Introduction and Historical Context
Freiberg infraction is a painful condition of the forefoot characterized by osteonecrosis (avascular necrosis) of the metatarsal head, most frequently involving the second ray. First described in 1914 by A.H. Freiberg, who reported six cases of "infraction" (an incomplete fracture of a bone without displacement of the fragments) of the second metatarsal head, the condition was initially attributed to acute mechanical trauma. In 1917, Campbell reported an identical pathologic process occurring in the third metatarsal head.
Over the past century, extensive clinical series—most notably by Smillie (41 cases) and Gauthier and Elbay (88 cases)—have expanded our understanding of the disease. While the exact etiology remains multifactorial and somewhat debated, Freiberg infraction is universally classified among the osteochondroses. It typically presents in the second decade of life, predominantly in adolescent females, and follows a predictable pathophysiologic cascade: osteonecrosis of the subchondral cancellous bone, structural collapse, and a subsequent reparative process that often results in a deformed, flattened metatarsal head and secondary osteoarthritis.
Pathophysiology and Biomechanics
The pathogenesis of Freiberg infraction is intimately tied to the unique biomechanics and vascular anatomy of the forefoot. The condition is widely considered to be the result of repetitive microtrauma superimposed on a susceptible vascular supply.
Biomechanical Factors
The second metatarsal is uniquely vulnerable to mechanical overload. It is typically the longest metatarsal and is rigidly stabilized at its base by the mortise created by the medial, intermediate, and lateral cuneiforms. Because the second ray is the least mobile of the metatarsals, it absorbs a disproportionate amount of sheer and compressive force during the terminal stance and toe-off phases of the gait cycle.
Excessive pressure on the metatarsal head during weight-bearing leads to repetitive microfractures within the subchondral bone. This mechanical overload compromises the delicate intraosseous microcirculation, leading to ischemia, loss of blood supply to the subchondral bone, and subsequent osteonecrosis.
The Pathologic Cascade
- Ischemia and Necrosis: Vascular compromise leads to necrosis of the subchondral cancellous bone.
- Subchondral Collapse: The necrotic bone loses its structural integrity, leading to the collapse of the cancellous architecture under the repetitive loads of weight-bearing.
- Cartilage Deformation: As the underlying bone collapses, the overlying articular cartilage deforms, leading to a flattened or centrally depressed metatarsal head.
- Synovitis and Contracture: The intra-articular degenerative process incites a robust inflammatory synovitis. If prolonged, this inflammation leads to capsular contracture and a marked limitation of metatarsophalangeal (MTP) joint motion, particularly in dorsiflexion (extension).
- Secondary Structural Changes: With the loss of MTP joint extension, weight-bearing forces are abnormally transmitted to the metatarsal shaft. This abnormal stress induces a hypertrophic response, resulting in widening of the metatarsal shaft due to bicortical thickening. Osteochondral fragmentation and loose body formation frequently occur around the degenerated metatarsal head.
Clinical Pearl: A misshapen metatarsal head is frequently an incidental radiographic finding in asymptomatic adults. Careful retrospective questioning often reveals a forgotten period of localized forefoot pain during adolescence, representing the acute phase of the infraction.
Clinical Presentation and Diagnosis
Patient Evaluation
Patients typically present with an insidious onset of pain localized to the involved MTP joint (most commonly the second, followed by the third). Symptoms are primarily exacerbated by weight-bearing activities, running, or wearing high-heeled shoes, which force the MTP joint into extension and increase joint reactive forces.
Physical examination reveals:
* Focal Tenderness: Exquisite point tenderness directly over the dorsal aspect of the involved metatarsal head.
* Swelling: Periarticular swelling and effusion secondary to reactive synovitis.
* Restricted Range of Motion: Limitation of MTP joint motion, with dorsiflexion being particularly restricted and painful.
* Plantar Callus: Occasionally, a transfer lesion or plantar keratosis may be present due to altered forefoot mechanics.
