Comprehensive Introduction and Patho-Epidemiology
The operative management of lesser ray pathologies demands a profound understanding of forefoot biomechanics, load distribution, and the delicate soft-tissue envelope of the foot. While joint-preserving osteotomies remain the gold standard for most forefoot deformities, specific clinical scenarios—such as the neuropathic foot with a severe bunionette or advanced osteochondrosis of the lesser metatarsal heads—necessitate specialized, and sometimes ablative, surgical interventions. This chapter exhaustively details the indications, biomechanical rationale, and step-by-step surgical execution for two distinct lesser ray procedures: the resection of the fifth metatarsal head for recalcitrant bunionette deformity, and the joint-preserving reconstructive options for Freiberg infraction.
A bunionette, or tailor's bunion, is a painful prominence on the lateral aspect of the fifth metatarsal head. The patho-epidemiology of this deformity varies significantly based on the patient's neurologic status. In the sensate foot, it is often a structural anomaly driven by an increased 4-5 intermetatarsal angle, lateral bowing of the fifth metatarsal shaft, or hypertrophy of the lateral condyle. However, in the neuropathic patient—particularly those with advanced diabetic peripheral neuropathy or Charcot neuroarthropathy—the etiology is driven by intrinsic minus foot deformities, equinus contractures, and profound loss of protective sensation. This leads to repetitive microtrauma, unrecognized focal pressure, and eventual full-thickness ulceration over the lateral eminence. In these compromised hosts, the primary goal shifts from anatomic restoration to rapid ulcer healing and limb salvage, making the non-anatomic fifth metatarsal head resection a vital tool in the surgeon's armamentarium.
Conversely, Freiberg infraction represents a completely different patho-epidemiological entity. First described by A.H. Freiberg in 1914, it is a painful osteochondrosis (avascular necrosis) of the lesser metatarsal heads. It predominantly affects adolescent females in their second decade of life, with a female-to-male ratio reported as high as 5:1. The second metatarsal head is involved in approximately 68% to 82% of cases, followed by the third metatarsal head. The precise etiology remains a subject of academic debate, though it is universally accepted as multifactorial. The prevailing consensus points toward a combination of tenuous vascular supply to the metatarsal head and repetitive microtrauma. During the terminal stance phase of gait, the second metatarsal—which is typically the longest and most rigidly fixed within the cuneiform mortise—experiences immense bending moments and sheer forces. This mechanical overload, coupled with a vulnerable capsular blood supply, precipitates subchondral microfractures, vascular compromise, and subsequent osteochondral collapse.
Understanding the divergent epidemiological profiles of these two pathologies is paramount for the orthopedic surgeon. The bunionette in a neuropathic patient represents an end-stage manifestation of systemic disease requiring aggressive, sometimes ablative, decompression to prevent osteomyelitis and amputation. Freiberg infraction, on the other hand, is a localized mechanical and vascular phenomenon in a typically young, healthy patient, demanding meticulous joint-preserving techniques to maintain forefoot kinematics and prevent premature degenerative joint disease. The synthesis of these concepts forms the foundation for rational surgical decision-making in lesser ray surgery.
Detailed Surgical Anatomy and Biomechanics
The biomechanical integrity of the forefoot relies on an intricate balance between the osseous architecture, the capsuloligamentous constraints, and the dynamic stabilizing forces of the intrinsic and extrinsic musculature. The lateral column of the foot, comprising the cuboid and the fourth and fifth metatarsals, functions as an independent functional unit designed to accommodate uneven terrain during the contact phase of gait. The fifth metatarsal possesses an independent axis of motion, allowing for significant pronation and supination. Its stability is governed by the strong plantar fascia laterally, the peroneus brevis inserting at the base, and the peroneus tertius dorsally. The blood supply to the fifth metatarsal head is derived from the lateral plantar artery and the dorsal metatarsal arteries, which form a rich capsular plexus. When resecting the fifth metatarsal head, the surgeon must be acutely aware of the dorsal cutaneous branch of the sural nerve, which courses dorsolaterally over the distal third of the metatarsal, as iatrogenic injury can lead to debilitating neuromas.
