Retrograde Femoral Nailing: An Intraoperative Masterclass for Fellows

Key Takeaway
Welcome to the OR, fellows. Today, we're performing a retrograde femoral nailing. This masterclass will cover comprehensive anatomy, meticulous preoperative planning, and a granular, real-time breakdown of the surgical execution, from incision to hardware application. We'll emphasize critical pearls, potential pitfalls, and strategies for intraoperative salvage, ensuring a deep understanding of this vital procedure.
Comprehensive Introduction and Patho-Epidemiology
Welcome, fellows, to the operating theater. Today, we are embarking on a comprehensive exploration of a highly versatile and indispensable procedure in modern orthopedic traumatology: retrograde intramedullary nailing of the femur. This technique, defined as any femoral nailing procedure utilizing a distal entry point from the condyles or through an intercondylar, intra-articular starting trajectory, has revolutionized our approach to complex lower extremity trauma. Originally conceptualized as a salvage procedure or a niche technique for specific distal third fractures, retrograde nailing has evolved into a primary, frontline intervention for a vast array of femoral shaft and supracondylar fractures. Its utility is particularly pronounced in the polytraumatized patient, where physiological optimization and damage control orthopedics dictate our surgical decision-making.
Our journey begins long before the scalpel meets the skin. Every trauma patient, particularly those presenting with suspected high-energy femoral fractures, must undergo a rigorous, systematic Advanced Trauma Life Support (ATLS) evaluation. This is a non-negotiable tenet of trauma surgery; our primary, overriding goal is to identify and resuscitate any associated life-threatening hemorrhagic, thoracic, or neurosurgical injuries before we even consider definitive stabilization of the appendicular skeleton. A femoral shaft fracture is a massive physiological insult, capable of sequestering up to 1,500 milliliters of blood within the thigh compartment. Consequently, the orthopedic surgeon must work in seamless tandem with the general trauma surgery and anesthesia teams to ensure the patient is adequately resuscitated and hemodynamically stable for surgical intervention.
On presentation, a patient with a femoral shaft fracture typically exhibits obvious, excruciating pain, gross deformity of the thigh, and an inability to bear weight. However, as aspiring master surgeons, you must never let these overt, dramatic signs lull you into diagnostic complacency. In a morbidly obese patient, or in a patient with severe concomitant traumatic brain injury, these classic physical findings may be significantly obscured or entirely absent, demanding a heightened index of suspicion. Furthermore, while we typically associate these fractures with high-energy mechanisms such as motor vehicle collisions or falls from significant heights, we must also recognize a bimodal epidemiological distribution. Low-energy mechanisms, such as simple ground-level falls, can easily precipitate catastrophic femoral shaft or distal femur fractures in our geriatric population, particularly in those with severe osteoporosis, chronic bisphosphonate use leading to atypical femur fractures, or metastatic bone disease.
A meticulous, exhaustive examination of the fractured extremity is absolutely paramount. We must actively and circumferentially search for any open wounds, paying particular attention to the posterior aspect of the thigh and the gluteal fold, which can be easily overlooked in the supine trauma patient. Even seemingly innocuous skin abrasions or puncture wounds require careful, sterile assessment to determine if they communicate with the fracture hematoma, thereby reclassifying the injury as an open fracture requiring emergent debridement and systemic antibiotic prophylaxis. While swelling is a ubiquitous finding, we must remain hyper-vigilant for the development of compartment syndrome of the thigh. Though statistically rare due to the large volume of the thigh compartments, it is a devastating, limb-threatening complication that necessitates immediate, definitive surgical fasciotomy.
Finally, we must internalize the reality that a high-energy femoral shaft fracture is rarely an isolated event; it is a glaring marker of massive kinetic energy transfer. Studies have consistently demonstrated that up to 38% of trauma patients with a femoral shaft fracture harbor additional, significant injuries. The literature indicates high incidences of concomitant musculoskeletal injuries (93%), thoracic trauma (62%), traumatic brain injuries (59%), solid organ abdominal injuries (35%), and maxillofacial trauma (16%). A thorough, meticulously documented neurologic and vascular examination is absolutely critical. While isolated femoral nerve damage is exceedingly rare, sciatic nerve neurapraxia or axonotmesis can occur, particularly with significant posterior fracture displacement or prolonged, excessive pre-hospital traction. Furthermore, associated ligamentous injuries of the knee—the so-called "floating hinge"—are incredibly common but notoriously difficult to assess accurately in the acute setting due to profound pain, guarding, and hemarthrosis. Therefore, a comprehensive ligamentous knee examination must be systematically repeated and documented after definitive intramedullary stabilization of the femoral fracture.
