Comprehensive Introduction and Patho-Epidemiology
Although the general principles of orthopedic trauma management remain consistent across all regions of the musculoskeletal system, the hand represents a highly specialized, prehensile structure that interacts intimately with the environment. Consequently, it is exquisitely sensitive to functional impairment. The intricate balance of the intrinsic and extrinsic musculature, combined with the tight tolerances of the flexor and extensor gliding mechanisms, dictates that even minor architectural disruptions can lead to profound disability. The hand is not merely a mechanical appendage; it is a primary organ of sensory feedback and environmental manipulation, making the preservation of its function the paramount objective in trauma management.
In the treatment of hand fractures and dislocations, a critical paradigm must be understood by all orthopedic surgeons: anatomical and radiographic perfection does not always equate to normal function. The pursuit of a pristine radiographic appearance through extensive surgical dissection often results in severe soft tissue scarring, tendon adhesions, and irreversible joint contractures. Often, it is far superior to accept a less-than-anatomical position of a fracture—provided it falls within acceptable biomechanical tolerances—and strive for excellent functional recovery through proper splinting and early, aggressive mobilization. The ultimate goal of hand fracture management is the restoration of the hand as a functional unit. When operative intervention is required, the surgeon must select the least complicated procedure that provides sufficient stability to allow for early active motion.
Epidemiologically, hand fractures account for approximately 10% to 20% of all fractures treated in emergency departments, with metacarpal and phalangeal fractures representing the vast majority. The demographic distribution is bimodal, peaking in young adult males (frequently resulting from high-energy trauma, sports injuries, or interpersonal violence) and an older, osteoporotic population (typically resulting from low-energy falls). Metacarpal fractures, particularly of the fifth ray (the so-called "boxer's fracture"), are the most common, followed closely by fractures of the proximal and distal phalanges. The mechanism of injury dictates the fracture pattern: axial loads typically produce intra-articular or comminuted metaphyseal fractures, torsional forces result in spiral or long oblique shaft fractures, and direct crush injuries lead to transverse or highly comminuted patterns with significant associated soft tissue compromise.
The pathophysiology of hand trauma extends far beyond the osseous injury. The soft tissue envelope of the hand is remarkably thin, providing minimal cushioning for the underlying skeleton and rendering the extensor mechanism, flexor tendons, and neurovascular bundles highly vulnerable to simultaneous injury. Furthermore, the healing process of hand fractures triggers an inflammatory cascade that invariably leads to edema. If this edema is not aggressively managed, protein-rich exudates organize into thick, unyielding scar tissue, binding the intimately associated gliding planes of the tendons to the healing bone. This patho-epidemiological reality underscores the absolute contraindication of prolonged immobilization; clinical union frequently precedes radiographic consolidation by many weeks, and early motion protocols must be initiated as soon as clinical stability is ensured to prevent devastating stiffness.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the surgical anatomy and biomechanics of the hand is non-negotiable for the orthopedic surgeon, as the deforming forces acting upon a fracture dictate both the pattern of displacement and the strategy for reduction. The skeletal architecture of the hand is organized into dynamic longitudinal and transverse arches. The proximal transverse arch is fixed at the level of the carpus, while the distal transverse arch is mobile at the level of the metacarpal heads, allowing the hand to cup and adapt to objects of varying shapes. The longitudinal arches consist of the individual digital rays, which pivot around the fixed central pillar of the second and third carpometacarpal (CMC) joints. The mobility of the first, fourth, and fifth CMC joints is crucial for opposition and grip strength.
The muscular anatomy is divided into extrinsic and intrinsic systems, which act as primary deforming forces following a fracture. In metacarpal shaft fractures, the volar interossei exert a strong proximal and volar pull on the distal fragment, predictably resulting in apex-dorsal angulation. Conversely, proximal phalanx fractures typically present with apex-volar angulation. This occurs because the interossei flex the proximal fragment via their insertion on the proximal phalanx base, while the central slip of the extensor mechanism extends the distal fragment. Understanding these vectors is essential for executing successful closed reductions, which rely on tensioning the intact soft tissue hinge to counteract these muscular forces.
