Femoral Shaft Fractures: Comprehensive Surgical Management and Osteosynthesis

Key Takeaway
Femoral shaft fractures represent a significant orthopaedic challenge, typically resulting from high-energy trauma. While locked intramedullary nailing remains the gold standard, plate osteosynthesis is crucial for polytraumatized patients with severe pulmonary compromise. This guide details evidence-based surgical techniques, biomechanical principles, and postoperative protocols to ensure optimal restoration of alignment, preservation of endosteal blood supply, and accelerated patient rehabilitation.
Comprehensive Introduction and Patho-Epidemiology
Fractures of the femoral diaphysis represent a formidable challenge in acute orthopaedic trauma surgery, characterized by their high energy mechanisms, complex biomechanical demands, and frequent association with life-threatening systemic polytrauma. As the largest, longest, and strongest tubular bone in the human body, the femur functions as the primary load-bearing strut of the lower extremity. The diaphyseal segment, extending from the lesser trochanter proximally to the supracondylar flare distally, is enveloped by a massive muscular mantle that provides a robust vascular supply but also exerts profound deforming forces upon fracture fragments. Consequently, diaphyseal fractures typically result from massive kinetic energy transfer—such as that experienced in high-speed motor vehicle collisions, motorcycle accidents, pedestrian-versus-auto incidents, or falls from significant heights.
The epidemiology of femoral shaft fractures demonstrates a classic bimodal distribution. The first and largest peak occurs in young adult males (ages 15 to 30 years) secondary to high-energy blunt trauma. These patients frequently present with concomitant multi-system injuries, including closed head trauma, blunt thoracic and abdominal injuries, and additional appendicular or axial skeletal fractures. The second peak occurs in the elderly population, predominantly females, where low-energy mechanisms such as ground-level falls lead to fractures in osteoporotic bone. Furthermore, the modern orthopaedic surgeon must be acutely aware of atypical femoral fractures (AFFs), which are increasingly recognized in patients on long-term bisphosphonate therapy. These fractures present with unique transverse or short oblique morphologies, lateral cortical thickening, and a prodrome of thigh pain, necessitating specific biomechanical considerations during osteosynthesis.
Without prompt, hemodynamically stabilized, and biomechanically sound surgical intervention, femoral shaft fractures precipitate catastrophic morbidity. The historical reliance on prolonged bed rest and skeletal traction carried unacceptably high rates of deep vein thrombosis (DVT), pulmonary embolism, decubitus ulcers, and severe pulmonary compromise. In the modern era, the systemic inflammatory response syndrome (SIRS) triggered by the massive release of inflammatory cytokines, marrow elements, and fat emboli from the fractured femur can rapidly progress to acute respiratory distress syndrome (ARDS) and multi-organ failure. Therefore, the definitive stabilization of the femoral shaft is not merely an orthopaedic endeavor to restore limb alignment; it is a critical, life-saving resuscitation maneuver that modulates the systemic inflammatory cascade.
The contemporary orthopaedic surgeon must possess a comprehensive armamentarium of fixation techniques, ranging from damage-control external fixation to definitive intramedullary nailing and advanced plate osteosynthesis. The selection of the optimal treatment modality is a highly nuanced decision, dictated by a multifactorial analysis of the fracture morphology (e.g., Winquist-Hansen classification), location, degree of comminution, soft-tissue envelope integrity, patient age, and, most importantly, the physiological status of the polytraumatized patient. The paradigm of Early Total Care (ETC) versus Damage Control Orthopaedics (DCO) remains a central tenet in the decision-making algorithmic pathway for these complex injuries.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of femoral anatomy and biomechanics is the cornerstone of successful osteosynthesis. The femoral diaphysis is not a perfect cylinder; it exhibits a distinct anterior bow (radius of curvature) that varies significantly among individuals and populations. The average radius of curvature is approximately 1.2 meters, a critical metric when selecting an intramedullary nail. A mismatch between the radius of curvature of the implant and the native femur can lead to iatrogenic anterior cortical perforation distally or malreduction of the fracture. The diaphysis is narrowest at the isthmus, typically located in the middle third of the bone, which dictates the maximum diameter of reamers and implants that can be safely accommodated without causing iatrogenic comminution.
