Comprehensive Introduction and Patho-Epidemiology
Brachymetatarsia is a complex structural anomaly of the forefoot characterized by the abnormal, premature cessation of growth in one or more metatarsals, resulting in a significantly shortened ray. Epidemiologically, this condition exhibits a striking and well-documented female predilection, with literature citing a female-to-male ratio as disproportionate as 25:1. The overall incidence in the general population is estimated to be approximately 1 in 2,500 to 1 in 4,000, though this may be underreported due to asymptomatic cases that never present for clinical evaluation. The fourth metatarsal is overwhelmingly the most frequently affected ray, followed in incidence by the first and fifth metatarsals. Bilateral presentation is not uncommon, occurring in roughly 50% to 72% of documented cases, suggesting a strong underlying genetic or systemic developmental component.
The etiology of brachymetatarsia is broadly stratified into congenital and acquired categories. Congenital brachymetatarsia is primarily driven by the premature closure of the metatarsal epiphyseal plate. In the lesser metatarsals, the secondary center of ossification is located distally, whereas in the first metatarsal, it is located proximally. Premature fusion of these physes halts longitudinal growth prematurely while the adjacent metatarsals continue their normal developmental trajectory. This congenital form may present as an isolated idiopathic anomaly or in association with systemic genetic syndromes. Notable syndromic associations include Turner syndrome, Down syndrome, Apert syndrome, and the Albright hereditary osteodystrophy spectrum (pseudohypoparathyroidism and pseudo-pseudohypoparathyroidism). In these syndromic presentations, multifocal and bilateral involvement is frequently observed.
Acquired brachymetatarsia, conversely, results from an external insult to the physis during the skeletal growth phase. Trauma is the most prevalent acquired cause, encompassing Salter-Harris fractures that result in physeal arrest or crush injuries that compromise the vascular supply to the growth plate. Other acquired etiologies include pediatric osteomyelitis, septic arthritis of the metatarsophalangeal (MTP) joint, childhood radiation therapy, or iatrogenic causes following aggressive surgical interventions in the pediatric forefoot. Regardless of the etiology, the resulting anatomical discrepancy becomes progressively more apparent during the adolescent growth spurt, which is the typical age of clinical presentation.
The pathoanatomy of brachymetatarsia extends far beyond the mere cosmetic appearance of a shortened toe. The primary biomechanical consequence is the profound disruption of the normal weight-bearing mechanics of the forefoot. During the terminal stance and preswing phases of the gait cycle, the forefoot must act as a rigid lever to facilitate forward propulsion. A shortened metatarsal fails to engage the ground effectively, leading to a catastrophic failure of load sharing. Consequently, the ground reaction forces that should have been absorbed by the affected ray are forcefully transferred to the adjacent, normal-length metatarsal heads. This pathological biomechanical shift manifests clinically as severe transfer metatarsalgia, the development of intractable plantar keratoses (IPK) beneath the overloaded adjacent metatarsal heads, and progressive dorsal soft-tissue contractures. The extensor tendons, lacking the normal bony tension, gradually contract, causing the affected toe to subluxate dorsally and rest on the dorsum of the foot—a deformity classically termed the "floating toe."
Detailed Surgical Anatomy and Biomechanics
A rigorous understanding of forefoot biomechanics and surgical anatomy is the cornerstone of successful reconstructive planning for brachymetatarsia. The metatarsal heads naturally align to form a smooth, parabolic arc, often referred to as the Maestro curve or the Lelièvre parabola. This geometric alignment is not merely aesthetic; it is a critical biomechanical requirement that ensures an even, physiological distribution of plantar pressures across the forefoot during the propulsive phase of gait. The second metatarsal is typically the longest and most rigid, serving as the keystone of the transverse arch, with the first, third, fourth, and fifth metatarsals progressively decreasing in relative projection.