Imaging Studies
Radiography:
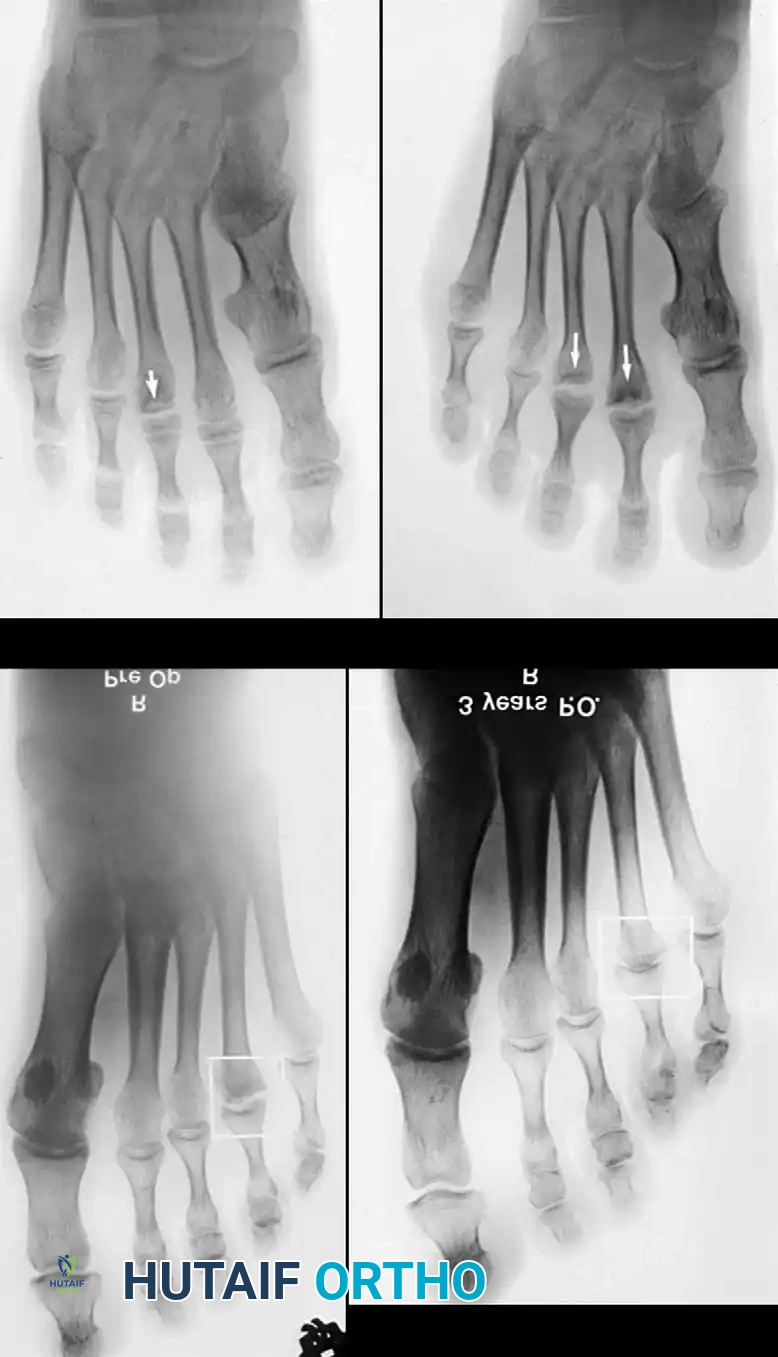
Weight-bearing anteroposterior (AP), lateral, and oblique radiographs of the foot are mandatory. Early radiographic findings may be subtle, showing only joint space widening due to effusion. As the disease progresses, classic signs emerge:
* Irregular ossification of the primary ossification center.
* Flattening and central depression of the metatarsal head.
* Widening and bicortical thickening of the metatarsal shaft.
* Osteochondral fragmentation and intra-articular loose bodies.

Magnetic Resonance Imaging (MRI):
MRI is highly sensitive for detecting early Freiberg infraction before radiographic collapse occurs. It is invaluable for evaluating the extent of bone marrow edema, the viability of the metatarsal head, and the integrity of the articular cartilage. T1-weighted images typically show decreased signal intensity in the subchondral bone, while T2-weighted STIR images highlight bone marrow edema and reactive synovitis. MRI is particularly useful in surgical planning to determine if the lesion is strictly localized to the dorsal aspect of the metatarsal head.
Conservative Management
The majority of patients with Freiberg infraction can be managed successfully with nonoperative modalities, particularly if diagnosed in the early stages before severe structural collapse occurs. The primary goal is to offload the affected metatarsal head and reduce inflammation.
- Activity Modification: Immediate cessation of high-impact activities (running, jumping).
- Orthotic Management: Semirigid orthoses with a metatarsal pad placed proximal to the involved metatarsal head to unload the joint. Metatarsal bars or stiff-soled shoes (e.g., carbon fiber inserts) limit MTP joint extension during toe-off.
- Immobilization: In acute, highly symptomatic cases, a short leg walking cast with a toe extension or a controlled ankle motion (CAM) boot may be required for 4 to 6 weeks.
- Assistive Devices: Occasionally, crutches are necessary for a brief period of strict non-weight-bearing to allow severe acute synovitis to subside.