The muscular anatomy surrounding the femur exerts predictable and powerful deforming forces on fracture fragments, which the surgeon must overcome to achieve anatomical reduction. In proximal third fractures, the proximal fragment is invariably flexed by the iliopsoas, abducted by the gluteus medius and minimus, and externally rotated by the short external rotators. Conversely, the distal fragment is pulled proximally and medially by the adductor complex. In middle third fractures, the adductors pull the distal fragment into varus and proximal translation. In distal third fractures, the gastrocnemius muscles exert a powerful flexion force on the distal fragment, resulting in a classic apex-posterior angulation that threatens the popliteal neurovascular bundle. Neutralizing these forces requires precise patient positioning, skeletal traction, and the strategic use of reduction adjuncts such as Schanz pins, reduction clamps, or blocking (Poller) screws.
The vascular supply to the femoral diaphysis is dual-sourced, comprising the endosteal and periosteal networks. The primary endosteal supply is derived from the nutrient artery, typically a branch of the second perforating artery of the profunda femoris, which enters the linea aspera at the junction of the proximal and middle thirds. This vessel supplies the inner two-thirds of the diaphyseal cortex. The periosteal supply, feeding the outer one-third of the cortex, is derived from the muscular perforators of the profunda femoris. In the event of a fracture, the medullary supply is disrupted, and the bone relies heavily on the periosteal network. Consequently, surgical approaches that require extensive subperiosteal stripping (such as traditional rigid plating) can devitalize the bone, increasing the risk of atrophic nonunion and infection. Closed intramedullary nailing respects this biological imperative by preserving the periosteal envelope and the fracture hematoma.
Biomechanically, the femur is subjected to immense axial, bending, and torsional forces during physiological loading. Intramedullary nails act as load-sharing devices. Because they are positioned within the medullary canal—co-linear with the mechanical axis of the bone—they are subjected to significantly lower bending moments compared to eccentrically placed plates. This central positioning allows for early, safe weight-bearing and stimulates secondary bone healing via endochondral ossification and robust callus formation. In contrast, plates function as load-bearing devices (until fracture union occurs) and must be placed on the tension band surface (the lateral cortex) to counteract the bending forces that naturally compress the medial cortex. The biomechanical efficacy of a plate construct depends heavily on its working length, the number of cortices engaged, and the utilization of interfragmentary compression where appropriate.
Exhaustive Indications and Contraindications
The selection of the appropriate fixation modality for a femoral shaft fracture requires a delicate balance between achieving mechanical stability, respecting the biological envelope, and optimizing the patient's systemic physiological status. While locked antegrade intramedullary nailing remains the undisputed gold standard for the vast majority of diaphyseal fractures, alternative modalities such as retrograde nailing, plate osteosynthesis, and external fixation possess highly specific and critical indications.
Intramedullary nailing is indicated for nearly all closed and most open (Gustilo-Anderson Types I, II, and IIIA) diaphyseal fractures. Antegrade nailing is the traditional approach, offering excellent biomechanical stability and high union rates. Retrograde nailing is specifically indicated for ipsilateral femoral neck and shaft fractures (allowing a single implant or separate implants to be placed without interference), floating knee injuries (permitting fixation of both the femur and tibia through a single knee incision), morbidly obese patients (where access to the piriformis fossa is anatomically prohibitive), and multiply injured patients where supine positioning without a fracture table expedites concurrent resuscitative and surgical procedures.
Plate osteosynthesis, while historically associated with higher rates of nonunion and infection due to soft-tissue stripping, remains an indispensable, life-saving technique in specific clinical scenarios. The most critical indication is the polytraumatized patient with severe blunt thoracic trauma or impending ARDS. In these "borderline" or "unstable" patients, the reaming and pressurization of the medullary canal required for IM nailing can precipitate a fatal "second hit" of fat embolization and inflammatory cytokine release. Plating provides definitive stabilization without canal pressurization.
External fixation is the cornerstone of Damage Control Orthopaedics (DCO). It is strictly indicated as a temporizing measure in hemodynamically unstable patients ("in extremis"), patients with severe head injuries where prolonged surgery or hypotension is contraindicated, or in the setting of catastrophic Type IIIB or IIIC open fractures with massive soft-tissue loss and gross contamination. The goal is to achieve rapid skeletal stability in under 30 minutes, controlling hemorrhage and allowing the patient to be transferred to the intensive care unit for physiological optimization prior to planned conversion to definitive internal fixation.