The ligamentous anatomy of the metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joints is uniquely designed to provide stability in flexion and mobility in extension. The collateral ligaments of the MCP joints are eccentric and cam-shaped; they are lax in extension (allowing for abduction and adduction) and maximally taut in 70 to 90 degrees of flexion. This biomechanical quirk is the foundation of the "intrinsic-plus" or "safe" position of immobilization. If a hand is immobilized with the MCP joints in extension, the collateral ligaments will predictably shorten, resulting in an irreversible extension contracture. The PIP joints, however, must be immobilized in full extension to prevent shortening of the volar plate and subsequent flexion contractures.
Rotational deformities are notoriously elusive on two-dimensional imaging due to the cylindrical nature of the phalangeal and metacarpal shafts. An error in rotation may only become devastatingly obvious after the fracture has clinically healed and the patient attempts to form a composite fist. A rotational deformity of merely 5 degrees at the metacarpal base can translate to a 1.5 cm overlap at the fingertip, severely impairing grip strength and fine motor dexterity.
The Composite Fist Assessment
To accurately assess rotation, the surgeon must observe the kinematic alignment of the digits during active or passive flexion. Normally, when a composite fist is made, the longitudinal axes of all four fingers converge and point toward a single anatomical landmark: the scaphoid tubercle.
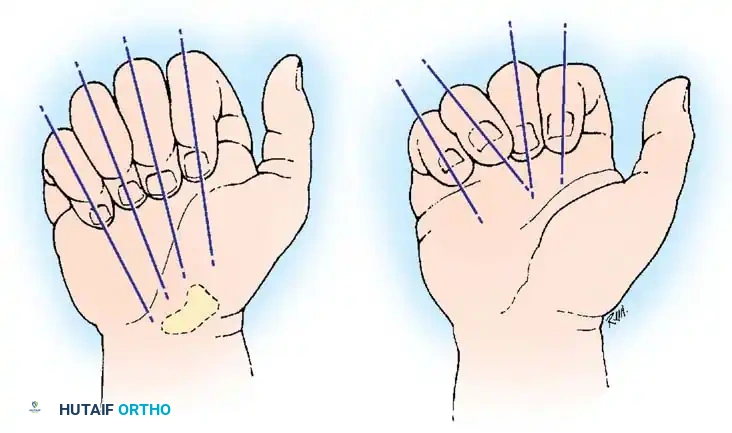
During the clinical evaluation of a fracture reduction, passively flexing all fingers fully at the MCP, PIP, and distal interphalangeal (DIP) joints simultaneously helps verify appropriate fracture rotation. If a fracture is malrotated, the affected finger will deviate from this convergence pathway, overriding or scissoring across an adjacent digit. This assessment must be performed meticulously prior to the application of any definitive cast or splint.
The Fingernail Plane Technique
Another highly reliable method for detecting subtle malrotation is the observation of the fingernail planes. With the fingers in partial flexion, the planes of the fingernails should align harmoniously, creating a smooth, uninterrupted arc.
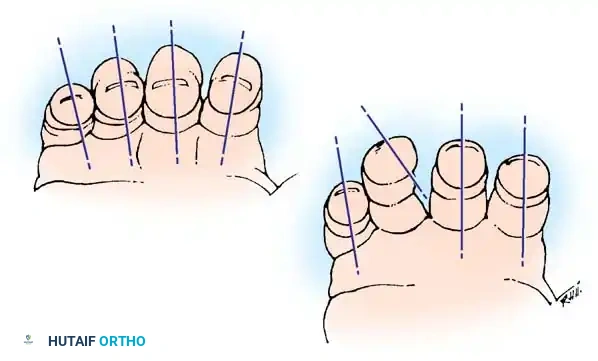
Comparing the injured hand to the contralateral, uninjured hand is essential. Any deviation in the plane of the nail bed relative to the adjacent digits strongly suggests a rotational malalignment at the fracture site that must be corrected prior to definitive fixation or casting.
