Comprehensive Introduction and Patho-Epidemiology
The human hand is an intricate biomechanical marvel, relying on a delicate equilibrium between the skeletal architecture, capsuloligamentous constraints, and the dynamic forces of the extrinsic and intrinsic musculature. Fractures and dislocations of the hand are among the most common injuries evaluated by orthopedic surgeons, accounting for nearly 20% of all emergency department fracture presentations. The majority of these injuries involve the metacarpals and phalanges, with the distal phalanx being the most frequently fractured bone, followed closely by the metacarpals and the proximal phalanges. Epidemiologically, these injuries exhibit a bimodal distribution, predominantly affecting young males engaged in athletic, occupational, or violent altercations, and older individuals sustaining low-energy falls. The socioeconomic impact of hand trauma is profound, often resulting in significant lost wages, prolonged rehabilitation, and permanent functional impairment if inadequately managed.
For the majority of nondisplaced or minimally displaced metacarpal and phalangeal fractures, closed manipulation, proper splinting in the "intrinsic-plus" (safe) position, and protected early motion generally produce excellent functional results. The intrinsic-plus position—characterized by metacarpophalangeal (MCP) joint flexion of 70 to 90 degrees and interphalangeal (IP) joint extension—maintains the collateral ligaments at their maximal length, thereby mitigating the risk of devastating joint contractures. However, the threshold for operative intervention is rapidly crossed when fracture geometry dictates instability, or when the capsuloligamentous envelope is severely compromised. Operative treatment, encompassing open reduction and internal fixation (ORIF) or closed reduction with percutaneous pinning (CRPP), is mandated to provide superior outcomes in specific, high-risk clinical scenarios.
The overarching goal of any surgical intervention in hand trauma is the precise restoration of anatomical alignment, the preservation of the gliding planes of the flexor and extensor tendons, and the rapid reinstitution of motion to prevent stiffness. The patho-epidemiology of hand fractures dictates that the soft tissue envelope is often the primary determinant of the final functional outcome. Because the tendons, neurovascular bundles, and skeletal structures are housed within tight, unforgiving compartments with minimal subcutaneous fat, any excessive edema, hematoma, or iatrogenic trauma can lead to profound fibrosis and tendon adhesions. Therefore, the contemporary approach to hand trauma emphasizes not only the mechanical stabilization of the fracture but also the meticulous, atraumatic handling of the surrounding soft tissues to optimize the biological environment for healing.
Understanding the mechanism of injury is paramount in anticipating the fracture pattern and associated soft tissue damage. Axial loading injuries typically produce intra-articular split or impaction fractures, such as pilon fractures of the middle phalanx base, which are notoriously difficult to manage. Torsional forces result in spiral or long oblique fractures that are inherently unstable and prone to shortening and rotational deformity. Direct crush injuries often yield highly comminuted, transverse, or short oblique patterns with significant soft tissue compromise, necessitating a more cautious approach to surgical timing and implant selection. By synthesizing the epidemiological data with an understanding of the patho-mechanical forces at play, the orthopedic surgeon can formulate a rational, individualized treatment algorithm for each patient.
Detailed Surgical Anatomy and Biomechanics
The skeletal architecture of the hand is organized into dynamic longitudinal and transverse arches that facilitate prehension, power grip, and fine motor dexterity. The proximal transverse arch is rigid, formed by the distal carpal row and the rigid intermetacarpal ligaments of the second and third carpometacarpal (CMC) joints. In contrast, the distal transverse arch, at the level of the metacarpal heads, is highly mobile due to the laxity of the fourth and fifth CMC joints. This mobility allows the ulnar border of the hand to cup around objects. The longitudinal arches are formed by the individual digital rays. Fractures that disrupt these arches, particularly those causing loss of metacarpal length or alteration of the normal digital cascade, severely compromise grip strength and hand function. The intrinsic musculature (interossei and lumbricals) and extrinsic tendons exert predictable deforming forces on fractured segments. For instance, in metacarpal neck fractures, the volar-directed force of the intrinsic muscles combined with the proximal pull of the extrinsic flexors consistently produces apex-dorsal angulation.
