Comprehensive Management of Ipsilateral Femoral Neck and Shaft Fractures
Key Takeaway
Ipsilateral femoral neck and shaft fractures occur in 1% to 9% of femoral shaft injuries. Because missed femoral neck fractures lead to catastrophic complications, a dedicated pelvic CT is mandatory for all blunt trauma femur fractures. Surgical priority dictates stabilizing the femoral neck first to ensure anatomic reduction, followed by shaft fixation. Postoperative protocols strictly limit patients to touch-down weight bearing for 10 to 12 weeks to optimize union.
Comprehensive Introduction and Patho-Epidemiology
Ipsilateral femoral neck fractures occur in association with femoral shaft fractures in approximately 1% to 9% of all femoral shaft fracture presentations. These complex, high-energy injuries present a formidable, multifaceted challenge to the orthopedic trauma surgeon. They are classically the result of severe blunt force trauma, most frequently encountered in motor vehicle collisions, motorcycle accidents, or falls from a significant height. The pathomechanics typically involve an immense axial load applied to a flexed and abducted thigh—such as a knee striking a dashboard during a high-speed deceleration event. This force propagates longitudinally through the femoral shaft, resulting in a diaphyseal fracture, and subsequently transmits residual kinetic energy proximally into the femoral neck, causing a concomitant cervical fracture.
The bimodal distribution of femoral fractures generally dictates that high-energy trauma affects predominantly young, male patients, whereas low-energy falls affect the elderly osteoporotic population. However, the ipsilateral neck and shaft combination is almost exclusively a high-energy phenomenon, meaning the patient cohort is typically young, physiologically robust, but frequently polytraumatized. These patients often present with concomitant life-threatening injuries, including traumatic brain injuries, blunt thoracic trauma, and solid organ visceral injuries, necessitating a multidisciplinary approach governed by Advanced Trauma Life Support (ATLS) protocols. The systemic inflammatory response syndrome (SIRS) and the "second hit" phenomenon must be carefully weighed when determining the timing of definitive fixation versus damage control orthopedics (DCO).
The timing of the diagnosis of the femoral neck fracture has a dramatic, often irreversible impact on patient outcomes. Historically, up to 30% of associated femoral neck fractures were missed at initial presentation, a catastrophic oversight that underscores the deceptive nature of this injury pattern. The grossly deformed, shortened, and externally rotated thigh characteristic of a mid-shaft femur fracture acts as a powerful "distracting injury." This dramatic clinical presentation invariably draws the trauma team's focus away from the proximal femur. Furthermore, the femoral neck fracture in this specific biomechanical setting is frequently nondisplaced or minimally displaced at the time of injury. It is often vertically oriented, conforming to a Pauwels type III shear pattern, which is notoriously difficult to visualize on standard, often suboptimal, trauma bay anteroposterior (AP) plain films.
Late diagnosis of concomitant femoral neck fractures invariably leads to disastrous complications. If a nondisplaced femoral neck fracture goes unrecognized and the femoral shaft is subsequently treated with an antegrade intramedullary nail, the rotational and translational forces exerted during reaming and nail insertion will almost certainly displace the cervical fracture. This iatrogenic displacement significantly compromises the delicate retinacular blood supply to the femoral head, astronomically increasing the risk of avascular necrosis (AVN), nonunion, varus collapse, and the tragic necessity for early total hip arthroplasty in a young patient. Consequently, a remarkably high index of suspicion, a rigorous, standardized diagnostic imaging protocol, and an unwavering commitment to the "neck first" fixation philosophy are absolute prerequisites for the successful management of these perilous injuries.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the surgical anatomy and biomechanics of the proximal femur is non-negotiable when addressing ipsilateral neck and shaft fractures. The vascular anatomy of the femoral head is notoriously precarious and unforgiving. The primary blood supply to the adult femoral head is derived from the medial femoral circumflex artery (MFCA), specifically its deep branch. The MFCA originates from the profunda femoris artery, courses posteriorly between the iliopsoas and pectineus, and passes anterior to the obturator externus and posterior to the obturator internus. It then gives rise to the critical posterosuperior and posteroinferior retinacular vessels, which perforate the joint capsule at the intertrochanteric line and travel proximally along the femoral neck to perfuse the capital epiphysis.