Kinematics of the Fifth Ray
A common clinical pitfall involves the assessment of the little finger. The fifth digit possesses a natural tendency to overlap the ring finger during partial flexion. This phenomenon is permitted by the unique, highly mobile articulation of the fifth CMC joint, which allows for 20 to 30 degrees of flexion and a significant degree of internal rotation (opposition) to facilitate cupping of the palm. When a fracture limits the full flexion of the little finger, this partial-flexion overlap can be highly concerning. However, when full flexion of the little finger is accomplished, external rotation becomes biomechanically impossible due to the tightening of the collateral ligaments, whereas further internal rotation remains possible. Therefore, apparent internal malrotation at the fracture site during partial flexion may be a physiological illusion rather than a true deformity.
Exhaustive Indications and Contraindications
The decision-making process regarding the operative versus non-operative management of hand fractures requires a nuanced appreciation of the injury pattern, patient demands, and the inherent stability of the reduction. While a closed approach is generally preferred to minimize soft tissue trauma, specific indications necessitate operative osteosynthesis to restore the structural integrity of the hand. The surgeon must weigh the risks of surgical scarring and tendon adhesion against the risks of malunion, nonunion, and post-traumatic arthritis.
Operative intervention is unequivocally indicated in the setting of open fractures, which require immediate irrigation, debridement, and stabilization to prevent catastrophic infection and preserve neurovascular viability. Irreducible fractures or dislocations, often resulting from soft tissue interposition (such as volar plate interposition in complex MCP dislocations or the extensor mechanism in phalangeal fractures), similarly mandate open reduction. Unstable fracture patterns, including spiral or long oblique fractures of the metacarpals or phalanges, inherently shorten and malrotate under the pull of the intrinsic muscles and cannot be reliably maintained in a cast. Furthermore, intra-articular fractures with an articular step-off greater than 1 to 2 mm, or those involving more than 25% of the articular surface, generally require open reduction and internal fixation (ORIF) to restore joint congruity and prevent rapidly progressive post-traumatic osteoarthritis. Multiple ray involvement, often seen in "crushed hand" injuries, requires rigid fixation of the skeletal architecture to provide a stable foundation for the management of complex soft tissue, vascular, and nerve injuries.
Conversely, absolute contraindications to operative intervention in the hand are relatively rare but must be respected. Severe systemic illness or medical comorbidities that preclude the safe administration of anesthesia (even regional or local) represent a primary contraindication. Active, untreated local infections (unless the surgery is for debridement and stabilization of an infected nonunion or open fracture) preclude the placement of internal hardware. Relative contraindications revolve heavily around patient factors and the local tissue environment. Severe osteopenia, particularly in the elderly rheumatoid patient, may render standard screw and plate fixation impossible due to inadequate purchase, necessitating alternative strategies such as intramedullary wire fixation or functional bracing. A profoundly non-compliant patient who is unlikely to participate in postoperative therapy or adhere to weight-bearing restrictions is often better served with closed management, as the failure of operative fixation in a non-compliant patient carries a higher morbidity than a malunion.