| Fixation Modality | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Antegrade IM Nail | Closed diaphyseal fractures; Gustilo I, II, IIIA open fractures; Pathological fractures. | Active medullary infection; Obliterated medullary canal; Unstable polytrauma with severe lung injury. | Morbid obesity; Ipsilateral femoral neck fracture; Severe pulmonary compromise. |
| Retrograde IM Nail | Ipsilateral neck/shaft fractures; Floating knee; Morbid obesity; Bilateral femur fractures. | Pre-existing knee sepsis; Distal femoral intra-articular comminution precluding locking. | Pre-existing knee arthroplasty (depending on component design); Patella baja. |
| Plate Osteosynthesis | Polytrauma with ARDS/chest trauma; Narrow canal; Vascular repair requiring exposure; Peri-prosthetic. | Severe osteopenia precluding screw purchase; Massive soft-tissue compromise over the lateral thigh. | Highly comminuted fractures where biological bridging is preferred over rigid fixation. |
| External Fixation | Hemodynamic instability (DCO); Type IIIC open fractures; Gross purulence/infection. | Definitive treatment in compliant adults (due to high nonunion/pin infection rates). | Minimal soft-tissue injury in a stable patient (unnecessary risk of pin tract seeding). |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the foundation of flawless execution in the operating theater. The evaluation must begin with high-quality, orthogonal radiographic imaging of the entire femur, encompassing both the hip and knee joints. It is an absolute orthopaedic imperative to actively rule out an ipsilateral femoral neck fracture, which occurs in up to 9% of all femoral shaft fractures. These proximal injuries are frequently non-displaced basicervical or vertical shear patterns that can be easily missed on standard AP pelvis radiographs, only to displace catastrophically during the antegrade nailing process. Therefore, a dedicated CT scan of the hip and pelvis is mandatory for all high-energy femoral shaft fractures prior to surgical intervention.
Pre-operative templating utilizes the uninjured contralateral femur to determine the appropriate length and diameter of the intramedullary nail or the required length of the plate. When templating for an IM nail, the surgeon must account for radiographic magnification (typically 10-15%). The nail diameter is estimated by measuring the narrowest point of the isthmus on the AP and lateral projections; the selected nail is generally 1 to 2 millimeters smaller than the reamed diameter to prevent cortical incarceration. Nail length is measured from the tip of the greater trochanter to the superior pole of the patella, ensuring the distal locking screws will engage the robust metaphyseal bone without penetrating the intercondylar notch.
Patient positioning is a critical decision that influences the surgical approach, reduction maneuvers, and fluoroscopic access. For antegrade intramedullary nailing, the patient is typically positioned supine or in the lateral decubitus position on a radiolucent fracture table. The supine position on a fracture table allows for the application of skeletal traction via a distal femoral or proximal tibial pin, utilizing a perineal post to provide counter-traction. This setup is highly effective for overcoming muscular deforming forces and restoring length. However, the perineal post carries a well-documented risk of pudendal nerve palsy, necessitating careful padding and limiting traction time.
Alternatively, many modern trauma surgeons prefer the "sloppy lateral" or completely lateral decubitus position on a flat radiolucent table, utilizing manual traction and a femoral distractor. This approach avoids the perineal post, facilitates access to the piriformis fossa in obese patients, and allows for easier soft-tissue clearance. For plate osteosynthesis or retrograde nailing, the patient is positioned supine on a flat, radiolucent table with a bump placed under the ipsilateral hip to control external rotation. A sterile tourniquet is rarely used for femoral diaphyseal plating due to the proximal location of the incisions, demanding meticulous intraoperative hemostasis by the surgical team.
Step-by-Step Surgical Approach and Fixation Technique
The execution of femoral osteosynthesis demands rigid adherence to biomechanical principles and soft-tissue respect. For the purpose of this definitive text, we will detail the anterolateral approach for plate osteosynthesis—a critical skill for the polytrauma setting—and the principles of antegrade intramedullary nailing.
The Anterolateral Approach and Plate Osteosynthesis
The anterolateral approach provides a safe, extensile internervous plane to the entire femoral diaphysis. The patient is positioned supine on a flat radiolucent table. A longitudinal incision is mapped along the axis connecting the anterior superior iliac spine (ASIS) to the lateral border of the patella. After incising the skin and subcutaneous tissues, the iliotibial band is sharply incised in line with its fibers.
Deep dissection exploits the plane between the rectus femoris (femoral nerve) and the vastus lateralis (femoral nerve). The vastus lateralis is retracted laterally and posteriorly. The critical step in this exposure is the meticulous elevation of the vastus lateralis from the linea aspera. The surgeon will encounter multiple perforating branches of the profunda femoris artery traversing the operative field. These vessels must be systematically identified, isolated, and either securely ligated or coagulated with bipolar electrocautery to prevent massive, limb-threatening postoperative hematomas.