Detailed Surgical Anatomy and Biomechanics
To master retrograde femoral nailing, one must possess an unparalleled, three-dimensional understanding of the osseous and neurovascular anatomy of the entire femur and the knee joint. The femoral shaft itself is essentially tubular over the extent of the diaphyseal isthmus, but it undergoes a dramatic morphological transformation as it transitions distally. Infra-isthmally, the femur gradually flares, taking on a distinct trapezoidal cross-section as it forms the medial and lateral femoral condyles. Understanding this specific morphology is not merely an academic exercise; it is the fundamental basis for accurate nail sizing, determining the appropriate radius of curvature of the implant, and predicting the trajectory of the nail as it traverses the distal metaphysis into the rigid diaphyseal bone.
Our entry point is the absolute cornerstone of this entire procedure. A malpositioned starting point dictates a malaligned trajectory, which inevitably leads to iatrogenic deformity, cortical blowout, or catastrophic joint penetration. The ideal entry point is located at the distal end of the patellofemoral groove, situated precisely anterior to the femoral insertion of the posterior cruciate ligament (PCL). Radiographically, on a perfect anteroposterior (AP) fluoroscopic view, this point lies exactly in the midline or just a millimeter medial to the true midline between the medial and lateral condyles. On the lateral radiographic view, the entry point sits just anterior to the line of Blumensaat as it merges with the trochlear groove.

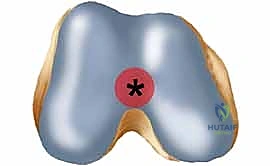
This specific, meticulously chosen flat articular area within the intercondylar notch is anatomically brilliant because it has minimal to absolutely no contact with the patella until the knee reaches approximately 120 degrees of deep flexion. By entering here, we create an ideal, low-impact entry zone that minimizes iatrogenic damage to the primary weight-bearing and articulating surfaces of the patellofemoral joint, thereby theoretically reducing the incidence of chronic, debilitating post-operative anterior knee pain.
Beyond the osseous landmarks, we must be acutely aware of the critical neurovascular structures that traverse the thigh, particularly when we turn our attention to the proximal interlocking screws. The femoral artery, having passed under the inguinal ligament, courses medially to the proximal femur. Crucially, its branches cross the anterior aspect of the femur more than 4 centimeters distal to the lesser trochanter. The femoral nerve branches cross even more proximally, starting approximately 4 centimeters distal to the piriformis fossa. When we insert our proximal locking screws in a retrograde nail (which typically sit in the subtrochanteric region), we are operating in dangerously close proximity to these vital structures.
Damage to the femoral neurovascular bundle caused by proximal locking screw insertion or errant drill bits can be reliably avoided by adhering to strict, meticulous surgical technique. We must absolutely limit medial soft tissue dissection and ensure that our screw placement is localized at or slightly above the level of the lesser trochanter, utilizing protective soft tissue sleeves down to the bone. Aggressive, blind medial soft tissue stripping in the proximal thigh is a hallmark of an amateur surgeon and directly jeopardizes these structures. Furthermore, while the sciatic nerve is posterior and less directly involved in the immediate anterior surgical field, it remains at significant risk with gross fracture displacement, excessive intraoperative traction on a fracture table, or careless manipulation of the limb. Gentle, deliberate reduction maneuvers and profound respect for the soft tissue envelope are paramount.
Exhaustive Indications and Contraindications
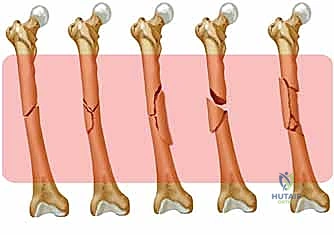
Retrograde femoral nailing is an extraordinarily versatile technique, but its application must be governed by strict adherence to established biomechanical principles and patient-specific physiological factors. In the broadest sense, virtually all diaphyseal femoral shaft fractures, as classified by the classic Winquist-Hansen system, are technically suitable and highly amenable to this approach. Whether dealing with a simple transverse Winquist Type I fracture or a highly comminuted, segmentally unstable Winquist Type IV fracture, the load-sharing capabilities of a reamed, statically locked retrograde intramedullary nail provide excellent biomechanical stability and high rates of clinical union.