| Category | Indications for Operative Intervention | Contraindications to Operative Intervention |
|---|---|---|
| Absolute | Open fractures requiring I&D; Irreducible dislocations (soft tissue interposition); Vascular compromise requiring skeletal stability for repair; Compartment syndrome. | Active, untreated local infection (non-trauma related); Severe systemic illness precluding anesthesia; Amputation indicated due to unsalvageable crush. |
| Relative / Biomechanical | Unstable spiral/oblique fractures; Intra-articular step-off > 1-2 mm; Articular involvement > 25%; Multiple ray injuries; Subungual hematoma with displaced distal phalanx fracture. | Severe osteopenia precluding hardware purchase; Highly comminuted fractures where surgery destroys remaining blood supply; Polytrauma requiring damage control. |
| Patient Factors | High-demand manual laborer or athlete requiring early return to function; Polytrauma patient needing hand for crutch weight-bearing. | Severe psychiatric illness or non-compliance; Advanced dementia preventing post-operative therapy participation; Heavy smoking (relative risk for nonunion). |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful hand surgery. The precise nature of hand anatomy leaves no room for intraoperative improvisation regarding implant selection or surgical approach. Radiographic evaluation must be exhaustive. Exact anteroposterior (AP) and lateral radiographs are mandatory, but standard views are often insufficient due to the superimposition of adjacent digits. Splay lateral (fan lateral) views can help isolate individual digits, while true lateral views of the 4th and 5th metacarpals are reliably obtained by positioning the hand in 10 degrees of supination, with the index and middle fingers held in 10 degrees of pronation. Oblique views are critical for assessing the reduction of intra-articular fractures, particularly at the metacarpal heads. For complex articular shear fractures or highly comminuted metaphyseal injuries, sagittal and coronal Computed Tomography (CT) reconstructions are increasingly necessary to map the fracture lines and plan the trajectory of lag screws or the placement of condylar plates.
Templating involves the careful selection of appropriate hardware based on the patient's specific anatomical dimensions. The surgeon must ensure the availability of comprehensive mini-fragment sets, typically including 1.2 mm, 1.5 mm, 2.0 mm, and 2.4 mm systems. The choice between low-profile plates, headless compression screws, and Kirschner wires (K-wires) depends entirely on the fracture geometry and the quality of the soft tissue envelope. For instance, a long oblique diaphyseal fracture may be ideally suited for multiple lag screws, whereas a transverse midshaft fracture will require the neutralization provided by a dorsal or lateral plate. Intraoperative fluoroscopy is mandatory; the C-arm must be positioned to allow for unimpeded visualization in multiple planes without compromising the sterile field.
Patient positioning and anesthesia represent a critical phase of pre-operative preparation. The patient is typically positioned supine with the operative extremity extended on a radiolucent hand table. A pneumatic tourniquet is routinely applied to the proximal arm to provide a bloodless surgical field, which is essential for identifying delicate neurovascular structures. Exsanguination is achieved with an Esmarch bandage prior to tourniquet inflation. However, the advent of Wide Awake Local Anesthesia No Tourniquet (WALANT) has revolutionized hand fracture management. By utilizing a tumescent mixture of lidocaine and epinephrine buffered with sodium bicarbonate, the surgeon can achieve both profound local anesthesia and excellent hemostasis without the need for a tourniquet or systemic sedation. The paramount advantage of WALANT in fracture care is the ability to assess the active motion of the digits intraoperatively. Once the fracture is provisionally or definitively fixed, the awake patient can actively flex and extend their fingers, allowing the surgeon to directly observe the tendon gliding, verify the absence of rotational deformity, and confirm the absolute stability of the construct before closure.
Step-by-Step Surgical Approach and Fixation Technique
When operative intervention is indicated, the surgical approach must respect the delicate soft tissue envelope of the hand, preserving the venous drainage and avoiding unnecessary stripping of the periosteum, which is the primary blood supply to the healing bone.
Metacarpal Fractures
For metacarpal shaft fractures, a dorsal longitudinal incision is typically utilized. If adjacent metacarpal fractures (e.g., 3rd and 4th) require fixation, a single incision placed strategically in the intermetacarpal space can access both rays, minimizing skin bridges and the risk of necrosis. The dissection proceeds through the subcutaneous tissue, taking immense care to identify and protect the longitudinal dorsal sensory branches of the ulnar and radial nerves, as well as the dorsal venous network. The extensor tendon is identified and usually retracted ulnarly or radially depending on the specific metacarpal. The dorsal periosteum is incised longitudinally and elevated minimally—only enough to expose the fracture site and allow for anatomic reduction.