Once the fracture site is exposed, the fracture hematoma is evacuated to allow for direct visualization of the cortical margins. For simple transverse or short oblique fractures, anatomical reduction is achieved using large Weber clamps or Jungbluth forceps. If the fracture pattern is oblique, absolute stability is mandated; this is achieved by placing one or two independent 4.5-mm interfragmentary lag screws across the fracture plane to generate compression.
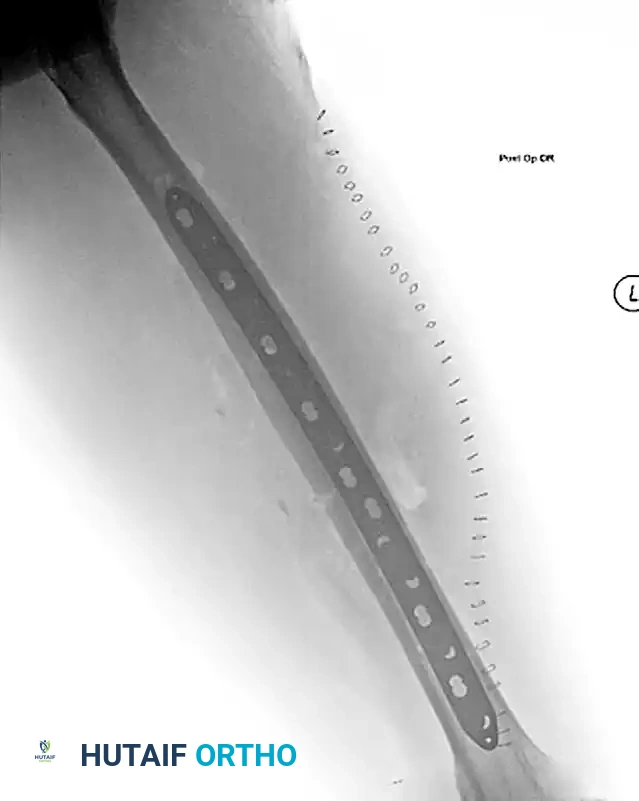
A pre-contoured 4.5-mm broad Low-Contact Dynamic Compression Plate (LC-DCP) or Locking Compression Plate (LCP) is then applied to the tension band surface (the lateral cortex). The plate must be of sufficient length to adhere to the working length principles—typically requiring a minimum of eight to ten cortices (four to five bicortical screws) of purchase proximal and distal to the fracture zone. The screws are inserted in a neutral mode if interfragmentary compression has already been achieved, or in a compression mode utilizing the eccentric drill guides if no lag screw was possible.

Antegrade Intramedullary Nailing
For antegrade nailing, access to the medullary canal is paramount. The entry point dictates the trajectory of the nail and prevents iatrogenic malalignment. The piriformis fossa entry point is co-linear with the anatomical axis of the medullary canal in the AP and lateral planes. The trochanteric entry point, slightly lateral to the piriformis fossa, requires a specifically designed nail with a proximal lateral bend to accommodate the offset.
Following the initial incision and fascial splitting, a guide pin is inserted into the chosen entry point under biplanar fluoroscopic guidance. A rigid opening reamer is used to breach the proximal cortex. A ball-tipped (olive) guide wire is then passed down the canal, navigated across the reduced fracture site, and advanced to the physeal scar in the distal femur. Sequential flexible reaming is performed over the ball-tipped wire, typically in 0.5-mm increments, until cortical "chatter" is felt, indicating engagement with the isthmic cortex. The canal is over-reamed by 1.0 to 1.5 mm larger than the selected nail diameter.
The selected nail is inserted over the guide wire. Gentle, controlled impaction is utilized; excessive force indicates cortical impingement and demands immediate removal and further reaming. Once the nail is seated at the appropriate depth, proximal and distal interlocking screws are placed. Distal locking is performed via a freehand perfectly round circles technique under fluoroscopy to ensure rotational stability and prevent axial telescoping.
Complications, Incidence Rates, and Salvage Management
Despite advances in surgical technique and implant metallurgy, the management of femoral shaft fractures remains fraught with potential complications. These range from devastating systemic sequelae to localized mechanical failures of the osteosynthesis construct. The orthopaedic surgeon must be vigilant in identifying and aggressively managing these complications to prevent long-term disability.