The lateral femoral circumflex artery (LFCA) provides a much smaller, anterior contribution via the anterior retinacular vessels, while the artery of the ligamentum teres (a branch of the obturator artery) provides a negligible supply in the adult. Displacement of a femoral neck fracture, or iatrogenic manipulation during shaft nailing, stretches, kinks, or completely ruptures these delicate retinacular vessels. Because the femoral neck lacks a cambium layer of periosteum, it heals almost entirely through primary endosteal bone formation, making it highly dependent on this fragile vascular network and rigid mechanical stability. Any disruption of this blood supply precipitates osteocyte death, leading to avascular necrosis and subsequent subchondral collapse.
Biomechanically, the proximal femur is subjected to massive forces during normal physiological loading. The femoral neck acts as a cantilever, subjected to bending moments that create high compressive forces on the inferior (calcar) aspect and high tensile forces on the superior aspect. The trabecular architecture of the proximal femur perfectly reflects these stress patterns, with the principal compressive group extending from the calcar to the superior femoral head, and the principal tensile group arcing from the lateral cortex to the inferior head. The intersection of these trabecular lines forms Ward's triangle, a central area of relative structural weakness.
In the setting of an ipsilateral shaft fracture, the normal biomechanical load-sharing of the femur is entirely disrupted. When the surgeon applies traction to reduce the shaft, or introduces a reamer into the medullary canal, immense torsional and translational forces are generated. If the femoral neck fracture is not rigidly stabilized prior to these maneuvers, the neck will inevitably displace. Furthermore, the typical Pauwels type III (vertical shear) orientation of the femoral neck fracture in these cases means that the fracture plane is subjected to maximal shear forces and minimal compressive forces, creating a highly unstable mechanical environment that demands meticulous, biomechanically sound fixation constructs, such as a compression hip screw or a perfectly executed inverted triangle of cannulated screws.
Exhaustive Indications and Contraindications
The management of ipsilateral femoral neck and shaft fractures requires highly nuanced decision-making. The primary indication for operative intervention is the presence of the fractures themselves, as non-operative management is universally condemned due to the certainty of profound morbidity, nonunion, and severe functional deficit. However, the timing and type of surgical intervention are dictated by the patient's overall physiologic status, the degree of soft tissue injury, and the specific fracture morphology.
In the polytraumatized patient exhibiting signs of the lethal triad (coagulopathy, hypothermia, acidosis), early total care (ETC) is strictly contraindicated. Instead, damage control orthopedics (DCO) must be instituted. In this scenario, the femoral shaft is rapidly stabilized with a spanning external fixator to control hemorrhage and reduce systemic inflammatory burden. Crucially, even in a DCO setting, a displaced femoral neck fracture must be anatomically reduced and provisionally or definitively stabilized (often with percutaneous cannulated screws) to minimize the risk of irreversible avascular necrosis, as the hip joint capsule tamponade and vascular kinking must be relieved emergently.
The choice of definitive implant construct—single implant (e.g., reconstruction nail) versus dual implant (e.g., cannulated screws for the neck and a retrograde nail for the shaft)—is a subject of intense academic debate. Dual implant constructs are generally favored as they allow for independent, optimized fixation of both fractures. Single implant constructs are technically demanding; achieving the perfect starting point for the nail to anatomically reduce the shaft while simultaneously ensuring perfect trajectory for the cephalomedullary screws into the femoral head often forces a compromise, leading to malreduction of the neck.