Fixation techniques vary based on the fracture pattern. For long oblique or spiral fractures where the length of the fracture line is at least twice the diameter of the bone, lag screw fixation alone may be sufficient. The technique requires meticulous precision: the near cortex is overdrilled to the outer diameter of the screw (gliding hole), the far cortex is drilled to the core diameter (thread hole), and the screw is inserted to compress the fragments. For transverse or short oblique fractures, dorsal plating is the gold standard. Low-profile titanium plates are contoured to the dorsal anatomy of the metacarpal. At least three bicortical screws (six cortices) are required on each side of the fracture to provide adequate stability for early active motion. Alternatively, in cases of severe soft tissue compromise or when minimal dissection is desired, antegrade or retrograde intramedullary K-wire fixation can be employed, though this may require a longer period of protected immobilization compared to rigid plate fixation.
Phalangeal Fractures
Approaches to the phalanges demand even greater precision due to the intimate relationship between the bone and the complex extensor apparatus. For proximal phalanx fractures, a mid-axial approach or a dorsal approach can be utilized. The mid-axial approach is often preferred for shaft fractures as it avoids incising the extensor mechanism and prevents scarring the tendon directly to the bone, which is a primary cause of post-operative stiffness. The incision is made along the neutral line of the digit (connecting the apices of the flexion creases). The lateral band is identified and retracted dorsally, exposing the periosteum. Care must be taken not to violate the flexor tendon sheath volarly.
If a dorsal approach is chosen, particularly for intra-articular base fractures, the extensor mechanism can be split longitudinally (splitting the central slip) or the entire apparatus can be elevated. Fixation in the phalanges relies heavily on low-profile implants. Mini-condylar plates are excellent for peri-articular fractures, while crossed K-wires remain a versatile workhorse for highly comminuted patterns. When using K-wires, they should ideally be placed in a configuration that avoids crossing the fracture site at the exact same level to prevent a stress riser, and the pins must be meticulously cut and buried or capped to prevent pin tract infections and snagging on dressings. Regardless of the implant chosen, the hardware must be placed to avoid impinging on the lateral bands, the central slip, or the collateral ligaments, as any mechanical block will severely limit postoperative range of motion.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique and rigorous adherence to biomechanical principles, complications following hand fracture management are common and can be devastating to the patient's functional independence. The surgeon must be acutely aware of these risks, counsel the patient appropriately pre-operatively, and possess the armamentarium to manage them when they arise.
The most ubiquitous complication in hand fracture management is joint stiffness and loss of motion, occurring to some degree in up to 50% of operatively treated phalangeal fractures. Stiffness arises from a combination of factors: direct surgical trauma to the soft tissues, edema leading to capsular contracture, and the formation of dense adhesions between the healing bone and the adjacent flexor or extensor tendons. Prevention is paramount and relies on rigid fixation allowing for immediate early active motion. When stiffness becomes established, initial management consists of aggressive hand therapy, dynamic splinting, and serial casting. If non-operative measures fail after 3 to 6 months of a plateaued recovery, surgical salvage via tenolysis (freeing the tendon from scar tissue) and capsulotomy (releasing the contracted joint capsule) may be indicated. These salvage procedures are technically demanding and require an intensely motivated patient, as the postoperative rehabilitation is excruciating and failure rates are high.
Malunion is another significant complication, particularly prevalent in non-operatively managed fractures or those treated with inadequate fixation. Rotational malunion, as discussed previously, causes digital overlap and severely impairs grip. Angular malunion (e.g., severe apex-dorsal angulation in a metacarpal neck fracture) can lead to a prominent metacarpal head in the palm, causing pain with grasping, and can alter the biomechanics of the intrinsic muscles, leading to a pseudo-claw deformity. Shortening of the metacarpal can lead to an extensor lag. Salvage of a symptomatic malunion requires a corrective osteotomy. For rotational or angular deformities, a closing wedge or opening wedge osteotomy at the apex of the deformity, followed by rigid plate fixation, is performed.