However, the true mastery of this technique lies in recognizing its distinct advantages in specific, complex clinical scenarios. In the polytraumatized patient, retrograde nailing is often the procedure of choice. The ability to perform the surgery with the patient positioned completely supine, without the need for a radiolucent hip bump or a complex fracture table setup, facilitates a simultaneous, multi-team surgical approach. General surgeons can perform exploratory laparotomies, while neurosurgeons address cranial vaults, all while the orthopedic team stabilizes the femur. Furthermore, this supine positioning is critical for maintaining strict spinal precautions in patients with concomitant, unstable cervical or thoracolumbar spine injuries.
In the context of the "floating knee" (ipsilateral fractures of the femur and tibia), retrograde femoral nailing combined with antegrade tibial nailing allows the surgeon to address both catastrophic injuries through a single, continuous sterile field and often a single peri-articular knee incision, drastically reducing operative time and physiological stress. Similarly, for bilateral femur fractures, both lower extremities can be prepped and draped simultaneously, eliminating the need for time-consuming intraoperative repositioning. In pregnant patients, the retrograde approach is heavily favored as the supine positioning and distal location of the primary C-arm fluoroscopy significantly decrease direct and scatter radiation exposure to the developing fetus compared to antegrade nailing on a fracture table.
We must also critically evaluate the proximal and distal extensions of the fracture to determine if retrograde nailing remains biomechanically sound. For proximal extension into the subtrochanteric region, we rely on the Russell-Taylor classification. Retrograde nailing can be cautiously considered for Russell-Taylor Type IA fractures, where the lesser trochanter and piriformis fossa remain anatomically intact, providing a medial cortical buttress. However, if the fracture extends proximally to involve the lesser trochanter or the piriformis fossa (Type IB, IIA, IIB), proximal interlocking screw fixation of a retrograde nail would be critically compromised, and alternative fixation methods, such as a cephalomedullary nail or a fixed-angle plate, are absolutely mandated.

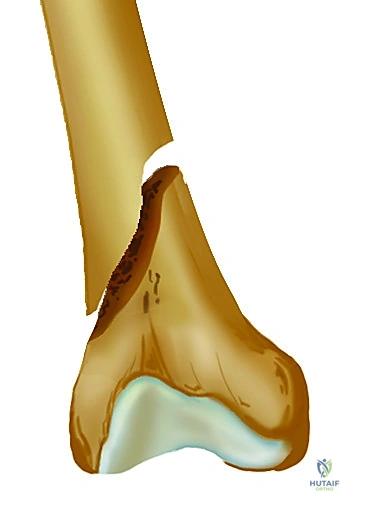
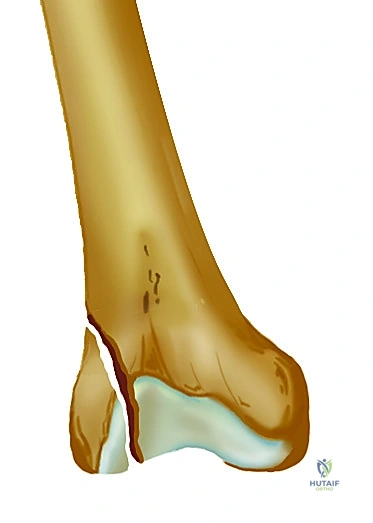
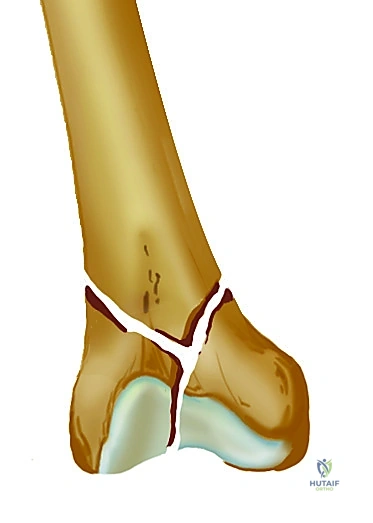
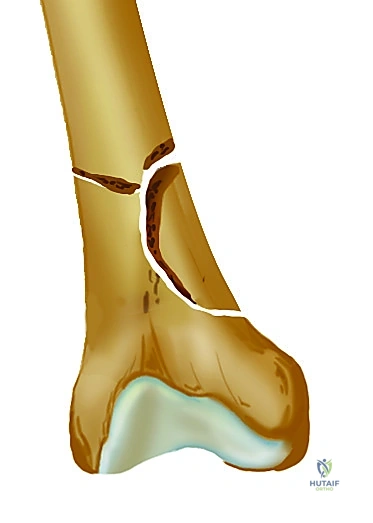
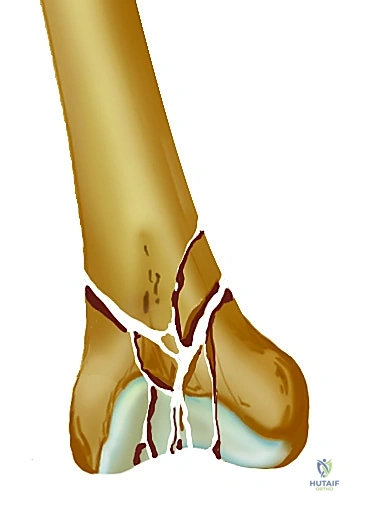
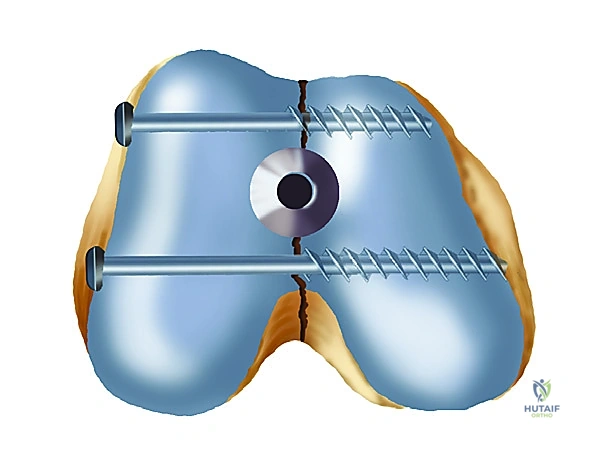
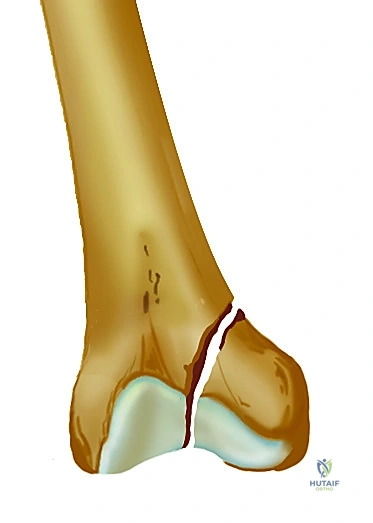
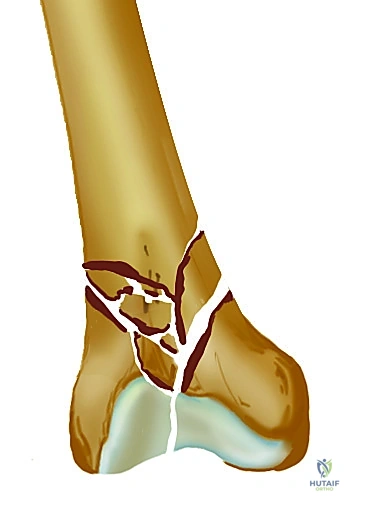
Distally, retrograde nailing is an excellent option for specific supracondylar femur fractures, guided by the Muller AO classification. Extra-articular (Type A) and simple partial articular (Type C1) fractures are often highly amenable to this technique, provided there is sufficient distal bone stock for at least two, and preferably three, multi-planar interlocking screws. However, the presence of complex, highly comminuted intra-articular fractures (Type C2, C3), or the presence of a coronal plane Hoffa fracture, represents a strict contraindication to standard retrograde nailing, as the nail passage will invariably displace the articular fragments and compromise joint congruity.