| Variable | Indications | Contraindications |
|---|---|---|
| Damage Control Orthopedics (DCO) | Polytrauma with hemodynamic instability, severe head injury (GCS < 8), blunt chest trauma with poor oxygenation, lethal triad. | Hemodynamically stable patient, isolated extremity trauma, normal acid-base status. |
| Early Total Care (ETC) | Hemodynamically stable, adequately resuscitated patient, isolated femur fracture, absence of severe traumatic brain injury. | Unresuscitated shock, coagulopathy, severe hypothermia, evolving pulmonary contusions. |
| Dual Implant Construct (Screws + Retrograde Nail) | Standard of care for most ipsilateral fractures. Allows independent optimization of neck and shaft reduction. | Severe intra-articular distal femur fractures precluding retrograde nail insertion. |
| Single Implant Construct (Reconstruction Nail) | Nondisplaced neck fractures where perfect starting point can be achieved without compromising neck stability. | Displaced neck fractures, basicervical fractures, inability to achieve anatomic neck reduction prior to reaming. |
| Open Reduction of Femoral Neck | Inability to achieve closed anatomic reduction of the femoral neck, irreducible fracture-dislocations. | Severe soft tissue compromise anteriorly (e.g., Morel-Lavallée lesion over the surgical approach). |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the absolute cornerstone of successful outcomes in these complex dual-level fractures. The standard radiographic evaluation of femoral fractures must be exhaustive and uncompromising. It must include high-quality anteroposterior (AP) and lateral views of the entire femur, an AP view of the pelvis, and a dedicated lateral view of the affected hip. Because a high-quality cross-table lateral image of the affected hip can be exceptionally difficult to obtain in a patient with a grossly unstable, painful femoral shaft fracture, a pelvic CT scan is mandatory for every patient who sustains a femoral fracture caused by high-energy blunt trauma.
The pelvic CT scan should never be limited to standard axial images. It must include high-resolution coronal and sagittal reconstructed images to accurately assess the trabecular lines of the femoral neck and head. These reformats are critical for identifying occult, nondisplaced cortical breaches that signify a hairline cervical fracture. Digital templating must be performed for both fracture sites. The surgeon must template the size, length, and trajectory of the femoral neck fixation (cannulated screws or sliding hip screw) and ensure that this hardware will not physically block or interfere with the trajectory of the chosen femoral shaft implant (antegrade or retrograde intramedullary nail).
Patient positioning dictates the flow and ease of the entire surgical procedure. Reduction and fixation are optimally performed with the patient positioned supine on a radiolucent fracture table. This specialized setup allows for the application of controlled, sustained skeletal traction and facilitates the highest quality orthogonal fluoroscopic imaging of the proximal femur without interference from the contralateral leg. The patient's torso must be carefully padded and secured to the perineal post to prevent sheer injury to the pudendal nerve.
The contralateral leg is typically placed in a hemilithotomy position using a well-padded gynecological stirrup, or scissored posteriorly, dropping it out of the fluoroscopic field of view for the cross-table lateral projection. The entire affected limb, from the iliac crest to the toes, should be prepped and draped into the sterile field. This extensile draping allows the surgeon the flexibility to transition from a closed percutaneous technique to an open anterior (Smith-Petersen) or anterolateral (Watson-Jones) approach if closed reduction of the femoral neck fails, and allows access to the knee for retrograde nailing.
Step-by-Step Surgical Approach and Fixation Technique
Management of the Displaced Femoral Neck
When an ipsilateral femoral neck and shaft fracture is diagnosed preoperatively, the fundamental, unyielding principle of surgical management is clear: treatment of the femoral neck fracture is the absolute priority, followed by treatment of the femoral shaft. If the femoral neck is displaced, anatomic reduction is non-negotiable. Closed reduction should be attempted gently using traction, internal rotation, and slight abduction; however, forceful or repeated closed reduction attempts are strictly contraindicated as they further damage the remaining retinacular blood supply. If anatomic alignment is not achieved on both AP and lateral fluoroscopic views, open reduction is mandatory.