In stark contrast, the central rays (second and third metatarsals) constitute the rigid keystone of the transverse metatarsal arch. The second metatarsal is mortised tightly between the medial, intermediate, and lateral cuneiforms, rendering its base virtually immobile. This rigid fixation, combined with the second metatarsal typically being the longest osseous segment in the forefoot, subjects its distal articular surface to extraordinary ground reaction forces during the heel-off and toe-off phases of the gait cycle. As the foot transitions into terminal stance, the windlass mechanism engages, plantarflexing the metatarsal heads against the ground. The second metatarsal head acts as the primary pivot point, absorbing the highest concentration of stress.
The vascular anatomy of the lesser metatarsal heads is a critical factor in the pathogenesis of Freiberg infraction. The arterial supply is primarily retrograde, originating from the dorsal and plantar metatarsal arteries which arborize into a delicate extraosseous capsular network before penetrating the anatomic neck. There is a well-documented vascular watershed area at the dorsal aspect of the metatarsal head. When the joint is subjected to repetitive forced dorsiflexion—such as in running, dancing, or wearing high-heeled footwear—the dorsal capsule impinges on this watershed zone. This repetitive mechanical ischemia, combined with the immense sheer forces described above, leads to subchondral trabecular failure, localized avascular necrosis, and the classic flattening of the dorsal articular surface seen in Freiberg infraction.
Surgical interventions must respect these biomechanical paradigms. Resection of the fifth metatarsal head fundamentally alters lateral column load sharing. By removing the lateral strut, ground reaction forces are inevitably transferred medially to the fourth and third metatarsal heads. In a sensate foot, this iatrogenic transfer metatarsalgia is poorly tolerated and often more painful than the original bunionette. However, in the neuropathic foot, this pressure redistribution is exactly the desired effect to offload a lateral ulcer. For Freiberg infraction, the biomechanical goal of the dorsal closing wedge osteotomy (Gauthier and Elbay technique) is to rotate the pristine, uninvolved plantar articular cartilage dorsally. This extra-articular correction restores a congruent articular surface to bear the brunt of the forces during the critical toe-off phase, effectively bypassing the necrotic dorsal lesion while preserving the vital plantar plate and collateral ligament attachments.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention in lesser ray pathologies must be guided by a rigorous assessment of the patient's symptoms, neurologic status, vascular perfusion, and functional demands. The indications for fifth metatarsal head resection and the surgical management of Freiberg infraction are highly specific and virtually mutually exclusive in their patient populations. A systematic approach to patient selection is the most critical determinant of surgical success and the avoidance of catastrophic complications.
For the bunionette deformity, primary resection of the fifth metatarsal head is absolutely contraindicated as an initial operative treatment in a healthy, sensate foot. Doing so predictably leads to devastating transfer metatarsalgia, lateral column instability, and severe cosmetic dissatisfaction. Instead, this ablative procedure is strictly reserved for the insensitive foot, specifically patients with profound peripheral neuropathy (e.g., advanced diabetic neuropathy, Charcot neuroarthropathy) who present with recurrent, recalcitrant callus formation or active ulceration directly beneath or lateral to the fifth metatarsal head. It is also indicated in cases of localized osteomyelitis of the fifth metatarsal head where joint preservation is impossible, or as a definitive salvage procedure for failed previous osteotomies with severe degenerative joint disease in low-demand, elderly patients. In the diabetic cohort, the primary metric of success is ulcer healing and amputation prevention, not the radiographic restoration of normal forefoot alignment.
The indications for operative management of Freiberg infraction are dictated by the failure of comprehensive conservative management (metatarsal pads, stiff-soled shoes, offloading boots, NSAIDs) and the specific stage of the disease as defined by the Smillie Classification. Smillie Stage I (fissuring of the epiphysis) and Stage II (central depression of the articular surface) are often managed conservatively, but if recalcitrant, respond exceptionally well to joint debridement and metatarsal head remodeling (cheilectomy). Stage III (central resorption and peripheral projection) and Stage IV (loose body formation and flattening) are the classic indications for the dorsal closing wedge osteotomy, provided the plantar cartilage remains viable. Stage V (end-stage arthrosis with complete joint destruction) requires salvage procedures such as interpositional arthroplasty or, rarely, osteochondral autograft transfer (OATS). Resection of the base of the proximal phalanx or the metatarsal head itself is strongly discouraged in this typically young patient demographic due to the resultant shortening, instability, and transfer lesions.