Surgical Indications and Decision Making
Surgical intervention is indicated when conservative management fails to relieve pain and functional limitations after a minimum of 3 to 6 months. The choice of procedure depends on the stage of the disease, the extent of articular cartilage damage, and the patient's age and activity level.
Historically, several surgical treatments have been described:
1. Resection of the metatarsal head (Giannestras): Generally abandoned due to severe transfer metatarsalgia and toe shortening.
2. Elevation of the depressed fragment and bone grafting (Smillie): Technically demanding and often yields unpredictable results in late stages.
3. Resection of the base of the proximal phalanx with syndactylization (Trott): Shortens the toe significantly. Because 90% of patients are in late adolescence or early adulthood, this resection should be avoided.
4. Dorsal closing wedge osteotomy (Gauthier and Elbay): Excellent for dorsal-specific lesions.
5. Joint débridement and metatarsal head remodeling (Freiberg and Mann): The most versatile and frequently utilized procedure for advanced degenerative changes.
Surgical Warning: The patient must be explicitly informed during the preoperative consent process that some permanent limitation of MTP joint motion is expected postoperatively. Because motion in the affected joint is frequently limited prior to surgery, this is rarely a deterrent, but managing expectations is critical.
Surgical Techniques
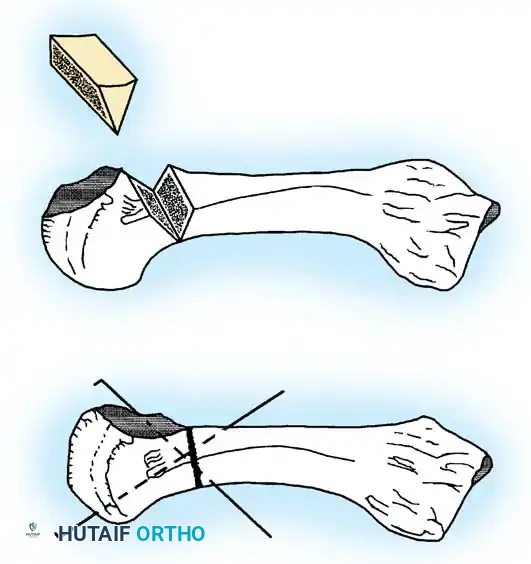
Technique 1: Dorsal Closing Wedge Osteotomy (Chao et al.)
Indications:
This extra-articular osteotomy is ideal for intermediate stages of Freiberg infraction where the necrotic lesion is localized strictly to the dorsal aspect of the metatarsal head, and the plantar articular cartilage remains healthy and viable. The goal is to rotate the healthy plantar cartilage dorsally to articulate with the proximal phalanx.
Surgical Steps:
- Positioning and Approach:
Place the patient supine with a calf or thigh tourniquet. Make a 3- to 4-cm dorsal longitudinal incision centered over the involved MTP joint, lateral to the extensor hallucis longus (if the second ray is involved). - Soft Tissue Dissection:
Retract the extensor tendons. Make a longitudinal incision in the dorsal capsule to expose the joint. - Joint Débridement:
Perform a thorough joint inspection. Débride the joint of any loose osteochondral fragments and perform a partial synovectomy to remove inflamed tissue. - Osteotomy Execution:
Identify the distal normal metaphysis, just proximal to the necrotic lesion. Using an oscillating microsaw, perform a dorsal closing wedge osteotomy.- The base of the wedge is dorsal, and the apex is plantar.
- Crucial Step: Do not remove the necrotic lesion itself. Instead, remove sufficient metaphyseal bone to allow the distal fragment (the metatarsal head) to be rotated proximally and dorsally.
- The angle of the closing wedge must be carefully calculated to maintain the length of the involved metatarsal bone as much as possible, preventing transfer metatarsalgia.
- Rotation and Articulation:
Close the osteotomy site. This maneuver rotates the healthy plantar aspect of the metatarsal head into direct articulation with the base of the proximal phalanx. - Fixation:
Temporarily fix the osteotomy with two crossed percutaneous Kirschner wires (K-wires) driven from distal-dorsal to proximal-plantar. Ensure the wires do not violate the newly aligned articular surface.
Postoperative Protocol (Dorsal Closing Wedge Osteotomy):
* 0-4 Weeks: A light compressive dressing is applied. The foot is immobilized in a short leg walking cast or rigid CAM boot. Weight-bearing is restricted to heel-touch or non-weight-bearing depending on fixation stability.
* 4 Weeks: The percutaneous K-wires are removed in the clinic. Weight-bearing is allowed as tolerated in a stiff-soled shoe.