Open reduction is typically performed through either a Smith-Petersen (anterior) or Watson-Jones (anterolateral) approach. The Smith-Petersen approach utilizes the internervous plane between the sartorius (femoral nerve) and tensor fasciae latae (superior gluteal nerve) superficially, and the rectus femoris (femoral nerve) and gluteus medius (superior gluteal nerve) deeply. This provides excellent direct visualization of the anterior femoral neck and allows for direct manipulation of the fracture fragments using a bone hook or Schanz pin. The Watson-Jones approach utilizes the internervous plane between the tensor fasciae latae and the gluteus medius, offering excellent access for both reduction and subsequent lateral hardware placement.
Once anatomic reduction is achieved under direct vision, it is provisionally held with multiple smooth Kirschner wires placed anteriorly or superiorly to avoid interfering with the definitive hardware trajectory. Definitive stabilization is then obtained with either multiple cannulated screws or a compression hip screw (CHS). For a Pauwels type III vertical shear fracture, a CHS with an additional derotational screw provides superior biomechanical stability against vertical shear forces compared to parallel cannulated screws.

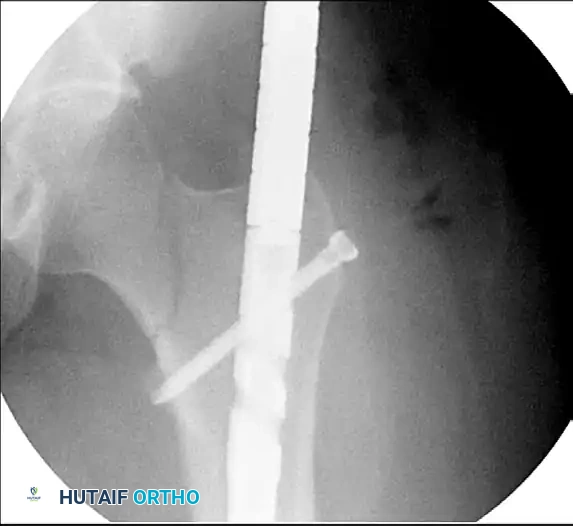
Figure 55-62A: Preoperative radiograph demonstrating a displaced ipsilateral femoral neck and shaft fracture.
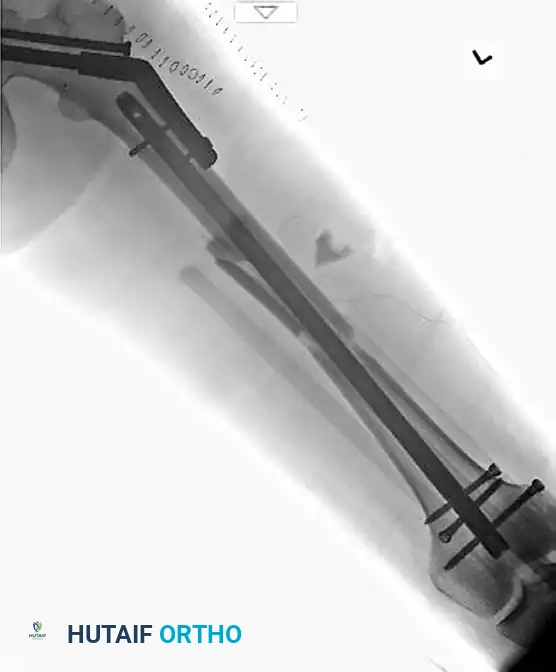
Figure 55-62B: Postoperative radiograph demonstrating fixation of the femoral neck with cannulated screws and the shaft with a retrograde intramedullary nail.

Figure 55-62C: Lateral postoperative radiograph confirming anatomic alignment and appropriate hardware placement.
Management of the Nondisplaced Femoral Neck
If the femoral neck is strictly nondisplaced on high-resolution CT imaging, it can be stabilized in situ. Fixation options include three 6.5mm or 7.3mm cannulated screws placed in an inverted triangle configuration. The inferior screw must rest directly on the dense bone of the calcar to provide optimal biomechanical support, while the posterior and anterior screws provide rotational stability. This technique is tissue-sparing and minimizes blood loss. Alternatively, a Compression Hip Screw (CHS) can be utilized, providing superior biomechanical stability, particularly for basicervical or high-shear angle fractures, though it requires a larger lateral exposure and greater bone removal for the lag screw.