Absolute contraindications for any elective forefoot surgery include inadequate vascular perfusion (ABI < 0.45, flat toe waveforms), active systemic infection, or profound medical comorbidities precluding safe anesthesia. Relative contraindications include poorly controlled diabetes mellitus (HbA1c > 8.0%), active smoking, and patient non-compliance with postoperative weight-bearing restrictions. The surgeon must weigh the risks of limb-threatening complications in the neuropathic patient against the necessity of removing infected or ulcer-causing bone.
Indications and Contraindications Summary Table
| Pathology | Primary Indications for Surgery | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| 5th Metatarsal Head Resection | Recalcitrant ulceration in a neuropathic foot; Localized osteomyelitis; Salvage of failed osteotomy in low-demand elderly; Severe Charcot deformity with lateral overload. | Healthy, sensate foot with primary bunionette; Inadequate vascular inflow (ABI < 0.45); Active systemic sepsis. | Poorly controlled diabetes (HbA1c > 8%); Patient non-compliance; Active smoking. |
| Freiberg Infraction (Cheilectomy) | Smillie Stages I-III failing >6 months conservative care; Painful mechanical block to dorsiflexion; Hypertrophic synovitis. | Smillie Stage V (end-stage arthrosis); Active joint infection; Asymptomatic radiographic findings. | High-demand athletic season approaching; Severe concurrent metatarsus adductus. |
| Freiberg Infraction (Osteotomy) | Smillie Stages II-IV with viable plantar cartilage; Intact plantar plate; Failure of orthotics/immobilization. | Extensive avascular necrosis involving plantar cartilage; Smillie Stage V; Open physes (pediatric). | Osteopenia precluding rigid K-wire fixation; Heavy smoking history. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of successful lesser ray surgery, beginning with an exhaustive clinical examination. For the patient presenting with a neuropathic bunionette, vascular assessment is mandatory and non-negotiable. Non-invasive vascular studies, including Ankle-Brachial Indices (ABI), Toe-Brachial Indices (TBI), and Doppler waveforms, must confirm adequate perfusion for soft-tissue healing. A TBI greater than 0.45 or absolute toe pressures exceeding 40 mmHg are generally required to ensure a high probability of primary wound healing. Neurologic testing with a 10-gram Semmes-Weinstein monofilament confirms the loss of protective sensation, validating the indication for an ablative rather than reconstructive procedure.
Radiographic evaluation requires standard weight-bearing anteroposterior, lateral, and oblique views of the foot. For the bunionette, the surgeon assesses the 4-5 intermetatarsal angle (normal is less than 8 degrees), the lateral bowing angle of the fifth metatarsal shaft, and the presence of osteolytic changes indicative of osteomyelitis. For Freiberg infraction, plain radiographs are utilized to stage the disease according to the Smillie classification. Early stages may demonstrate subtle joint space widening or subchondral sclerosis, while late stages show classic flattening of the metatarsal head, central depression, and loose body formation.

Advanced imaging is heavily utilized in the modern management of Freiberg infraction. Magnetic Resonance Imaging (MRI) is considered the gold standard for evaluating the metatarsal head in early or ambiguous cases. MRI is highly sensitive for detecting early bone marrow edema (T2/STIR sequences), occult subchondral fractures, and assessing the exact extent of articular cartilage viability before gross radiographic collapse occurs. Intraoperative decision-making—specifically choosing between a simple cheilectomy versus a dorsal closing wedge osteotomy—is heavily reliant on the preoperative MRI confirming that the plantar half of the metatarsal head cartilage remains pristine.
Patient positioning and anesthesia are standardized for both procedures to optimize surgical efficiency and patient safety. The patient is placed in the supine position on a standard operating table. A bump may be placed under the ipsilateral hip to internally rotate the leg, bringing the lateral border of the foot into a directly vertical orientation, which is particularly helpful for the fifth metatarsal approach. A regional anesthetic technique, specifically a popliteal sciatic nerve block combined with a saphenous nerve block, is highly preferred. This provides excellent intraoperative anesthesia and prolonged postoperative analgesia, minimizing the need for systemic opioids. Monitored anesthesia care (MAC) or light general anesthesia is used as an adjunct. A calf or thigh tourniquet is applied and inflated to 250 mmHg to ensure a bloodless surgical field, provided there is no severe peripheral arterial disease or recent history of deep vein thrombosis.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of lesser ray procedures requires meticulous soft-tissue handling and precise osseous resection to avoid debilitating postoperative complications. For the resection of the fifth metatarsal head in the setting of a neuropathic bunionette, the approach must avoid the plantar weight-bearing surface at all costs. A 4 to 5 cm midlateral or dorsolateral longitudinal incision is made over the distal third of the fifth metatarsal. Deepening the incision through the subcutaneous tissues must be performed with blunt dissection to identify and protect the dorsal cutaneous branch of the sural nerve, which is highly variable but generally courses dorsolaterally in this region. Retraction of this nerve is performed with silastic vessel loops to prevent traction neuropraxia.