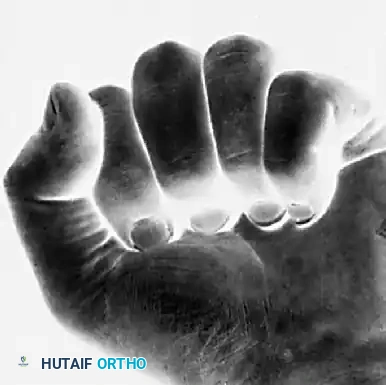
One of the most devastating complications of hand fractures is unrecognized malrotation. Because of the functional length of the digits, even a seemingly trivial rotational deformity of 5 degrees at the metacarpal level can translate to 1.5 cm of digital overlap at the fingertips, severely impairing the patient's ability to form a functional grip. Clinical assessment of rotation must be performed meticulously. The most reliable method is observing the digital cascade during active or passive flexion. Normally, when a fist is made, the longitudinal axes of all the fingers converge and point toward the region of the scaphoid tubercle.

Normally, all fingers point toward the region of the scaphoid when a fist is made.
Malrotation at the fracture site disrupts this harmonious convergence, causing the affected finger to deviate and cross over adjacent digits. This overlap must be corrected anatomically during reduction.

Malrotation at the fracture causes the affected finger to deviate, leading to functional impairment during grip.
Fingernail Alignment and the Assessment of Rotation
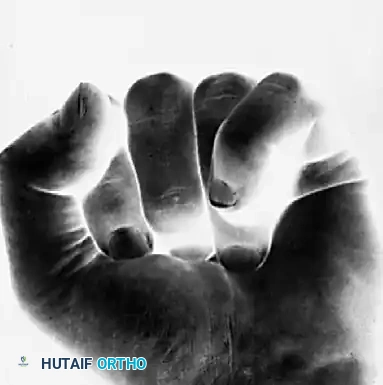
Another highly effective clinical tool for detecting subtle malrotation is observing the plane of the fingernails in a semi-flexed position and comparing it to the contralateral, uninjured hand. Normal alignment of the fingernails demonstrates a smooth, parallel arc that follows the contour of the distal transverse arch.

Normal alignment of the fingernails, demonstrating a smooth, parallel arc.
If a fracture is malrotated, the fingernail of the involved digit will sit out of plane compared to its neighbors. This is particularly noticeable in spiral fractures of the proximal phalanx or metacarpal shafts, where the deforming forces of the interosseous muscles exacerbate the rotational malalignment.

Alignment of the fingernails demonstrating clear malrotation of the ring finger.
Nuances of the Little Finger Kinematics
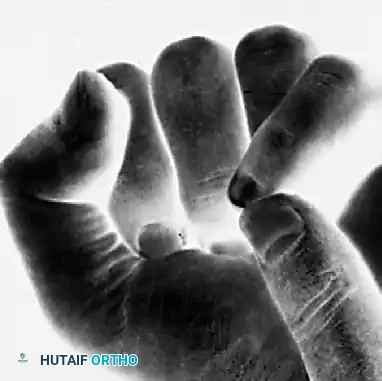
The fifth ray (little finger) possesses unique kinematics due to the mobility of the fifth carpometacarpal (CMC) joint, which allows for 20 to 30 degrees of flexion and extension. This mobility can sometimes mask or simulate rotational deformities, requiring careful examination.
Note the alignment of the normal little finger during flexion.
Because of the CMC joint's mobility, a normal little finger can actually be made to overlap the ring finger passively. With incomplete flexion, this normal overlap may be erroneously perceived as a rotational deformity.
A normal little finger can be made to overlap the ring finger. With incomplete flexion, this overlap may be perceived as a rotational deformity.
Furthermore, rotation of the little finger at the CMC joint can be accentuated by passive manipulation by the examiner. The examiner must be acutely aware of this hypermobility to avoid misdiagnosing a normal variant as a pathologic malrotation.
Rotation of the little finger at the carpometacarpal joint may be accentuated by passive help.
However, it is critical to note that from a position of normal alignment, true external rotation of the little finger is biomechanically impossible without a structural disruption (fracture or ligamentous tear). The ulnar collateral ligament and the dorsal capsular structures of the CMC and MCP joints strictly prohibit this motion in the uninjured state.

From the normal alignment of the little finger, external rotation is impossible.
Finally, the examiner must ensure that all digits are fully flexed during assessment. Incomplete flexion of the ring finger may simulate a rotational deformity because it naturally tends to overlap the little finger as it descends into the palm.