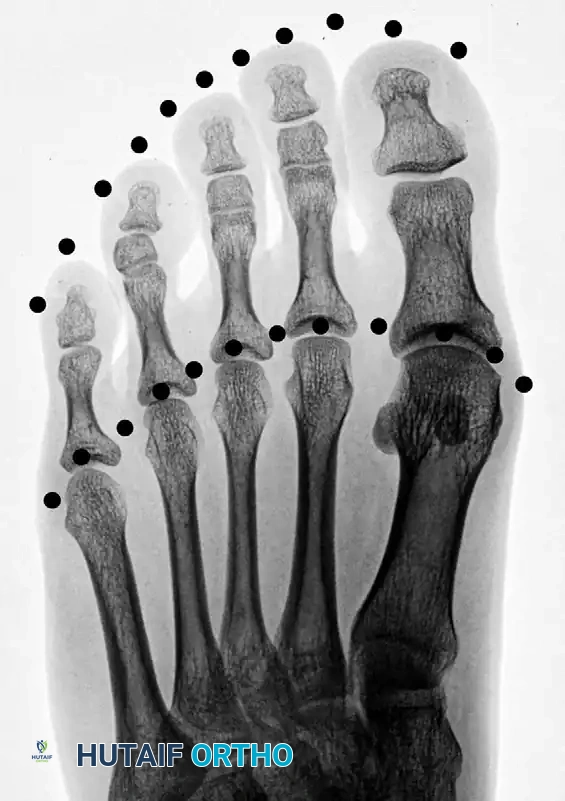
Figure 1: Normal toe-tip and metatarsal head parabolas (dotted lines), demonstrating the ideal geometric arc required for optimal forefoot biomechanics.
When brachymetatarsia is present, this delicate parabolic arc is severely disrupted. The affected metatarsal head is proximally retracted, creating a functional void in the transverse arch. The distance required to advance the affected metatarsal head distally to restore it to the ideal parabola dictates the precise surgical lengthening goal.

Figure 2: Disruption of the normal parabolic arc associated with brachymetatarsia of the first metatarsal.
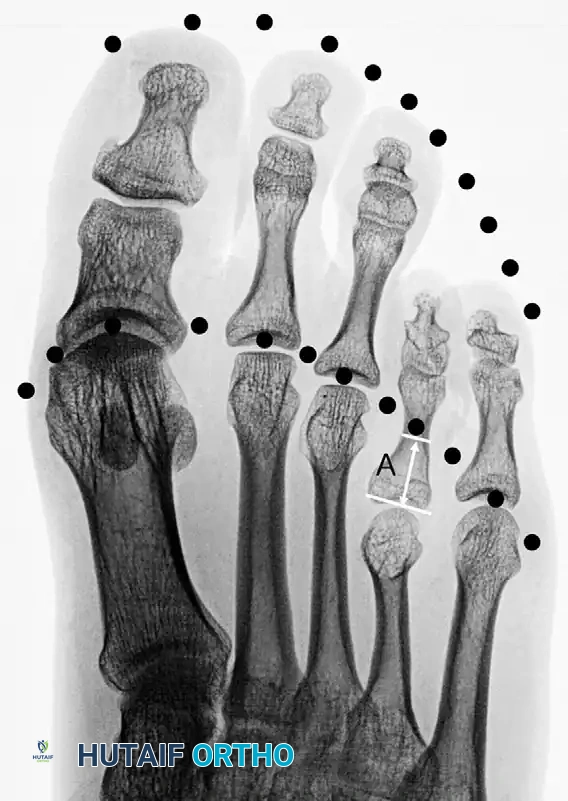
Figure 3: Disruption with brachymetatarsia of the fourth metatarsal. The distance marked “A” represents the precise length needed to obtain an ideal parabola.
The vascular anatomy of the metatarsals is of paramount importance, particularly when performing corticotomies for distraction osteogenesis. The blood supply to the metatarsal diaphysis is dual-sourced: the nutrient artery, which supplies the endosteal circulation, and the periosteal plexus, which supplies the outer cortical layers. The periosteal network is exceptionally robust and is the primary driver of regenerate bone formation (callotasis) during gradual lengthening. Surgical techniques must meticulously preserve the periosteal sleeve to prevent avascular necrosis of the intercalary segment and to ensure robust osteogenesis. Disruption of this dual blood supply through aggressive stripping or thermal necrosis during the osteotomy will inevitably lead to delayed union or nonunion.