The periosteum and the lateral capsule of the fifth metatarsophalangeal (MTP) joint are incised longitudinally. The capsule is reflected dorsally and plantarly using a Freer elevator to achieve circumferential exposure of the metatarsal head and the anatomical head-neck junction. Using a sagittal microsaw equipped with a fine-toothed blade, the metatarsal head is resected. The critical technical pearl here is the starting point and trajectory of the osteotomy. The cut must begin exactly 5 mm proximal to the capsular insertion at the head-neck junction. The trajectory must be oblique—directed from distal-lateral to proximal-medial, and slightly plantar-distal to dorsal-proximal. This complex multi-planar beveling ensures that no sharp bony stump remains on the lateral or plantar aspect that could act as a new focal pressure point and precipitate recurrent ulceration.
Following the resection, the wound is copiously irrigated with sterile saline to remove all particulate bone debris, which could otherwise cause a sterile inflammatory response or nidus for infection. The remaining metatarsal stump is aggressively rasped to ensure absolute smoothness. The MTP capsule is then pulled over the resected bone end and closed using 2-0 or 3-0 absorbable sutures (e.g., Vicryl) in a figure-of-eight or purse-string fashion. This capsular interposition serves to pad the bony stump and stabilize the base of the proximal phalanx, preventing severe flail toe deformity. The skin is closed with nonabsorbable sutures (e.g., 3-0 or 4-0 Nylon) using a tension-free, interrupted horizontal mattress technique to maximize skin edge eversion and blood flow.
For the operative management of Freiberg infraction, the surgical approach is dorsal. A 4 cm dorsal longitudinal incision is centered over the affected MTP joint. The extensor digitorum longus and brevis tendons are identified and retracted laterally. A longitudinal dorsal capsulotomy is performed to expose the joint. If performing Joint Débridement and Metatarsal Head Remodeling (Cheilectomy) for Smillie Stages II-III, all loose osteochondral fragments are meticulously excised. The hypertrophic, inflamed synovium is aggressively resected using a combination of sharp dissection and a rongeur. Using a high-speed burr, the peripheral osteophytes and the flattened, necrotic dorsal lip of the metatarsal head are resected back to bleeding, healthy subchondral bone. The goal is to decompress the joint space and restore a smooth gliding surface, accepting that it will be non-spherical.
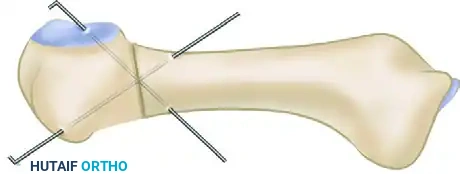
If the preoperative MRI and intraoperative inspection confirm pristine plantar cartilage, the Dorsal Closing Wedge Osteotomy (Gauthier and Elbay Technique) is executed. Following the dorsal exposure and joint debridement, the metatarsal neck is exposed subperiosteally. Using a microsaw, a dorsal-based wedge of bone is resected from the metatarsal neck, immediately proximal to the articular surface. The plantar cortex is left intact to act as a hinge. The osteotomy is then closed by forcefully dorsiflexing the metatarsal head, which rotates the healthy plantar cartilage dorsally into articulation with the proximal phalanx.

Rigid fixation of this osteotomy is paramount. While micro-fragment plates or compression screws can be utilized, cross-pinning with two 0.045-inch or 0.062-inch Kirschner wires remains the most reliable, low-profile, and cost-effective method. The K-wires are driven from the dorsal-distal aspect of the metatarsal head, across the osteotomy site, and into the proximal metatarsal diaphysis, ensuring bicortical purchase. The pins are typically cut outside the skin and capped for easy removal in the clinic setting.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, operative interventions on the lesser rays carry a distinct profile of potential complications. The surgeon must be fully prepared to manage these adverse events, which range from minor wound healing delays to catastrophic biomechanical failures requiring complex salvage reconstruction. Thorough preoperative patient counseling regarding these risks is a mandatory component of the informed consent process.