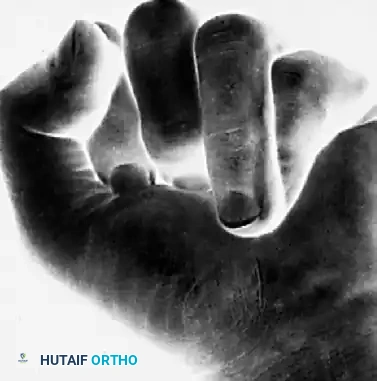
Incomplete flexion of the ring finger may simulate a rotational deformity because it tends to overlap the little finger.
Exhaustive Indications and Contraindications
The decision to proceed with operative fixation of hand fractures requires a nuanced understanding of fracture stability, patient demands, and the inherent risks of surgical intervention. While each case must be individualized, some form of rigid or semi-rigid fixation is most often indicated for fractures that cannot be reduced or maintained in an acceptable alignment via closed means. Irreducible fractures are an absolute indication for surgery. These typically occur when soft tissue interposition blocks reduction; a classic example is a complex metacarpophalangeal dislocation where the volar plate becomes incarcerated within the joint space, or a proximal phalanx fracture where the lateral bands or flexor tendons become entrapped in the fracture site.
Unstable fracture patterns also mandate operative stabilization. Spiral or long oblique fractures of the metacarpals or phalanges are notoriously unstable. Despite appropriate splinting, the dynamic forces of the extrinsic flexors and extensors will inevitably cause these fractures to shorten and rotate. Shortening of a metacarpal by more than 3 to 5 mm alters the tension of the intrinsic muscles, leading to an intrinsic-minus posture and significant grip weakness. Intra-articular fractures are another critical indication. Fractures involving more than 25% of the articular surface or those with greater than 1 mm of articular step-off predispose the joint to rapid post-traumatic arthritis and severe stiffness. Anatomic reduction and rigid fixation are required to restore the congruity of the joint surface and allow for immediate postoperative motion.
Multiple fractures, often resulting from "crush" injuries, represent a scenario where the hand loses its structural scaffolding. In these cases, internal fixation of multiple rays is necessary to restore the skeletal framework, allowing the soft tissues to heal at their optimal resting length. Open fractures requiring surgical debridement often benefit from immediate stabilization. Rigid fixation protects the delicate soft tissue repairs, prevents ongoing trauma to the neurovascular structures from mobile bone fragments, and facilitates wound care. Finally, fractures with segmental bone loss require structural grafting and rigid plate or K-wire fixation to span the defect and maintain length until biologic incorporation occurs.
Contraindications to operative intervention, while fewer, are equally important to recognize. Severe medical comorbidities that preclude safe anesthesia administration are an absolute contraindication. Relative contraindications include highly contaminated wounds presenting in a delayed fashion; in such cases, immediate internal fixation with plates and screws is ill-advised due to the prohibitive risk of deep infection. Instead, these should be managed with serial debridements and temporary stabilization using external fixation or judiciously placed K-wires. Non-compliant patients or those with severe cognitive impairments may also be poor candidates for complex open reduction and internal fixation, as they may be unable to adhere to the rigorous postoperative rehabilitation protocols necessary to prevent hardware failure and joint contractures.
| Parameter | Indications for Operative Fixation | Contraindications to Operative Fixation |
|---|---|---|
| Fracture Pattern | Irreducible fractures (soft tissue interposition); Unstable spiral/oblique patterns; Intra-articular step-off > 1mm or >25% surface involvement. | Nondisplaced or stable transverse fractures that maintain alignment in an intrinsic-plus cast. |
| Soft Tissue Status | Open fractures requiring stabilization to protect repairs; Compartment syndrome requiring fasciotomy. | Active, untreated localized infection; Grossly contaminated wounds (relative contraindication for plates/screws). |
| Systemic Factors | Polytrauma patients requiring immediate mobilization of the upper extremity for transfers. | Severe medical comorbidities precluding anesthesia; Extreme non-compliance or inability to participate in hand therapy. |
| Anatomic Factors | Multiple ray involvement (crush injuries); Segmental bone loss requiring grafting. | Fractures in severely osteoporotic bone where hardware purchase is impossible (relative - may require specialized techniques). |
Pre-Operative Planning, Templating, and Patient Positioning
Accurate radiographic assessment is the cornerstone of preoperative planning in hand trauma. Standard posteroanterior (PA), true lateral, and oblique radiographs of the hand are mandatory. However, the complex overlapping anatomy of the hand often requires specialized views to fully delineate the fracture geometry. Shaft fractures are best evaluated by multiple images with the bone parallel to the film or image source. To avoid overlap on lateral views, a 10-degree supinated lateral is ideal for the index and middle fingers, while a 10-degree pronated lateral isolates the ring and small fingers. Articular fractures involving the interphalangeal or metacarpophalangeal joints may require specific views projecting the joint surfaces perpendicular to the radiation beam. The Brewerton view, obtained with the MCP joints flexed to 65 degrees and the tube angled 15 degrees ulnar-to-radial, is invaluable for diagnosing occult metacarpal head fractures and collateral ligament avulsions.