Systemic complications, particularly in the polytraumatized patient, are a primary concern. Fat Embolism Syndrome (FES) and Acute Respiratory Distress Syndrome (ARDS) occur secondary to the systemic inflammatory response and the intravasation of marrow contents during injury and subsequent intramedullary reaming. The incidence of clinically significant ARDS in polytrauma patients undergoing early IM nailing can approach 5-10%. Management requires aggressive intensive care support, mechanical ventilation, and, fundamentally, appropriate initial patient selection (utilizing DCO and plating in borderline patients to mitigate the "second hit").
Locoregional and mechanical complications include nonunion, malunion, infection, and hardware failure. Nonunion of the femoral shaft following IM nailing occurs in approximately 1-5% of cases, while rates following plate osteosynthesis can range from 5-15% depending on the degree of soft-tissue stripping. Hypertrophic nonunions, characterized by abundant callus formation that fails to bridge the fracture gap, indicate adequate biology but insufficient mechanical stability. These are typically managed by exchange nailing (reaming the canal to a larger diameter and inserting a thicker, stiffer nail). Atrophic nonunions, characterized by a lack of callus and tapering bone ends, indicate biological failure. Management requires debridement of the nonunion site, rigid stabilization (often converting to a plate or utilizing a larger nail), and the application of autologous bone graft (e.g., from the iliac crest) or orthobiologics.
Malunion, particularly rotational malalignment, is a subtle but highly morbid complication. Rotational discrepancies greater than 15 degrees compared to the contralateral limb can lead to significant gait abnormalities, patellofemoral pain, and early-onset osteoarthritis of the hip and knee. Prevention relies on meticulous intraoperative assessment utilizing fluoroscopic matching of the lesser trochanter profile and cortical step signs. If identified postoperatively, significant rotational malunion requires surgical correction via a derotational osteotomy.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Aseptic Nonunion | 1% - 5% (IM Nail) 5% - 15% (Plate) |
Smoking; NSAID use; Excessive soft-tissue stripping; Inadequate construct stability. | Hypertrophic: Exchange nailing or dynamization. Atrophic: Bone grafting + rigid fixation. |
| Deep Infection | 1% - 2% (Closed) 5% - 10% (Open Type III) |
Open fracture contamination; Prolonged operative time; Poor soft-tissue envelope. | Hardware removal (if loose); Radical debridement; Antibiotic cement spacer/nail; ExFix. |
| Rotational Malunion | 10% - 20% (>10° error) | Failure to assess clinical/fluoroscopic rotation intraoperatively; Comminuted fractures. | Preventative intra-op checks; Post-op derotational osteotomy if highly symptomatic (>15°). |
| Pudendal Nerve Palsy | 2% - 10% | Prolonged traction on fracture table perineal post; Inadequate padding. | Typically transient neuropraxia; Observation. Prevention via limiting traction time to <2 hours. |
| Hardware Failure | < 2% | Premature weight-bearing on load-bearing constructs (plates); Delayed union. | Revision osteosynthesis; Autologous bone grafting; Addressing the underlying nonunion. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation trajectory is intrinsically linked to the biomechanical properties of the specific fixation modality utilized. The fundamental goal of rehabilitation is to restore normal limb kinematics, prevent arthrofibrosis of the knee and hip, and stimulate biological fracture healing while protecting the mechanical integrity of the osteosynthesis construct.
Following intramedullary nailing, the rehabilitation protocol is generally aggressive. Because the locked IM nail is a load-sharing device positioned at the neutral mechanical axis of the femur, it exhibits exceptional resistance to bending moments. Consequently, patients with isolated femoral shaft fractures treated with an appropriately sized, statically locked IM nail are typically permitted immediate weight-bearing as tolerated (WBAT). Early axial loading generates controlled micromotion at the fracture site, which is a potent mechanical stimulus for endochondral ossification and robust callus formation. Physical therapy focuses on immediate, aggressive active and active-assisted range of motion (ROM) of the hip and knee. Strengthening of the quadriceps, hamstrings, and hip abductors is initiated early to prevent disuse atrophy.
Conversely, the rehabilitation protocol following plate osteosynthesis must be highly conservative and meticulously phased. Plates are eccentrically placed, load-bearing devices. Until the fracture biologically unites and begins to share the physiological load, the plate and screws are subjected to immense cyclical bending stresses. Immediate, unprotected weight-bearing in a plated femur carries a high risk of catastrophic hardware failure, including plate fatigue fracture or screw pullout.