Nonunion is exceedingly rare in the heavily vascularized hand skeleton, occurring in less than 1% of cases, but incidence increases significantly in the presence of severe bone loss, infection, or heavy tobacco use. Infection, while uncommon (1-2% in closed fractures, higher in open injuries), requires aggressive surgical debridement, hardware removal (if the fracture is healed or the hardware is loose), and culture-directed antibiotic therapy. Complex Regional Pain Syndrome (CRPS) is a catastrophic complication characterized by disproportionate pain, swelling, sudomotor changes, and profound stiffness. Its incidence is variable but it represents a severe threat to hand function. Early recognition, aggressive pain management, sympathetic blocks, and relentless physical therapy are the mainstays of salvage.
| Complication | Estimated Incidence | Primary Etiology / Risk Factors | Salvage Management Strategy |
|---|---|---|---|
| Joint Stiffness / Adhesions | 30% - 50% (Phalanges) | Prolonged immobilization, excessive surgical dissection, hematoma. | Aggressive hand therapy, dynamic splinting; Surgical tenolysis and capsulotomy if refractory > 6 months. |
| Malunion (Rotational/Angular) | 5% - 15% | Failure to recognize malrotation clinically, loss of reduction in cast, inadequate fixation. | Corrective osteotomy (closing/opening wedge or derotational) with rigid internal fixation. |
| Infection (Deep) | 1% - 3% (Closed) | Open fractures, prolonged surgical time, diabetes, poor soft tissue envelope. | Immediate I&D, culture-directed IV antibiotics, hardware removal if loose/unnecessary, external fixation if unstable. |
| Hardware Prominence / Tendon Irritation | 10% - 20% | Use of thick plates on dorsal phalanges, prominent screw heads, unburied K-wires. | Hardware removal after radiographic and clinical union is confirmed (typically > 3-4 months). |
| Nonunion | < 1% | Severe bone loss, infection, heavy smoking, inadequate immobilization/fixation. | Debridement of nonunion site, autologous bone grafting (e.g., distal radius or iliac crest), and rigid plate fixation. |
Phased Post-Operative Rehabilitation Protocols
The success of hand fracture management is ultimately determined not in the operating theater, but in the postoperative rehabilitation phase. The most perfectly executed osteosynthesis will yield a poor functional result if the rehabilitation protocol is inadequate or delayed. The surgeon and the certified hand therapist must work in lockstep to guide the patient through a phased recovery program.
The Concept of Clinical Union
Surgeons must clearly differentiate between clinical union and radiographic union to safely advance rehabilitation protocols. Clinical union is defined as the absence of pain at the fracture site upon palpation and the absence of motion at the fracture site under gentle manual stress. In the highly vascularized hand, clinical union typically occurs rapidly, usually at 3 to 4 weeks post-injury. Radiographic consolidation, characterized by bridging callus and the obliteration of the fracture line, may not be visible for 6 to 8 weeks, or even longer in fractures treated with absolute stability (primary bone healing without callus). Waiting for radiographic union to initiate motion is a historic error that guarantees a stiff, non-functional hand.
Phase 1: Immediate Post-Operative Phase (0-3 weeks)
Prolonged immobilization is the enemy of hand function. Once rigid internal fixation is achieved, or once a closed fracture demonstrates clinical stability, early active range of motion (AROM) must be initiated immediately. In Phase 1, the primary goals are edema control, wound care, and the prevention of tendon adhesions. The hand is typically placed in a custom thermoplastic splint in the intrinsic-plus position (wrist extended 20-30 degrees, MCP joints flexed 70-90 degrees, PIP/DIP joints fully extended) between exercise sessions. Patients are instructed to perform protected active motion exercises, such as tendon gliding exercises (straight fist, hook fist, composite fist), multiple times a day. Passive range of motion (PROM) is generally avoided in this phase to prevent stressing the fracture site or hardware construct. Edema is aggressively managed with elevation, compressive wrapping (e.g., Coban), and retrograde massage.