In the context of fifth metatarsal head resection, the most devastating complication in a sensate foot is iatrogenic transfer metatarsalgia, occurring in up to 80% of patients if this procedure is inappropriately selected for a primary bunionette. The loss of lateral column support forces the fourth and third metatarsals to bear unphysiologic loads, leading to intractable plantar pain, adventitial bursitis, and secondary stress fractures. In the appropriately selected neuropathic patient, transfer ulceration to the adjacent metatarsal heads occurs in approximately 15% to 20% of cases. Recurrent ulceration at the surgical site can occur if the metatarsal stump is not adequately beveled or if the patient is non-compliant with postoperative offloading footwear. Sural nerve entrapment or neuroma formation occurs in 2% to 5% of cases and presents with sharp, shooting pain along the lateral border of the foot.
Complications following the surgical management of Freiberg infraction are largely related to stiffness, hardware irritation, and osteotomy nonunion. Following joint debridement and cheilectomy, virtually all patients will experience some degree of permanent restriction in MTP joint range of motion. This is an expected outcome rather than a true complication, but failure to set this expectation preoperatively leads to significant patient dissatisfaction. Following a dorsal closing wedge osteotomy, delayed union or nonunion occurs in approximately 3% to 5% of cases, often related to thermal necrosis from the saw blade or inadequate rigid fixation. Pin tract infections from percutaneous K-wires are relatively common (up to 10%) but usually resolve rapidly with oral antibiotics and pin removal. Progression of avascular necrosis and secondary joint collapse can occur if the vascular insult continues or if the osteotomy fails to adequately offload the necrotic segment.
Salvage management requires a stepwise, logical approach. For transfer metatarsalgia or transfer ulceration following fifth metatarsal head resection, initial management consists of aggressive orthotic modifications, utilizing custom-molded total contact insoles with specific accommodations and metatarsal offloading pads. If conservative measures fail, surgical salvage may require shortening osteotomies (e.g., Weil osteotomies) of the adjacent overloaded lesser metatarsals to restore a harmonious metatarsal parabola. For a painful nonunion of a Freiberg osteotomy, revision surgery with autologous bone grafting and rigid internal fixation with a dorsal locking plate is indicated. In cases of end-stage joint destruction following failed Freiberg reconstruction, salvage options are limited. Interpositional arthroplasty using an extensor digitorum brevis tendon roll or a synthetic spacer can be attempted, though resection arthroplasty or amputation of the toe may be the ultimate final common pathway in severe, recalcitrant cases.
Complications and Salvage Strategies Table
| Complication | Estimated Incidence | Primary Etiology | Salvage Management Strategy |
|---|---|---|---|
| Transfer Metatarsalgia / Ulceration | 15-20% (Neuropathic) / >80% (Sensate) | Loss of lateral column support; Altered forefoot parabola. | Custom accommodative orthotics; Weil osteotomies of adjacent metatarsals. |
| Recurrent Lateral Ulceration | 5-10% | Inadequate bony beveling; Sharp plantar-lateral stump; Non-compliance. | Revision osseous resection; Aggressive rasping; Total contact casting. |
| Sural Neuroma | 2-5% | Iatrogenic transection or traction injury during lateral approach. | Gabapentinoids; Corticosteroid injections; Surgical excision and burying into muscle. |
| MTP Joint Stiffness (Freiberg) | >90% (Expected) | Capsular scarring; Altered joint kinematics post-cheilectomy. | Aggressive physical therapy; Preoperative patient counseling (critical). |
| Osteotomy Nonunion (Freiberg) | 3-5% | Thermal necrosis; Inadequate K-wire fixation; Early weight-bearing. | Prolonged immobilization; Bone stimulator; Revision with bone graft and plating. |
| Pin Tract Infection | 5-10% | Percutaneous K-wire colonization. | Oral antibiotics (e.g., Cephalexin); Early K-wire removal if union is progressing. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol must be specifically tailored to the procedure performed, the patient's biologic healing capacity, and their underlying neurologic status. A rigid, phased approach ensures the protection of the surgical repair while mitigating the risks of deep vein thrombosis, severe disuse osteopenia, and complex regional pain syndrome. The surgeon must maintain strict oversight during the transition between these phases.