Advanced imaging modalities, such as Computed Tomography (CT) scans in the sagittal, coronal, and axial planes, are occasionally necessary to evaluate displacement, especially when a splint or cast obscures fine details. CT with 3D reconstruction is critical for the preoperative planning of complex intra-articular fractures, such as Rolando fractures of the thumb base or pilon-type fractures of the middle phalanx. These scans allow the surgeon to map the articular fragments, plan the trajectory of lag screws, and determine the optimal placement of minicondylar plates. Templating should be performed routinely. The surgeon must measure the size of the bone fragments and select the appropriate implant systems (e.g., 1.2 mm vs. 1.5 mm vs. 2.0 mm screws) before entering the operating room. Anticipating the need for bone graft (autograft from the distal radius or allograft) is also a crucial component of the preoperative plan.
The timing of fracture fixation is a critical variable in the surgical decision-making process. Percutaneous pinning should ideally be attempted before the onset of massive edema obliterates external anatomic landmarks. If the soft tissue envelope is already compromised by severe swelling, the extremity should be strictly elevated for 24 to 48 hours before attempting reduction and pinning. Fracture fixation, particularly via open approaches, is preferably performed when the soft tissue envelope is pliable and not markedly swollen. Operating through severely traumatized, edematous tissue increases the risk of wound dehiscence, infection, and subsequent tendon adhesions. In cases of severe closed trauma, a deliberate delay in fixation of 7 to 10 days is often warranted to allow the soft tissues to declare themselves and swelling to subside.
Patient positioning and operating room setup must be optimized for efficiency and precision. The patient is typically positioned supine with the operative arm extended on a radiolucent hand table. A pneumatic tourniquet is applied to the upper arm, and the extremity is exsanguinated using an Esmarch bandage prior to inflation (typically to 250 mmHg). For highly comminuted fractures where prolonged operative time is anticipated, a sterile forearm tourniquet may be considered to minimize ischemic pain, though upper arm placement remains standard. Intraoperative fluoroscopy is essential, even when a fracture is being reduced under direct vision. The mini C-arm should be positioned parallel to the hand table, allowing the surgeon to control the imaging independently. Radiographs can prevent subtle errors in alignment and can reveal small, incarcerated fragments of bone or articular step-offs not appreciated before reduction.
Step-by-Step Surgical Approach and Fixation Technique
When operative intervention is selected, the surgeon must choose the fixation method that provides adequate stability while minimizing soft tissue trauma. The management of open fractures and dislocations takes precedence, requiring urgent evaluation and treatment to prevent deep space infections, osteomyelitis, and devastating stiffness. The principles of the Gustilo-Anderson classification apply, though the robust vascularity of the hand often allows for more aggressive salvage than in the lower extremity. The primary tenet of open fracture management is meticulous surgical débridement. Thorough irrigation with normal saline and the sharp excision of all devitalized soft tissue, skin margins, and contaminated bone fragments are usually adequate for primary fracture treatment. The routine use of prophylactic antibiotics for fresh, clean, simple open injuries of the hand is debated, but antibiotic use is absolutely justified when prolonged contamination has occurred, essential tissues have borderline viability, or the injury involves a human or animal bite (requiring coverage for Eikenella corrodens or Pasteurella multocida, typically with Amoxicillin-Clavulanate or IV cephalosporins).
Percutaneous Pinning (K-wires)
Kirschner wire (K-wire) fixation remains the workhorse for many hand fractures, particularly extra-articular phalangeal and metacarpal neck fractures. Biomechanically, K-wires provide relative stability; they do not compress the fracture but hold it in alignment while secondary bone healing via callus formation occurs. The technique involves closed reduction of the fracture using longitudinal traction and manipulation, followed by the percutaneous insertion of smooth K-wires (typically 0.035 or 0.045 inches) under fluoroscopic guidance. Pins can be placed in a crossed configuration or longitudinally. When crossing pins, it is imperative that they do not cross exactly at the fracture site, as this can distract the fragments and lead to nonunion. To prevent thermal necrosis of the bone, pins should be inserted using a power driver at low speeds. Pins are typically bent, cut, and left protruding through the skin to facilitate easy removal in the clinic at 3 to 4 weeks, provided rigid clinical union is progressing.