Surgical Warning: A nondisplaced femoral neck fracture with an associated femoral shaft fracture can theoretically be treated with a single device, such as an antegrade reconstruction nail. However, this is exceptionally technically difficult. Achieving the perfect piriformis or trochanteric starting point for the nail while simultaneously perfectly aligning the cephalomedullary screws into the center of the femoral head often leads to a compromise that causes malreduction of the neck. The potential complications (varus collapse, nonunion) are significantly greater with single-implant constructs compared to dual-implant constructs (e.g., cannulated screws for the neck and a retrograde nail for the shaft).
Management of the Femoral Shaft
Once the femoral neck is rigidly stabilized, attention is turned to the femoral shaft. Retrograde intramedullary nailing is the preferred technique in the dual-implant paradigm. A trans-patellar tendon or medial parapatellar approach is utilized to access the intercondylar notch. The starting point is critical: exactly in the center of the intercondylar notch on the AP view, and just anterior to Blumensaat's line on the lateral view.
Retrograde nailing is advantageous because it avoids the proximal femur entirely, preventing any crowding or hardware conflict with the newly placed femoral neck screws. It also eliminates the need to manipulate the proximal femur to find a starting point, thereby protecting the delicate femoral neck fixation from iatrogenic stress. The canal is reamed sequentially, and an appropriately sized retrograde nail is inserted and locked distally and proximally. The proximal locking screws must be placed carefully to avoid the femoral neck hardware, a step that requires meticulous fluoroscopic visualization.
Complex Proximal Femoral Trauma: Associated Head and Acetabular Fractures
In the most severe high-energy trauma cases, ipsilateral femoral fractures may be complicated by concomitant injuries to the femoral head and acetabulum, such as a Pipkin IV fracture-dislocation. These represent the zenith of orthopedic trauma complexity and require highly specialized, multidisciplinary management.
Surgical dislocation of the hip (Ganz approach) is often required to adequately address these complex intra-articular injuries. This approach involves a trochanteric flip osteotomy, allowing for a 360-degree view of the femoral head and acetabulum while meticulously protecting the medial femoral circumflex artery by keeping the external rotators intact. This exposure permits anatomic reduction of the posterior wall of the acetabulum, debridement of intra-articular fragments, and precise fixation of the femoral head fracture.

Figure 55-61A: Preoperative radiograph demonstrating a complex Pipkin IV fracture (posterior wall acetabular fracture with an associated femoral head fracture).

Figure 55-61B: Postoperative radiograph following surgical dislocation of the hip, open reduction and internal fixation of the posterior wall acetabular fracture, and débridement of the infrafoveal femoral head fracture.
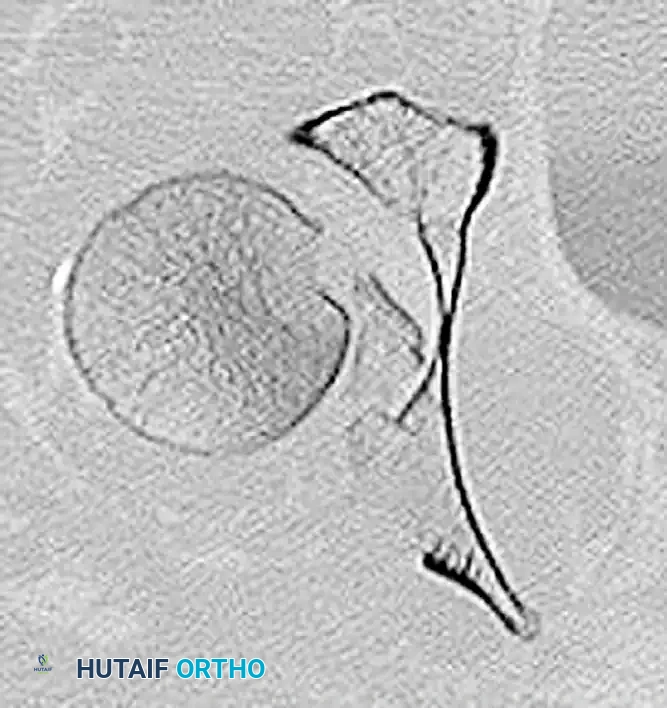
Figure 55-61C: Postoperative axial CT scan confirming concentric reduction and hardware placement.