The soft tissue envelope surrounding the metatarsals presents one of the most formidable challenges during lengthening procedures. The extensor digitorum longus (EDL), extensor digitorum brevis (EDB), flexor digitorum longus (FDL), and flexor digitorum brevis (FDB) tendons, along with the intrinsic lumbricals and interossei, all cross the MTP joint. As the metatarsal is surgically lengthened, these structures are subjected to immense tension. Because skeletal tissue responds to distraction osteogenesis more rapidly than tendinous and neurovascular tissues (which undergo a process of stretch-induced neogenesis), the lagging soft tissues create a profound tethering effect. This tethering pulls the proximal phalanx dorsally, risking severe MTP joint subluxation or frank dislocation. Furthermore, the plantar digital nerves and arteries are susceptible to stretch-induced neuropraxia and ischemia, necessitating strict adherence to safe distraction rates.
Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention for brachymetatarsia must be carefully weighed against the arduous nature of the recovery, particularly when utilizing external fixation. Surgery is never indicated solely for mild cosmetic concerns in an asymptomatic patient. The primary indication for surgical lengthening is intractable transfer metatarsalgia that has proven refractory to comprehensive conservative management, including custom orthotics, metatarsal pads, and modified footwear with deep toe boxes.
Secondary indications include severe dorsal subluxation of the affected toe (the "floating toe" deformity) that causes painful friction against footwear, recurrent ulcerations or intractable plantar keratoses on the adjacent overloaded rays, and profound psychological distress that significantly impairs the patient's quality of life and psychosocial functioning. In cases of first metatarsal brachymetatarsia, surgical intervention is more aggressively indicated due to the critical role of the first ray in the windlass mechanism and overall medial column stability; a shortened first ray rapidly leads to severe second ray overload and subsequent crossover toe deformities.
Contraindications must be rigorously evaluated during the preoperative assessment. Absolute contraindications include active local or systemic infection, severe peripheral vascular disease (PVD) that would preclude wound healing or tolerate the vascular stretch of lengthening, and Charcot neuroarthropathy. Perhaps the most critical absolute contraindication is a non-compliant patient. Distraction osteogenesis requires meticulous daily pin care, precise adjustments of the external fixator multiple times a day, and strict adherence to weight-bearing restrictions. A patient lacking the cognitive capacity, social support, or psychological fortitude to manage an external fixator for several months is an absolute contraindication for callotasis.
Relative contraindications include poorly controlled diabetes mellitus, heavy tobacco use (which significantly impairs osteogenesis and increases nonunion rates), severe osteoporosis (which compromises half-pin purchase and risks fixator pull-out), and open physes in a pediatric patient. While some surgeons will perform lengthening in children with open physes, great care must be taken to avoid physeal injury, and the patient's family must understand the risk of recurrence if the adjacent metatarsals continue to grow postoperatively.
| Category | Specific Conditions | Clinical Rationale |
|---|---|---|
| Indications | Intractable transfer metatarsalgia | Failure of load sharing causing severe pain under adjacent normal-length metatarsal heads. |
| "Floating toe" causing footwear impingement | Dorsal contracture leading to painful friction, corns, and inability to wear standard shoes. | |
| Severe psychological/cosmetic distress | Significant negative impact on body image and psychosocial wellbeing, particularly in adolescents. | |
| Relative Contraindications | Poorly controlled Diabetes Mellitus | Increased risk of pin tract infections and impaired osteogenesis. |
| Active tobacco use | Nicotine-induced vasoconstriction severely inhibits regenerate bone formation and soft tissue healing. | |
| Severe osteoporosis | Poor cortical bone density leads to mini-Schanz pin loosening and fixator failure. | |
| Absolute Contraindications | Active local or systemic infection | High risk of deep space infection or osteomyelitis with the introduction of percutaneous pins. |
| Severe Peripheral Vascular Disease (PVD) | Inability of the vascular tree to adapt to the stretch, risking digital ischemia and necrosis. | |
| Patient non-compliance / Psychiatric instability | Inability to perform daily fixator adjustments and pin care will lead to catastrophic failure. |
Pre-Operative Planning, Templating, and Patient Positioning
Preoperative planning for brachymetatarsia reconstruction is highly quantitative and relies on meticulous clinical and radiographic evaluation. The clinical examination must assess the flexibility of the MTP joints, the presence of fixed soft tissue contractures, and the exact location of plantar keratoses. A thorough neurovascular assessment is mandatory, documenting baseline capillary refill, pedal pulses, and protective sensation. The surgeon must also carefully differentiate brachymetatarsia from other pathologies that alter metatarsal mechanics, most notably Freiberg infraction (avascular necrosis of the metatarsal head).