Minicondylar Plate Fixation
For complex periarticular fractures, such as those involving the metacarpal head or the base of the proximal phalanx, minicondylar plates offer rigid fixation. These implants are indicated for comminuted intra-articular fractures where K-wires would not provide sufficient stability to allow for early motion. A dorsal surgical approach is typically utilized. The extensor mechanism must be carefully managed; depending on the fracture geometry, the extensor tendon can be split longitudinally (tendon-splitting approach) or retracted laterally. The fracture is anatomically reduced and provisionally held with fine K-wires. The minicondylar plate is then contoured to match the specific anatomy of the bone and secured with locking or non-locking screws. The primary advantage of plate osteosynthesis is that it allows for absolute stability and immediate postoperative active range of motion, which is critical for preventing joint contractures and tendon adhesions in these complex periarticular injuries.
Intraosseous Wiring and Lag Screw Techniques
Intraosseous wiring (e.g., 90-90 wiring or tension band wiring) is highly effective for transverse or short oblique fractures of the phalanges. This technique utilizes a combination of a longitudinal K-wire to control bending forces and an intraosseous stainless-steel wire loop to provide dynamic compression and control rotation. The advantage of this technique is its extremely low profile, which minimizes irritation to the overlying extensor gliding mechanism. For long oblique and spiral fractures, where the fracture length is at least twice the diameter of the bone, interfragmentary lag screw fixation is the gold standard. Using a standard glide hole and thread hole technique, 1.5 mm or 2.0 mm cortical screws are placed perpendicular to the fracture plane to achieve absolute stability through interfragmentary compression. This technique demands meticulous surgical execution, as over-tightening can easily split the delicate cortical bone of the phalanges.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical care and rigorous preoperative planning, complications following the operative treatment of hand fractures can and do arise. These complications are often directly related to the severity of the initial trauma, the degree of soft tissue stripping during surgical exposure, or patient non-compliance with postoperative rehabilitation protocols. The hand surgeon must be adept not only at primarily fixing these fractures but also at recognizing and managing the inevitable sequelae of severe hand trauma.
Malunion occurs when a fracture heals in a non-anatomic position. As previously discussed, rotational malunion is the most poorly tolerated deformity in the hand, leading to digital crossover and a profoundly weakened grip. The incidence of clinically significant malunion in operatively treated hand fractures ranges from 2% to 5%, though subtle radiographic malunions are more common. Angular malunions, such as apex dorsal angulation in metacarpal neck fractures, are better tolerated biomechanically due to the compensatory mobility of the adjacent joints. However, excessive angulation can lead to pseudo-clawing of the digit, a prominent metacarpal head in the palm that causes pain during grip, and an extension lag at the proximal interphalangeal (PIP) joint. Treatment for symptomatic malunions requires corrective osteotomies (closing wedge, opening wedge, or rotational osteotomies) at the site of the original fracture or at the metacarpal base, followed by rigid plate fixation.
Nonunion in the hand is relatively rare, with an incidence of less than 1% in closed fractures, primarily due to the excellent vascular supply of the upper extremity. However, the incidence rises significantly in the setting of severe open fractures with bone loss, deep infection, or inadequate immobilization (e.g., loose K-wires that fail to neutralize bending forces). Nonunions typically present with persistent pain, swelling, and motion at the fracture site beyond 8 to 12 weeks post-injury. Treatment requires a thorough debridement of the nonunion site to bleeding bone, rigid internal fixation (usually with a compression plate), and the application of autologous bone grafting, often harvested from the distal radius metaphysis or the iliac crest.