Figure 55-61D: Postoperative coronal CT scan demonstrating restoration of the articular congruity.

Figure 55-61E: Postoperative AP pelvic radiograph showing the final construct.
Complications, Incidence Rates, and Salvage Management
The complication profile for ipsilateral femoral neck and shaft fractures is formidable, driven primarily by the high-energy mechanism and the precarious vascularity of the proximal femur. Avascular necrosis (AVN) of the femoral head remains the most devastating complication. Historically, rates of AVN approached 20-30%, largely due to missed diagnoses and delayed fixation. With modern CT protocols and immediate, rigid internal fixation, the rate of AVN has been reduced to approximately 3-5%, though it remains significantly higher if the initial fracture was severely displaced or if diagnosis was delayed beyond 24 hours.
Nonunion of the femoral neck occurs in 5-10% of cases and is heavily influenced by the quality of the initial reduction and the biomechanical stability of the construct. Varus collapse is a frequent precursor to nonunion, particularly in Pauwels type III fractures treated with inadequate fixation (e.g., poorly spaced cannulated screws). Femoral shaft nonunion is less common (1-3%) but can occur due to excessive stripping during open reduction or inadequate mechanical stabilization. Infection rates mirror those of other high-energy long bone fractures, ranging from 1-2% for closed injuries to significantly higher for open fractures.
Intraoperative discovery of a missed neck fracture is a highly stressful scenario that demands immediate, calculated salvage techniques. Despite rigorous preoperative imaging, occult fractures can still be missed. To avoid leaving the operating room with an undiagnosed femoral neck fracture, a strict intraoperative fluoroscopic protocol must be adhered to. After the placement of an intramedullary nail for the femoral shaft, the surgeon must obtain live fluoroscopic images of the hip through a full range of motion, and a standard AP view of the pelvis with the extremities in internal rotation.
If a femoral neck fracture is discovered after the placement of an antegrade femoral shaft intramedullary nail, treatment is dictated by the specific design of the implanted nail system.
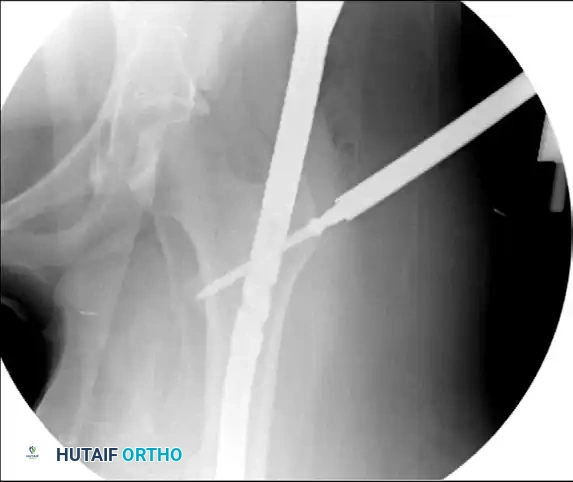
Figure 55-63A: Preoperative radiograph of a femoral shaft fracture. The subtle nondisplaced femoral neck fracture was initially missed.
Figure 55-63B: Intraoperative fluoroscopic view after placement of an antegrade intramedullary nail. Note the appearance of the proximal femur.

Figure 55-63C: Intraoperative fluoroscopic view after range of motion of the hip under live fluoroscopy reveals the previously occult femoral neck fracture.