Phase 2: Intermediate Phase (3-6 weeks)
As the fracture achieves clinical union, the protocol advances. The custom splint is progressively weaned, initially being discontinued during the day and worn only at night or during high-risk activities. Passive range of motion (PROM) exercises are initiated to address any developing joint contractures. Blocking exercises are introduced; the patient stabilizes the proximal phalanx to isolate and actively flex the PIP joint, or stabilizes the middle phalanx to isolate the DIP joint. This differential gliding is critical to prevent the superficialis and profundus tendons from adhering to one another or to the underlying bone. Dynamic splinting may be introduced in this phase if specific joint contractures are identified (e.g., a dynamic extension splint for a PIP flexion contracture).
Phase 3: Late Phase and Strengthening (>6 weeks)
Once radiographic union begins to manifest and clinical union is solid, the focus shifts to aggressive strengthening and work conditioning. Progressive resistance exercises using therapy putty, hand grippers, and weights are employed to rebuild the intrinsic and extrinsic muscle mass that invariably atrophies during the recovery period. The patient is guided through functional tasks specific to their occupation or daily life. Return to full, unrestricted heavy manual labor or contact sports is typically permitted between 8 and 12 weeks, depending on the fracture pattern, the rigidity of the fixation, and the patient's functional recovery. By adhering to these strict biomechanical principles, respecting the soft tissue envelope, and prioritizing functional movement over radiographic perfection, the orthopedic surgeon can consistently achieve excellent outcomes in the management of complex hand fractures and dislocations.
Summary of Landmark Literature and Clinical Guidelines
The modern management of hand fractures is built upon a foundation of landmark biomechanical studies and evolving clinical guidelines. A historical appreciation of this literature is essential for the academic orthopedic surgeon. The concept of the "safe position" of immobilization was definitively established by James in the mid-20th century, who elucidated the cam-effect of the MCP collateral ligaments and the propensity for devastating extension contractures if the hand is immobilized improperly. This principle remains the bedrock of all non-operative and postoperative splinting protocols today.
In the realm of acceptable radiographic tolerances, clinical guidelines have evolved to favor function over perfect alignment. For fractures of the fifth metacarpal neck (boxer's fractures), landmark studies have demonstrated that volar angulation up to 40 to 70 degrees is well-tolerated functionally, largely due to the compensatory mobility of the fifth CMC joint. Conversely, fractures of the second and third metacarpals, which articulate with the rigid central pillar of the carpus, tolerate minimal angulation (strictly less than 10 degrees) before grip strength and biomechanics are compromised. Rotational deformity, as emphasized by Swanson and others, remains unforgiving across all digits, with zero degrees of malrotation considered the only acceptable clinical standard.
More recently, the paradigm shift toward Wide Awake Local Anesthesia No Tourniquet (WALANT) surgery, pioneered and popularized by Lalonde, has fundamentally altered the surgical approach to hand trauma. The ability to perform intraoperative active motion testing has drastically reduced the incidence of postoperative tendon adhesions and unrecognized malrotation, as the surgeon can dynamically verify the functional integrity of the repair prior to skin closure. Furthermore, the American Academy of Orthopaedic Surgeons (AAOS) and the American Society for Surgery of the Hand (ASSH) continue to publish updated clinical practice guidelines emphasizing the minimization of immobilization time and the judicious use of operative fixation only when closed functional management cannot reliably maintain acceptable biomechanical parameters. Familiarity with these guidelines and the historical literature ensures that the surgeon's practice remains evidence-based, patient-centered, and functionally oriented.