While distinct from brachymetatarsia, Freiberg disease similarly disrupts the articular mechanics of the lesser rays and can be exacerbated by abnormal stress distributions in the forefoot. It most commonly affects the second metatarsal head but can present atypically.

Figure 4: Freiberg infraction presenting in an uncommon location.

Figure 5: Three years following joint débridement and remodeling of the metatarsal head. While motion remains limited, the patient is highly active and asymptomatic.
Systemic factors, such as hemoglobinopathies, can predispose patients to multifocal osteonecrosis in the forefoot, which must not be confused with congenital brachymetatarsia.

Figure 6: Freiberg infraction of the third metatarsal head in a teenage girl (arrow).

Figure 7: One year later, the second metatarsal head is also involved. Arrows indicate Freiberg infractions on both the second and third metatarsal heads in a patient with a known hemoglobinopathy.
Radiographic templating utilizes standard weight-bearing anteroposterior (AP), lateral, and oblique views of the foot. On the AP radiograph, the normal metatarsal parabola (Maestro curve) is traced. The exact degree of shortening is calculated by measuring the longitudinal distance required to advance the affected metatarsal head to intersect this ideal parabolic arc. This measurement dictates the surgical lengthening goal. Crucially, the surgeon must apply the "40% Rule": lengthening a metatarsal by more than 40% of its original native length significantly increases the risk of neurovascular compromise, severe joint stiffness, and MTP joint subluxation. If the required length exceeds this threshold, adjunctive soft tissue releases or shortening osteotomies of the adjacent metatarsals may be required to achieve a harmonious parabola without over-stretching the affected ray.
The choice of surgical technique depends directly on the calculated lengthening requirement. One-stage lengthening with an interpositional structural bone graft (autograft from the iliac crest or allograft) is generally reserved for mild deformities where the required lengthening is less than 10 to 15 mm.
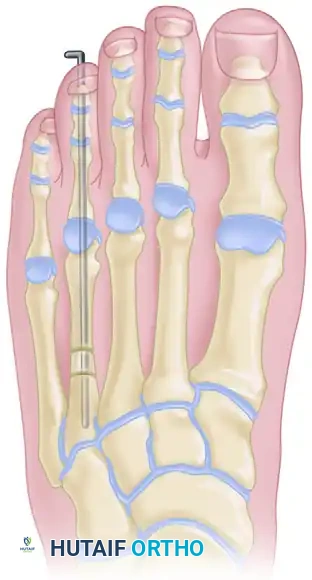
Figure 8: Lengthening of the metatarsal utilizing a one-stage allograft interposition technique. Rigid internal fixation (typically with a plate or intramedullary K-wire) is required to stabilize the intercalary graft.
Attempting acute lengthening beyond 15 mm places excessive, immediate tension on the neurovascular bundles, risking acute digital ischemia. For lengthening requirements exceeding 15 mm, gradual distraction osteogenesis (callotasis) is the undisputed gold standard.