* Phase I (0-6 Weeks): The patient is restricted to toe-touch weight-bearing (TTWB) or strict non-weight-bearing (NWB) utilizing bilateral axillary crutches or a walker. Despite the weight-bearing restrictions, aggressive early ROM of the hip and knee is absolutely critical. The vastus lateralis is frequently tethered by the surgical approach and the underlying plate; failure to mobilize the knee early will result in profound, recalcitrant arthrofibrosis and loss of terminal flexion.
* Phase II (6-12 Weeks): Clinical and radiographic assessments are performed. If serial radiographs demonstrate the formation of bridging callus across at least three cortices, the patient may begin a graduated progression to partial weight-bearing (PWB), typically advancing by 25% of body weight per week.
* Phase III (12+ Weeks): Progression to full, unprotected weight-bearing is permitted only after radiographic evidence of solid bony union is confirmed. Advanced proprioceptive and sports-specific rehabilitation is instituted to restore pre-injury functional baseline.
Regardless of the fixation method, all patients require stringent deep vein thrombosis (DVT) prophylaxis, typically utilizing low-molecular-weight heparin (LMWH) or direct oral anticoagulants (DOACs) for a minimum of 28 to 35 days postoperatively, given the high thrombogenic potential of major lower extremity trauma.
Summary of Landmark Literature and Clinical Guidelines
The evolution of femoral shaft fracture management has been shaped by several pivotal clinical studies that form the evidence-based foundation of modern orthopaedic trauma protocols. Familiarity with this landmark literature is essential for the academic surgeon and constitutes highly testable material for board examinations.
The paradigm shift toward Early Total Care (ETC) was catalyzed by the seminal work of Bone et al. (1989). In their landmark prospective study, they demonstrated that early intramedullary nailing (within 24 hours of injury) of femoral shaft fractures in polytrauma patients significantly reduced the incidence of ARDS, fat embolism, and intensive care unit length of stay compared to delayed fixation. This established early stabilization as a critical resuscitative maneuver rather than merely an orthopaedic procedure.
However, the concept of ETC was subsequently refined by the recognition that not all polytrauma patients can tolerate early, definitive IM nailing. Pape et al. (1993 and 2002) introduced the concept of Damage Control Orthopaedics (DCO). Their extensive research demonstrated that in "borderline" or "unstable" patients—particularly those with concurrent severe blunt thoracic trauma—the intramedullary reaming process acts as a systemic "second hit," exacerbating the inflammatory cascade and precipitating multi-organ failure. Pape's work established the modern algorithmic approach: stable patients receive early IM nailing (ETC), while hemodynamically unstable or borderline patients receive rapid external fixation (DCO) with delayed conversion to definitive nailing once physiologically optimized.
The debate regarding reamed versus unreamed intramedullary nailing was definitively addressed by the Canadian Orthopaedic Trauma Society (COTS) in 2003. In a massive, multicenter randomized controlled trial, COTS demonstrated that reamed intramedullary nailing of closed femoral shaft fractures resulted in significantly higher union rates, lower times to union, and fewer hardware failures compared to unreamed nailing. This study solidified reamed antegrade nailing as the undisputed gold standard for closed diaphyseal fractures.
Finally, the role of plate osteosynthesis in the modern era was elucidated by Seligson et al. and further supported by contemporary trauma registries. While acknowledging the higher locoregional complication rates (nonunion and infection) associated with plating, these studies validated that in the severely polytraumatized patient with profound pulmonary compromise, plate osteosynthesis effectively avoids the medullary pressurization and fat embolization associated with IM nailing, thereby saving lives at the acceptable expense of potentially requiring secondary orthopaedic procedures for fracture union.
By integrating the biomechanical principles, meticulous surgical techniques, and evidence-based clinical algorithms detailed in this chapter, the orthopaedic surgeon is fully equipped to navigate the profound complexities of femoral shaft fractures, optimizing both systemic survival and long-term functional outcomes.
This academic synthesis is based on established protocols from Hutaifortho's Operative Orthopaedics and has been medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is designed to assist orthopedic residents, fellows, and practicing surgeons in surgical preparation and board reviews (AAOS, FRCS, Arab Board).

Chapter Index
- Comprehensive Introduction and Patho-Epidemiology
- Detailed Surgical Anatomy and Biomechanics
- Exhaustive Indications and Contraindications
- Pre-Operative Planning, Templating, and Patient Positioning
- Step-by-Step Surgical Approach and Fixation Technique
- Complications, Incidence Rates, and Salvage Management
- Phased Post-Operative Rehabilitation Protocols
- Summary of Landmark Literature and Clinical Guidelines
Back to Master Guide