Salvage Techniques for Missed Fractures
Scenario A: The Nail System Has a Reconstruction Option
If the fracture is nondisplaced and the implanted nail system features a reconstruction option (holes designed for cephalomedullary screws), the surgeon can convert the construct. The standard proximal transverse interlocking screw is removed. The nail position must often be adjusted (tapped cephalad or caudad) to perfectly align the reconstruction holes with the center of the femoral neck and head. Critical Step: If this adjustment is necessary, two provisional guide pins must be placed anteriorly across the femoral neck before moving the nail to prevent iatrogenic displacement of the fracture during nail manipulation. Once aligned, two cephalomedullary screws are placed into the femoral head.

Figure 55-63D: Intraoperative fluoroscopic view after removal of the standard proximal interlocking screw, adjustment of the nail, and successful placement of reconstruction screws.
Scenario B: The Nail System Lacks a Reconstruction Option
If the nailing system does not allow for a reconstruction option, the surgeon must utilize a "miss-a-nail" technique. Multiple cannulated screws (typically 6.5mm or 5.0mm) are carefully placed around the intramedullary nail. This requires precise fluoroscopic guidance to ensure the screws pass anterior or posterior to the nail without compromising the fixation of either the neck or the shaft. This is technically demanding and provides suboptimal biomechanical stability, but avoids the morbidity of removing the entire antegrade nail.
| Complication | Incidence Rate | Salvage Management / Treatment Strategy |
|---|---|---|
| Avascular Necrosis (AVN) | 3 - 5% (Modern cohorts); up to 30% historically. | Young patients: Core decompression, vascularized fibular graft, or proximal femoral osteotomy. Older patients: Total Hip Arthroplasty (THA). |
| Femoral Neck Nonunion | 5 - 10% | Valgus intertrochanteric osteotomy to convert shear forces to compressive forces; revision internal fixation with bone grafting; THA if AVN is also present. |
| Varus Collapse | 5 - 15% (Higher in Pauwels III) | Early revision to a more stable construct (e.g., replacing screws with a CHS); Valgus osteotomy. |
| Femoral Shaft Nonunion | 1 - 3% | Exchange nailing (reaming to a larger diameter and inserting a larger nail); dynamization; augmentation with plating and bone graft. |
| Missed Neck Fracture (Intra-op) | Variable (depends on protocol adherence) | "Miss-a-nail" technique with cannulated screws around the existing shaft nail; Conversion to a reconstruction nail construct. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol for patients with ipsilateral femoral neck and shaft fractures is significantly more conservative and protracted than for isolated femoral shaft fractures. The overarching principle is that the femoral neck fracture represents the "weak link" in the biomechanical construct. It is highly susceptible to varus collapse and nonunion under cyclic loading, demanding strict adherence to weight-bearing precautions to protect the delicate endosteal healing process.
Phase I: Immediate Post-Operative (Weeks 0-6)
During the initial six weeks, the primary goals are protection of the fixation, prevention of thromboembolic events, and restoration of basic joint mobility. Patients are strictly limited to touch-down weight bearing (TDWB) or flat-foot weight bearing (maximum 10-15 lbs of pressure) on the affected extremity. This allows for balance assistance without imparting significant axial or shear loads across the healing femoral neck. Early active and active-assisted range of motion of the hip and knee is highly encouraged to prevent arthrofibrosis, promote cartilage nutrition, and reduce edema, provided the fracture fixation was deemed rigidly stable intraoperatively. Given the high-energy nature of the trauma, the prolonged period of restricted weight bearing, and the inherent hypercoagulability of major orthopedic trauma, aggressive chemical (e.g., Low Molecular Weight Heparin) and mechanical DVT prophylaxis is mandatory per institutional trauma guidelines.
Phase II: Intermediate Healing (Weeks 6-12)
At the 6-week mark, comprehensive radiographic evaluation is performed. If there is evidence of early callus formation at the shaft and maintenance of anatomic alignment at the neck without signs of hardware back-out or varus collapse, weight-