Indications and Contraindications Summary
| Category | Specific Clinical Scenario | Rationale / Biomechanical Consideration |
|---|---|---|
| Absolute Indications | Polytrauma with unstable spine | Supine positioning maintains spine precautions; allows multi-team approach. |
| Absolute Indications | Floating Knee (Ipsilateral Tibia/Femur) | Single surgical field and setup for both retrograde femur and antegrade tibia. |
| Absolute Indications | Bilateral Femoral Shaft Fractures | Decreases operative time; avoids repositioning between sides. |
| Relative Indications | Morbid Obesity | Easier access to distal femur compared to deep proximal antegrade starting point. |
| Relative Indications | Ipsilateral Pelvic/Acetabular Fracture | Spares the proximal hip abductor musculature and avoids compromising future surgical approaches. |
| Relative Contraindications | Proximal Subtrochanteric Extension | Contraindicated if lesser trochanter/piriformis fossa are involved (Russell-Taylor IB, IIA, IIB). |
| Absolute Contraindications | Coronal Plane Hoffa Fractures | Nail insertion will displace articular fragments; requires rigid lag screw/plate fixation. |
| Absolute Contraindications | Active Knee Joint Infection | Passing hardware through an infected joint into the medullary canal will seed the entire femur. |
Pre-Operative Planning, Templating, and Patient Positioning
The success of a retrograde femoral nailing procedure is inextricably linked to the meticulousness of the preoperative planning phase. Before the patient is even transported to the operating room, a comprehensive and exhaustive imaging workup is absolutely mandatory. We require high-quality, orthogonal AP and lateral radiographs of the full length of the femur, ensuring the entire diaphysis is visualized. Crucially, we must also obtain formal, dedicated AP and lateral radiographs of both the hip and the knee joints. The knee radiographs must be scrutinized for subtle patellar impaction fractures, undisplaced tibial plateau fractures, or any pre-existing arthritic changes that might complicate our intra-articular entry point.
The evaluation of the hip is of paramount importance. The surgeon must meticulously scrutinize the AP and cross-table lateral hip radiographs to definitively rule out an associated ipsilateral femoral neck fracture. The literature demonstrates that concomitant femoral neck fractures occur in 1% to 6% of all femoral shaft fractures, and horrifically, they are initially missed in 20% to 50% of cases during the acute trauma evaluation. Because of this unacceptably high miss rate on plain radiography, it is now the standard of care in many level-one trauma centers, and my personal strong recommendation, to obtain a routine fine-cut Computed Tomography (CT) scan of the femoral neck as part of the initial trauma workup for any high-energy femoral shaft fracture.
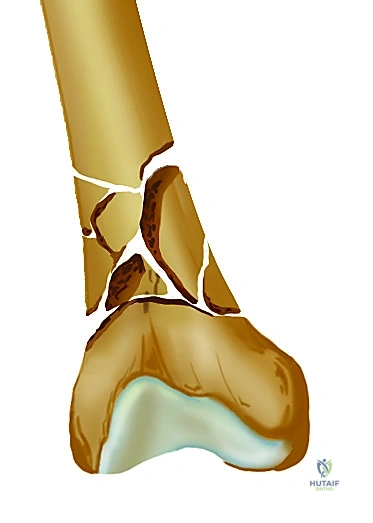
Furthermore, if dealing with a supracondylar distal femur fracture, a dedicated CT scan of the knee with sagittal and coronal reconstructions should always be obtained. This is vital to identify any occult coronal plane fractures, such as the aforementioned Hoffa fractures of the femoral condyles, which are notoriously difficult to appreciate on standard plain radiographs. As previously stated, any coronal fracture identified on CT is generally considered a strict contraindication for retrograde nailing due to the high probability of displacing the articular block and compromising distal interlocking screw fixation.
