
None