In the operating room, the patient is positioned supine on a radiolucent table. A small bump may be placed under the ipsilateral hip to correct natural external rotation of the lower extremity, ensuring the foot points directly toward the ceiling. A calf or thigh tourniquet is applied to provide a bloodless surgical field, which is critical for identifying the delicate periosteal layer. Regional anesthesia, such as a popliteal sciatic nerve block combined with a saphenous nerve block, provides excellent intraoperative anesthesia and prolonged postoperative analgesia. The fluoroscopy unit (C-arm) is positioned entering from the contralateral side or distal end of the table, allowing for rapid, unobstructed AP and lateral imaging throughout the procedure.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of distraction osteogenesis for brachymetatarsia demands exacting precision. The technique detailed herein utilizes a unilateral external fixator, based on the principles popularized by Lee et al. Meticulous pin placement, preservation of the periosteal sleeve, and a low-energy corticotomy are the triad of success for this procedure.
Under strict fluoroscopic guidance, the initial step is the insertion of the mini-Schanz half-pins. The goal is to place two pins into the proximal metaphysis and two into the distal metaphysis of the affected metatarsal. For first metatarsal brachymetatarsia, 3.0 mm diameter pins are typically utilized due to the robust diaphyseal diameter. These are directed from medial to lateral to avoid the extensor hallucis longus (EHL) tendon dorsally and the sesamoid apparatus plantarly. The unilateral external fixator is applied to the medial aspect of the first ray. For the more common fourth metatarsal brachymetatarsia, 2.0 mm diameter mini-Schanz pins are required. These are inserted on the dorsolateral aspect of the fourth metatarsal. Extreme care must be taken to avoid entrapping the extensor digitorum longus (EDL) tendon to the fifth toe. A critical technique pearl is to position the proximal two pins lateral to the fifth EDL tendon, and the two distal pins medial to it, creating a safe soft-tissue corridor that prevents tendon tethering during the distraction phase.
Proper alignment of the external fixator rail is arguably the most critical step in preventing axial deviation during the lengthening process. The fixator rail dictates the vector of distraction.
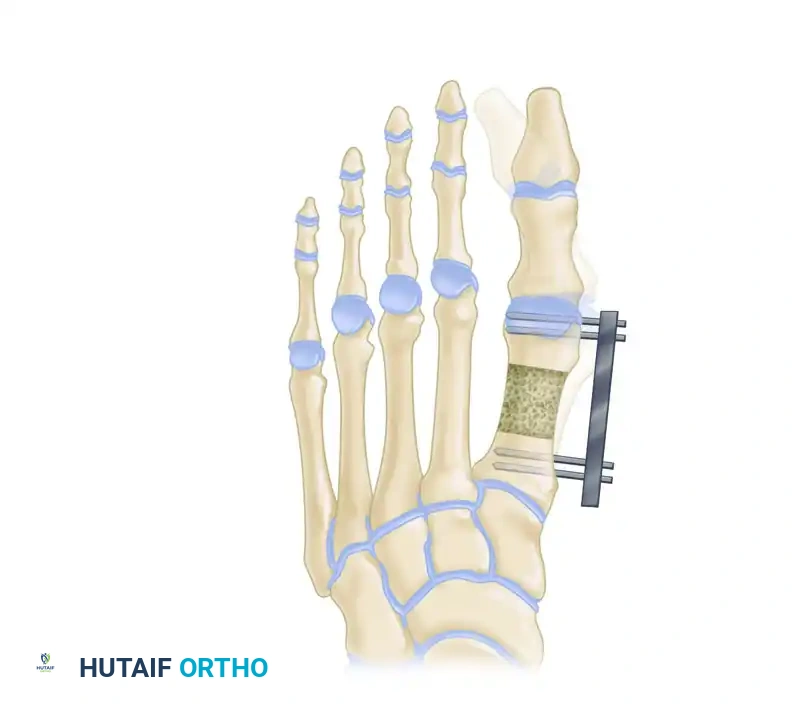
Figure 9: External fixator application in the transverse plane. The fixator must be applied as parallel as possible to the axis of the second metatarsal to ensure a straight longitudinal distraction.
In the transverse plane, the fixator must be applied parallel to the longitudinal axis of the foot (often referenced off the second metatarsal) to prevent varus or valgus deviation. In the sagittal plane, the rail must be strictly parallel to the plantar surface of the foot.