* 8 Weeks: Patients are restricted from running, jumping, or engaging in any strenuous physical activity for a minimum of 8 weeks postoperatively to ensure complete osseous union.
Technique 2: Joint Débridement and Metatarsal Head Remodeling (Freiberg and Mann)
Indications:
This is the preferred procedure for advanced stages of Freiberg infraction where there is extensive central depression, diffuse cartilage damage, and significant osteophyte formation. It relies on aggressive débridement, soft tissue balancing, and biological remodeling of the joint space.
Surgical Steps:
- Incision and Exposure:
Make an angled or lazy-S incision, the apex of which is at the lateral margin of the MTP joint. This prevents dorsal scar contracture. Carefully identify and ligate any crossing veins returning to the dorsal venous arch to prevent postoperative hematoma. - Extensor Hood Dissection:
Expose the entire extensor expansion over the MTP joint. Identify the extensor digitorum brevis (EDB) tendon as it joins the extensor digitorum longus (EDL). Section the EDB at this juncture (tenotomy) to remove its deforming force. - Capsulotomy:
Incise the extensor hood just lateral to the EDL tendon and retract the EDL medially. Perform a longitudinal capsulotomy. Enter the MTP joint and reflect the capsule medially and laterally by sharp dissection to fully expose the metatarsal head.- Observation: The degree of macroscopic degeneration, pitting, and cartilage loss on the metatarsal head is often strikingly more severe than anticipated from preoperative radiographs.
- Débridement and Release:
Remove all loose osteochondral fragments and perform a thorough synovectomy. Distract the toe manually and flex it acutely to expose the entire plantar aspect of the metatarsal head. Both the medial and lateral collateral ligaments may require division to achieve adequate exposure. - Assessment and Soft Tissue Balancing:
Evaluate the articular surface. If the joint has remodeled favorably and the cartilage appears surprisingly intact, limit the bony work. Instead, focus on soft tissue decompression: perform a Z-plasty lengthening (8 to 12 mm) of the EDL tendon to relieve chronic extensor pressure on the joint. - Metatarsal Head Remodeling (Arthroplasty):
If the metatarsal head is severely pitted and deformed, aggressive contouring is required.- Use a rongeur or a high-speed burr to remove the damaged articular cartilage.
- The surface of the metatarsal head is usually depressed dorsally and centrally. Round the remainder of the head to match this depth. This typically requires the circumferential removal of 3 to 4 mm of bone.
- Critical Pitfall: When remodeling the metatarsal head, meticulously palpate the plantar aspect. Ensure that absolutely no osteophytes or sharp bony prominences remain on the plantar surface, as these will cause intractable postoperative plantar keratosis and pain.
- Closure:
Irrigate the joint copiously with sterile saline while actively flexing and extending the toe to flush out any microscopic cartilage or bony debris. Secure meticulous hemostasis by direct pressure—this is a vital step to prevent postoperative arthrofibrosis secondary to hemarthrosis. Close the capsule with fine absorbable sutures (e.g., 3-0 or 4-0 Vicryl), and apply a bulky compressive dressing that holds the joint in a reduced, neutral position.
Postoperative Protocol (Joint Débridement and Remodeling):
* 0-48 Hours: Continuous strict elevation of the foot is highly recommended to minimize swelling and bleeding. The patient is allowed to mobilize for essential needs in a wooden-soled or rigid postoperative shoe.
* 2 Weeks: The skin sutures are removed. The forefoot is redressed, ensuring the toe is taped or splinted in the desired neutral position to prevent dorsal drift.
* 4 Weeks: The patient is transitioned to a wide toe-box shoe. Active and gentle active-assisted range of motion exercises of the involved MTP joint are initiated and strongly encouraged to prevent capsular adhesions.
* Long-term: Metatarsal bars or orthotic pads should be utilized for 3 to 6 months postoperatively to protect the remodeling joint interface.
Complications and Outcomes
Surgical management of Freiberg infraction generally yields high patient satisfaction, provided expectations regarding postoperative stiffness are managed. Potential complications include:
* Persistent Stiffness: The most common sequela. Aggressive early ROM (after 4 weeks) is essential.
* Transfer Metatarsalgia: Can occur if the osteotomy excessively shortens the metatarsal or alters the declination angle.
* Progression of Arthrosis: In severe cases, joint remodeling may eventually fail, necessitating a salvage procedure such as an interpositional arthroplasty or, rarely, MTP joint resection arthroplasty.
By adhering to strict biomechanical principles—whether rotating healthy cartilage via osteotomy or meticulously decompressing and remodeling the joint—the orthopedic surgeon can reliably restore function and alleviate pain in patients suffering from Freiberg infraction.