Phase 1: Acute Healing and Protection (0 to 2 Weeks)
Immediately following fifth metatarsal head resection in a neuropathic patient, the foot is placed in a bulky, soft compressive dressing. Weight-bearing to tolerance in a rigid, wooden-soled postoperative shoe or a controlled ankle motion (CAM) boot is generally permitted immediately, as there is no osteotomy requiring rigid union. However, strict elevation of the extremity above the level of the heart is strongly encouraged for the first 48 to 72 hours to minimize dependent edema and protect the vascularity of the incision. For patients who underwent a Freiberg osteotomy, the protocol is decidedly more conservative. The foot is immobilized in a well-padded posterior splint or CAM boot, and the patient is restricted to strict non-weight-bearing or heel-touch weight-bearing with crutches to prevent catastrophic displacement of the K-wires and osteotomy. Suture removal for both procedures typically occurs between 14 to 21 days, contingent upon absolute resolution of wound drainage and intact epidermal healing.
Phase 2: Transition and Osseous Consolidation (2 to 6 Weeks)
During this phase, the neuropathic patient following a fifth metatarsal resection continues to mobilize in a rigid postoperative shoe. The focus shifts to monitoring the wound for delayed breakdown and ensuring the patient does not return to standard footwear prematurely. For the Freiberg osteotomy patient, this is the critical period of osseous consolidation. The patient remains in the CAM boot, and weight-bearing is gradually advanced from heel-touch to flat-foot weight-bearing as tolerated, provided serial radiographs at 3 and 6 weeks demonstrate progressive callus formation across the osteotomy site. If percutaneous K-wires were utilized for fixation, they are typically removed in the outpatient clinic at the 4 to 6-week mark, once clinical and radiographic union is confirmed. Active and passive range of motion exercises of the MTP joint are initiated immediately following pin removal to combat capsular fibrosis.
Phase 3: Functional Restoration and Long-Term Offloading (6 to 12+ Weeks)
At the 6-week juncture, assuming uncomplicated healing, patients are transitioned out of the CAM boot or surgical shoe. For the Freiberg patient, transition into a stiff-soled athletic shoe with a wide toe box is recommended. Physical therapy is aggressively escalated, focusing on intrinsic foot muscle strengthening, intrinsic stretching, and restoration of the windlass mechanism. Metatarsal bars or custom orthotic pads with a specific relief cutout for the affected metatarsal head should be utilized for 3 to 6 months postoperatively to continuously offload the healing bone and maturing cartilage. For the neuropathic patient following fifth metatarsal resection, the long-term protocol dictates a permanent lifestyle modification. The patient is transitioned to a wide, extra-depth diabetic shoe with a custom-molded plastazote accommodative orthotic. Lifelong adherence to diabetic foot care protocols, daily skin inspections, and routine podiatric or orthopedic follow-up is mandatory to prevent contralateral breakdown or transfer lesions.
Summary of Landmark Literature and Clinical Guidelines
The evolution of operative management for lesser ray pathologies is deeply rooted in a rich history of orthopedic literature and progressive clinical guidelines. Understanding this historical context provides the modern surgeon with the rationale behind current gold-standard treatments and highlights the iterative process of surgical innovation.
The foundational understanding of lesser metatarsal osteochondrosis began with A.H. Freiberg's seminal publication in 1914. Freiberg initially reported a series of six cases involving the second metatarsal head, noting that three of the patients had a distinct history of a single significant traumatic event. He hypothesized that the disorder was a direct secondary consequence of acute trauma, leading to structural collapse. Shortly thereafter, in 1917, Campbell reported the identical condition occurring in the third metatarsal head. Over the subsequent decades, as larger epidemiological series were published, the theory evolved from acute trauma to the modern consensus of repetitive microtrauma superimposed on a tenuous vascular watershed zone.
The classification system proposed by Smillie in 1957 remains the universally accepted framework for staging Freiberg infraction and directly guides surgical decision-making. Smillie's original work also advocated for elevation of the depressed fragment and cancellous bone grafting, a technique that laid the groundwork for modern joint-preserving philosophies, though it has largely