Figure 10: External fixator application in the sagittal plane. The rail must be parallel to the plantar surface of the foot to prevent iatrogenic elevation or depression of the metatarsal head.
Once the pins are placed and the fixator alignment is confirmed, the corticotomy is performed. A 1.5-cm longitudinal incision is made directly over the metatarsal shaft, perfectly centered between the proximal and distal pin clusters. Careful blunt dissection is carried down to the bone, gently retracting the extensor tendons. The periosteum is longitudinally incised and meticulously elevated using a fine periosteal elevator. Preserving this periosteal sleeve is absolutely vital, as it contains the osteoprogenitor cells responsible for intramembranous ossification during callotasis.
The bone cut must be a low-energy corticotomy. Using a motorized sagittal saw with continuous, copious cold saline irrigation, a transverse cut is made perpendicular to the plantar surface of the foot. Thermal necrosis from a hot saw blade will instantly destroy the osteogenic potential of the bone ends, virtually guaranteeing a nonunion. Alternatively, a multiple drill-hole technique using a 1.5 mm drill bit, followed by connection with a sharp, thin osteotome, can be utilized to minimize thermal injury. Once the osteotomy is complete, the surgeon must confirm the proper direction of metatarsal lengthening by acutely distracting the osteotomy approximately 5 mm using the external fixator mechanism. The direction of distraction is assessed under fluoroscopy to ensure there is no angular or translational deformity. After confirmation, the bone surfaces are restored to complete, compressed apposition (zero distraction) to initiate the latency phase. The periosteum is meticulously closed over the osteotomy site with fine absorbable sutures, followed by standard layered soft tissue closure.
Complications, Incidence Rates, and Salvage Management
While distraction osteogenesis is a highly effective and versatile technique for managing severe brachymetatarsia, it is fraught with a distinct and challenging complication profile. The surgeon must be prepared to identify and manage these complications promptly to prevent catastrophic failure of the reconstruction.
Pin tract infections are by far the most common complication, with reported incidence rates ranging from 30% to over 50% in some series. These typically present as localized erythema, serous or purulent discharge, and pain at the pin-skin interface. The vast majority of these are superficial and can be effectively managed with aggressive local pin care (using chlorhexidine or sterile saline solutions) and a short course of oral antibiotics targeting common skin flora (e.g., first-generation cephalosporins). Deep pin tract infections that progress to osteomyelitis or cause catastrophic loosening of the mini-Schanz pins are rare but require immediate pin removal, debridement, and conversion to alternative fixation or premature cessation of the lengthening process.
Metatarsophalangeal (MTP) joint subluxation or frank dislocation is a severe complication directly related to the soft tissue tethering effect. As the bone lengthens, the unyielding extensor and flexor tendons act as a bowstring, driving the proximal phalanx dorsally. The incidence of MTP subluxation increases exponentially when lengthening exceeds 40% of the native bone length. To prevent this, many surgeons advocate for prophylactic pinning of the MTP joint. A smooth K-wire is driven antegrade through the toe and retrograde into the metatarsal head and shaft, holding the joint in a neutral or slightly plantarflexed position for the duration of the distraction phase. If subluxation occurs during lengthening without prophylactic pinning, the distraction must be immediately halted, and a percutaneous extensor tendon lengthening or MTP joint capsulotomy may be required.