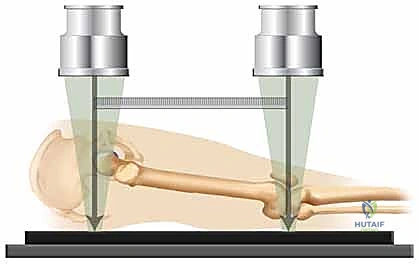
Once the imaging is complete, digital templating must be performed to estimate the required nail diameter and length. Using magnification markers, the narrowest portion of the medullary canal (the isthmus) is measured to estimate the reamer size and final nail diameter. Nail length is templated from the intercondylar notch to the level of the lesser trochanter. Patient positioning is equally critical. The patient is placed supine on a fully radiolucent flat Jackson table or a standard operating table with a radiolucent extension. A sterile bump may be placed under the ipsilateral hip to correct external rotation, and a sterile triangle or radiolucent bump is placed under the knee to maintain approximately 30 to 40 degrees of knee flexion. This flexion relaxes the gastrocnemius, aiding in the reduction of the distal fragment, and perfectly exposes the intercondylar notch for our surgical approach. The C-arm fluoroscope is positioned on the contralateral side of the table, ensuring unimpeded orthogonal imaging of the entire femur from the hip to the knee.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach for retrograde femoral nailing demands precision and a profound respect for the extensor mechanism of the knee. We typically utilize a midline longitudinal incision, approximately 3 to 5 centimeters in length, centered over the inferior pole of the patella and extending distally over the patellar tendon. Following meticulous subcutaneous dissection and hemostasis, the paratenon is incised. The surgeon then has the option of a transpatellar tendon splitting approach or a medial parapatellar approach. The medial parapatellar arthrotomy is generally preferred as it avoids direct trauma to the substance of the patellar tendon, theoretically reducing the risk of post-operative tendonitis or rupture, and provides excellent, direct visualization of the intercondylar notch.
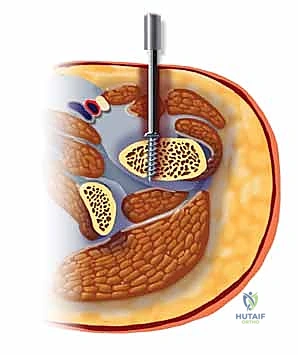
Once the joint is entered, any hemarthrosis is thoroughly evacuated, and the intercondylar notch is visualized. The starting point is established exactly anterior to the origin of the posterior cruciate ligament (PCL) in the intercondylar notch. A rigid, sharp guide pin is manually inserted into this exact footprint. Before advancing the pin into the distal metaphysis, its position must be absolutely confirmed with orthogonal AP and lateral fluoroscopy. On the AP view, the pin must be perfectly centered between the condyles; on the lateral view, it must align with the anterior extension of Blumensaat's line. Once confirmed, the pin is advanced, and a cannulated opening reamer or awl is passed over the pin to breach the dense metaphyseal bone and enter the medullary canal.

With the canal opened, a ball-tipped guide wire with a distinct bend at its tip is introduced. The fracture is manually reduced using longitudinal traction and manipulation, and the guide wire is carefully navigated across the fracture site and advanced proximally until its tip rests precisely at the level of the lesser trochanter. Sequentially increasing flexible intramedullary reamers are then passed over the ball-tipped wire. Reaming must be performed deliberately and steadily. The surgeon must feel for "cortical chatter"—the tactile feedback indicating the reamer is engaging the dense diaphyseal cortex. We typically ream 1.0 to 1.5 millimeters larger than the intended final nail diameter to ensure smooth, unhindered insertion and to prevent iatrogenic comminution or incarceration of the nail during passage.