Joint contracture is by far the most common complication following hand fractures, affecting up to 20% of patients with complex intra-articular injuries. It is primarily caused by prolonged immobilization, persistent edema, and the formation of dense adhesions between the flexor or extensor tendons and the underlying fracture callus. The best treatment for contracture is meticulous prevention through anatomic fixation and early motion. If severe contractures develop and non-operative therapy (including static progressive splinting) has plateaued for at least 3 to 6 months, surgical intervention may be required. Salvage procedures include open capsulectomy, collateral ligament release, and tenolysis. In cases of severe, painful post-traumatic arthritis resulting from intra-articular fractures, salvage options are limited to joint arthrodesis (fusion) or, in select low-demand patients, arthroplasty.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Treatment |
|---|---|---|---|
| Joint Contracture | 10% - 20% | Prolonged immobilization, severe edema, tendon adhesions, intra-articular trauma. | Aggressive hand therapy, static progressive splinting; Surgical tenolysis or capsulectomy if plateaued > 6 months. |
| Malunion | 2% - 5% | Inadequate reduction, loss of fixation, unrecognized rotational deformity. | Corrective osteotomy (rotational or angular) with rigid internal plate fixation. |
| Infection (Deep) | 1% - 3% | Open fractures, prolonged surgical time, severe soft tissue compromise. | Urgent irrigation and debridement, hardware removal if unstable, culture-directed IV antibiotics. |
| Nonunion | < 1% (Closed) up to 5% (Open) |
Bone loss, inadequate stabilization, thermal necrosis from K-wires, infection. | Debridement of nonunion site, rigid plate osteosynthesis, autologous bone grafting. |
| Hardware Failure | 2% - 4% | Patient non-compliance, undersized implants, early unprotected weight-bearing. | Revision open reduction and internal fixation, potentially upgrading to a stronger construct (e.g., locking plates). |
Phased Post-Operative Rehabilitation Protocols
The success of operative intervention in hand trauma is inextricably linked to the quality and execution of the postoperative rehabilitation protocol. The hand surgeon and the certified hand therapist (CHT) must work in close collaboration to navigate the delicate balance between protecting the healing fracture and preventing soft tissue adhesions. The rehabilitation process is generally divided into three distinct phases, tailored to the specific fracture pattern, the rigidity of the fixation achieved, and the patient's individual healing response.
Phase 1 encompasses the immediate postoperative period, typically lasting from day 1 to day 10. The primary goals during this phase are the control of edema, the management of pain, and the protection of the surgical construct. The hand is immobilized in a bulky, non-compressive dressing, reinforced with a plaster or fiberglass splint. Crucially, the splint must place the hand in the "intrinsic-plus" position—wrist extended 20 to 30 degrees, MCP joints flexed 70 to 90 degrees, and IP joints fully extended. This position maintains the collateral ligaments of the MCP joints at their maximum length, preventing extension contractures, while preventing flexion contractures at the PIP joints. Strict elevation of the extremity above the level of the heart is mandatory to facilitate venous and lymphatic drainage. Active motion of the uninvolved digits, shoulder, and elbow is encouraged immediately to prevent regional stiffness.
Phase 2 begins once the surgical wounds have stabilized and the initial inflammatory phase has subsided, typically between days 10 and 21. If rigid internal fixation (e.g., lag screws or plates) was achieved, early protected active range of motion (AROM) is initiated. The bulky dressing is removed, and a custom-molded thermoplastic splint is fabricated, which the patient removes only for designated exercise sessions. Therapy focuses on tendon gliding exercises, including isolated flexor digitorum profundus (FDP) and flexor digitorum superficialis (FDS) glides, to prevent adhesions at the fracture site. If the fracture was treated with percutaneous pinning, motion may be delayed until the pins are removed at 3 to 4 weeks, depending on the stability of the construct. Synergistic wrist and finger motion is emphasized to maximize tendon excursion while minimizing stress on the fracture site.
Phase 3 marks the transition to strengthening and the return to functional activities, typically commencing around 6 to 8 weeks postoperatively, contingent upon radiographic evidence of bony union. Passive range of motion (PROM) and dynamic or static progressive splinting may be introduced at this stage to address any residual joint contractures. Strengthening exercises begin with light putty and progress to grip and pinch strengthening using specialized dynamometers. The patient is gradually weaned from the protective splint and guided through work-hardening or sports-specific drills. It is critical to educate the patient that maximal functional recovery following a complex hand fracture may take up to a full year, and adherence to the home exercise program during this final phase is paramount to achieving an optimal outcome.
Summary of Landmark Literature and Clinical Guidelines
The evolution of operative treatment for hand fractures is deeply rooted in landmark anatomical and clinical studies that have shaped modern orthopedic practice. The foundational work by Swanson in the 1970s