Axial deviation, delayed union, and premature consolidation represent failures of the biological and mechanical environment of the regenerate bone. Axial deviation (usually plantarflexion or dorsiflexion of the distal fragment) occurs due to improper initial fixator alignment or the asymmetric pull of the soft tissues. This requires early identification on bi-weekly surveillance radiographs and potential mechanical adjustment of the fixator. Premature consolidation occurs if the biological healing outpaces the distraction rate, often necessitating a return to the operating room to re-cut the bone. Conversely, delayed union or nonunion occurs if the distraction rate is too fast, tearing the delicate osteogenic tissue, or if the periosteal blood supply was destroyed during surgery. This is often managed via the "accordion technique"—alternating compression and distraction of the fixator over several weeks to stimulate the biological healing cascade—or ultimately, by utilizing autologous bone grafting.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Prevention |
|---|---|---|---|
| Pin Tract Infection | 30% - 50% | Poor local hygiene, skin tension around pins. | Local care, oral antibiotics. Prevent with meticulous daily pin care and releasing skin tension during insertion. |
| MTP Joint Subluxation | 15% - 30% | Soft tissue tethering (extensor tendons), lengthening >40%. | Halt distraction, extensor tenotomy, capsulotomy. Prevent with prophylactic transarticular K-wire pinning. |
| Axial Deviation | 10% - 20% | Improper fixator alignment, asymmetric muscle pull. | Adjust fixator trajectory. Prevent by ensuring fixator rail is perfectly parallel to the 2nd metatarsal and plantar foot. |
| Delayed Union / Nonunion | 5% - 10% | Thermal necrosis during corticotomy, distraction too fast. | "Accordion technique" (cyclic compression/distraction), bone grafting. Prevent with cold saline irrigation during bone cut. |
| Premature Consolidation | < 5% | Distraction rate too slow, latency period too long. | Return to OR for repeat corticotomy. Prevent by adhering strictly to the 0.75 mm/day distraction protocol. |
Phased Post-Operative Rehabilitation Protocols
The ultimate success of distraction osteogenesis relies just as heavily on strict adherence to the postoperative rehabilitation protocol as it does on the surgical execution. The postoperative course is an arduous journey for the patient, typically lasting several months, and is rigidly divided into three distinct biological phases: Latency, Distraction, and Consolidation.
The Latency Phase begins immediately postoperatively and typically lasts for 7 days. The primary biological purpose of this phase is to allow for the resolution of acute surgical inflammation and the initiation of the early fracture healing cascade. During this week, the hematoma organizes, and crucial mesenchymal stem cells migrate to the corticotomy site. Absolutely no distraction is performed during this period. Attempting to distract the bone before the osteoprogenitor cells have populated the gap will result in a fibrous nonunion. Weight-bearing is typically restricted to heel-touch or partial weight-bearing utilizing a rigid postoperative shoe or CAM boot, allowing the patient to mobilize safely without putting bending stresses on the fixator pins.
The Distraction Phase is the active lengthening period, beginning on postoperative day 8. The standard rate of distraction in the forefoot is 0.75 mm per day. However, to optimize the biological response and minimize soft tissue trauma, this is divided into a rhythm of 0.25 mm performed three times daily (e.g., morning, afternoon, evening). This rate and rhythm are not static; they must be continuously titrated according to radiographic findings and the patient’s clinical tolerance. The patient is seen in the clinic every 10 to 14 days for serial radiographs. The surgeon meticulously evaluates the quality of the regenerate bone (looking for the classic "streaky" intramembranous ossification pattern) and monitors the adjacent MTP joint for any signs of dorsal subluxation. If the regenerate appears lucent or cystic, the distraction rate is slowed. If the regenerate is consolidating too rapidly, the rate is increased. Physical therapy is critical during this phase to maintain ankle and adjacent toe range of motion and to stretch the Achilles tendon, preventing secondary equinus contractures. Distraction is terminated exactly when the predetermined length is achieved, restoring the ideal metatarsal parabola.
The Consolidation Phase begins the moment distraction is halted. The external fixator is locked in its final position and left in place to act as a rigid neutralization device while the soft, fibrous regenerate bone mineralizes into mature, load-bearing cortical bone. This phase is notoriously lengthy. The consolidation index—the time required for the regenerate to fully mineralize—is roughly 30 to 40 days per centimeter of lengthening achieved. Therefore, the consolidation phase typically takes twice as long as the distraction phase. The external fixator is removed in the clinic or minor procedure room only when orthogonal radiographs demonstrate solid, mature, tricortical callus bridging the entire distraction gap. Following fixator removal, the newly formed bone remains vulnerable to bending and torsional forces. The patient is transitioned to a