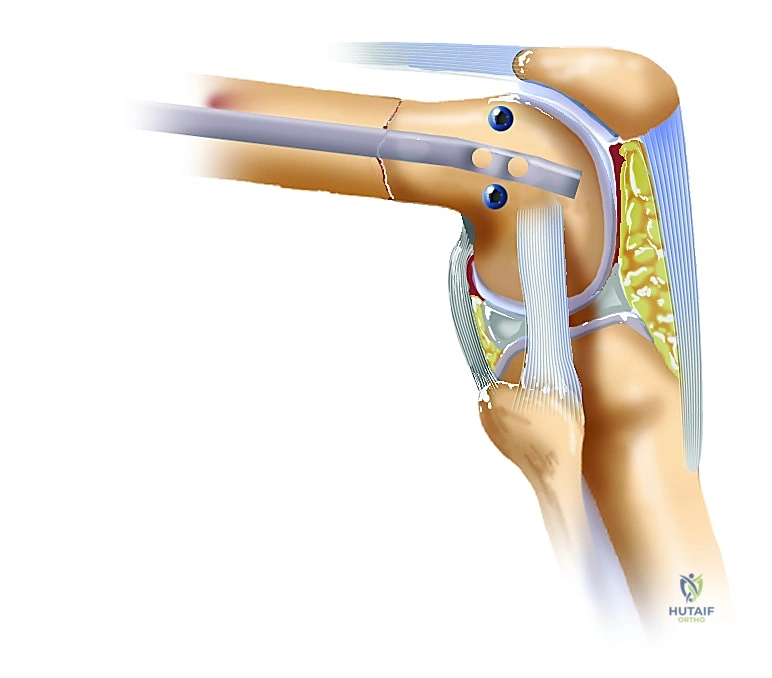
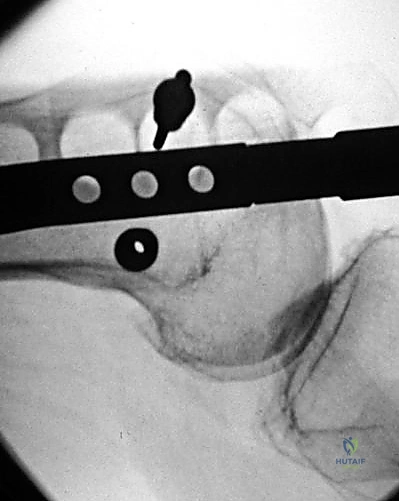
Following adequate reaming, the ball-tipped wire is exchanged for a smooth insertion wire using a plastic exchange tube. The selected retrograde nail is assembled onto the radiolucent insertion jig and advanced into the canal over the wire. The nail is gently impacted across the fracture site. Aggressive, forceful hammering must be avoided; if the nail is not advancing smoothly, the surgeon must stop, reassess the reduction, and potentially re-ream the canal. Once the nail is fully seated—ensuring the distal tip is countersunk 2 to 3 millimeters deep to the articular cartilage to prevent patellofemoral impingement—distal interlocking screws are placed through the outrigger jig. Proximal interlocking screws are then placed using a meticulous freehand "perfect circle" fluoroscopic technique, utilizing sharp trocars and tissue protection sleeves to absolutely safeguard the proximal neurovascular structures. Finally, a thorough, multi-planar fluoroscopic sweep of the entire femur, hip, and knee is performed to confirm perfect hardware placement, anatomic fracture alignment, and the absence of any iatrogenic fractures.
Complications, Incidence Rates, and Salvage Management
Despite the high success rates and biomechanical advantages of retrograde femoral nailing, it is a major surgical intervention fraught with potential complications. As master surgeons, we must not only be technically proficient in the primary procedure but also possess the advanced knowledge required to anticipate, diagnose, and definitively manage these complex sequelae. The most frequently cited complication specific to the retrograde approach is post-operative anterior knee pain. While the exact etiology is multifactorial, it is primarily attributed to iatrogenic damage to the intra-articular structures during the surgical approach, prominent hardware impinging on the patellar tendon or the patellofemoral articulation, or residual, unaddressed intra-articular debris.



Nonunion and delayed union represent significant, catastrophic failures of biological healing or mechanical stability. While the union rates for reamed retrograde nailing approach 95-98%, nonunions do occur, particularly in open fractures, highly comminuted segments lacking cortical contact, or in patients with severe metabolic comorbidities or a history of heavy tobacco use. Management of a hypertrophic nonunion, indicative of adequate biology but insufficient mechanical stability, typically involves dynamization of the nail (removing the static locking screws at one end) or an exchange nailing procedure to a larger diameter implant. Atrophic nonunions, characterized by a lack of biological activity, require a more aggressive approach, often necessitating exchange nailing combined with meticulous decortication and the application of autologous iliac crest bone graft or potent orthobiologics.
Malalignment, particularly apex posterior (procurvatum) and valgus deformities, is a notorious complication of distal third femoral fractures treated with intramedullary nails. The wide medullary canal in the distal metaphysis fails to provide the intimate cortical fit seen in the isthmus, allowing the distal fragment to toggle around the nail. This "bell-clapper" effect is exacerbated by the deforming forces of the gastrocnemius muscle pulling the distal fragment into flexion
