Calcaneus Fractures: Surgical Management & Techniques
Key Takeaway
Intraarticular calcaneus fractures present significant reconstructive challenges. Successful management requires a thorough understanding of hindfoot pathoanatomy, precise CT-based classification, and meticulous soft tissue handling. This guide details the biomechanics of axial load injuries, the Sanders classification system, and step-by-step surgical techniques for open reduction and internal fixation (ORIF) using the extensile lateral approach to restore the Böhler angle and subtalar congruency.
INTRAARTICULAR FRACTURES OF THE CALCANEUS
Intraarticular fractures of the calcaneus represent some of the most challenging injuries in orthopedic traumatology. Historically associated with poor outcomes and significant long-term disability, the management of these fractures has evolved dramatically with the advent of advanced computed tomography (CT) imaging, refined surgical approaches, and modern internal fixation techniques. For the practicing orthopedic surgeon, achieving a successful outcome requires a profound understanding of hindfoot biomechanics, meticulous soft-tissue management, and precise restoration of articular congruency and calcaneal morphology.
Mechanism of Injury and Pathoanatomy
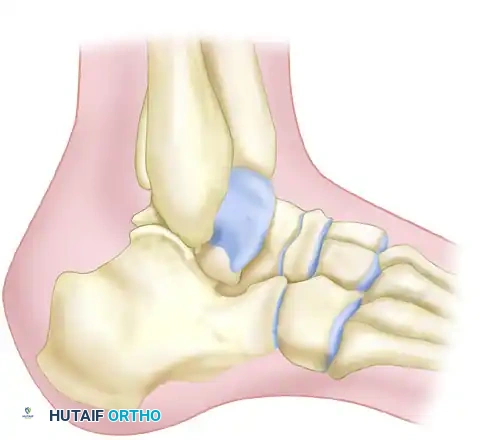
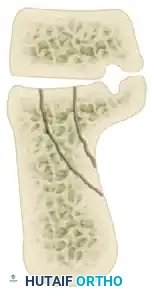
The vast majority of intraarticular calcaneal fractures occur as a result of high-energy axial loading, most commonly from a fall from a height or a motor vehicle collision. As the axial force is transmitted through the lower extremity, the talus acts as a wedge, driving into the calcaneus.
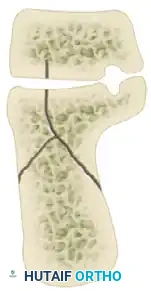
The primary fracture line is generated by a shear force. The lateral process of the talus acts as an anvil, splitting the calcaneus obliquely. This primary fracture line typically runs from posteromedial to anterolateral, dividing the calcaneus into two main fragments:
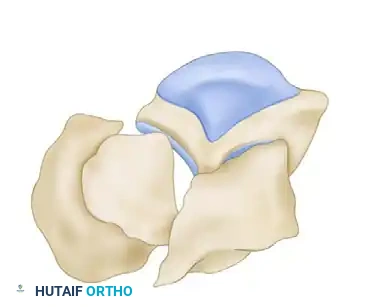
1. The Sustentacular Fragment (Medial Fragment): This fragment includes the sustentaculum tali and is strongly tethered to the talus by the robust interosseous talocalcaneal and deltoid ligaments. It remains anatomically aligned with the talus and serves as the "constant fragment" upon which the rest of the calcaneus must be reconstructed.
2. The Tuberosity Fragment (Lateral Fragment): This fragment displaces laterally, superiorly, and into varus due to the pull of the Achilles tendon.


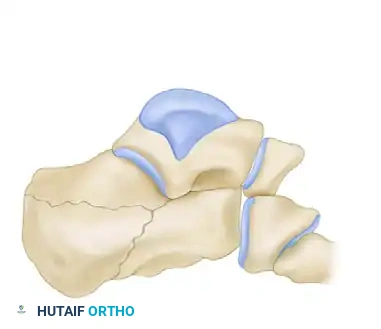
As the axial force continues, secondary fracture lines develop, dictating the specific fracture pattern. The talus pushes the posterior facet and the underlying thalamic fragment into the body of the calcaneus, simultaneously blowing out the lateral wall. This lateral wall blowout severely compromises the subfibular space, leading to impingement of the peroneal tendons and potential abutment against the distal fibula.
Clinical Pearl: As the deforming force is removed, the talus recoils, leaving a depressed thalamic fragment. The medial spike (attached to the sustentaculum) is often forcefully retracted into the medial soft tissues. In medially open fractures, this spike can penetrate the plantar-medial skin. Simply excising the skin wound is inadequate; deep dissection is mandatory to expose, thoroughly irrigate, and debride the medial spike.
The secondary fracture lines were classically described by Essex-Lopresti, dividing these injuries based on the exit point of the secondary fracture line:




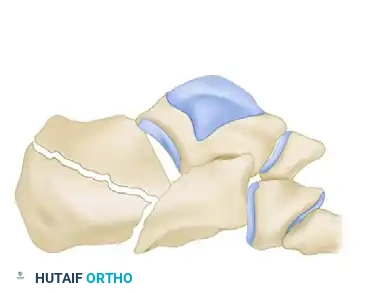
- Joint Depression Type: The secondary fracture line exits behind the posterior facet but anterior to the Achilles tendon attachment. The posterior facet is driven into the cancellous body of the calcaneus.
- Tongue Type: The secondary fracture line exits posteriorly, distal to the Achilles tendon insertion. The posterior facet remains attached to the posterior tuberosity, creating a single "tongue" fragment that rotates dorsally.
Radiographic Evaluation
A comprehensive radiographic evaluation is the cornerstone of preoperative planning. The standard trauma series should include five specific views:
-
Lateral Radiograph: Essential for assessing the loss of calcaneal height, the rotation of the posterior facet, and the measurement of the Böhler angle and the crucial angle of Gissane.

-
Axial (Harris) View: Evaluates the varus deformity of the tuberosity, the increase in heel width, and the status of the medial wall.
- Anteroposterior (AP) and Oblique Views of the Foot: Necessary to assess the involvement of the anterior process and the calcaneocuboid joint.
- Brodén View: Obtained by internally rotating the leg 40 degrees with the ankle in neutral, then angling the X-ray beam 10 to 15 degrees cephalad. This view is critical for evaluating the congruency of the posterior facet, particularly intraoperatively.

Advanced Imaging (Computed Tomography)
While plain radiographs provide a baseline, CT scanning is the gold standard and is mandatory for complete evaluation and surgical planning. Scans must be ordered in two specific planes:
* Semicoronal Plane: Oriented perpendicular to the normal position of the posterior facet. This is the most critical view for assessing articular comminution and applying the Sanders classification.
* Axial Plane: Oriented parallel to the sole of the foot, excellent for assessing the calcaneocuboid joint and the sustentaculum tali.
Surgical Warning: Never rely solely on a CT scan. CT can occasionally underestimate the sagittal plane rotation of a depressed fragment. Always correlate CT findings with plain lateral radiographs to fully appreciate the three-dimensional displacement.
Classification Systems
While the Essex-Lopresti system remains useful for describing the secondary fracture line (and is particularly relevant for percutaneous treatment of tongue-type fractures), it fails to quantify the energy absorbed by the posterior facet or the degree of articular comminution.
The Sanders Classification is the most widely accepted and prognostically validated system. It is based entirely on the semicoronal CT image showing the widest portion of the posterior facet. The classification is determined by the number and location of primary fracture lines running through the posterior facet.
The posterior facet is divided into three potential fracture lines (A, B, and C), creating four potential articular fragments (Lateral, Central, Medial, and Sustentacular).
* Line A: Lateral.
* Line B: Central.
* Line C: Medial (adjacent to the sustentaculum).
Sanders Classification Types:
* Type I: All non-displaced fractures (regardless of the number of fracture lines).
* Type II: Two-part fractures of the posterior facet (one fracture line). Subdivided into IIA, IIB, and IIC based on the location of the line.
* Type III: Three-part fractures (two fracture lines) featuring a central depressed fragment. Subdivided into IIIAB, IIIAC, and IIIBC.
* Type IV: Four-part (or more) highly comminuted fractures of the posterior facet.
CT Classification of Intraarticular Calcaneal Fractures (Sanders):














Surgical Decision Making
The management of calcaneal fractures requires a highly individualized approach. The learning curve for operative intervention is notoriously steep, and complication rates can be severe if patient selection is poor.
Goals of Treatment:
1. Restoration of congruency of the posterior facet of the subtalar joint.
2. Restoration of calcaneal height (Böhler angle).
3. Reduction of calcaneal width.
4. Decompression of the subfibular space to relieve peroneal tendon impingement.
5. Realignment of the tuberosity out of varus and into neutral/slight valgus.
6. Reduction of the calcaneocuboid joint, if involved.
Patient Selection Factors:
* Age: Most operative candidates are physiologically younger than 50-55 years. Older patients with lower functional demands or severe osteopenia are generally treated non-operatively.
* Health Status: Absolute or strong relative contraindications to open treatment include an insensate limb (due to sciatic/tibial nerve injury, diabetic neuropathy), severe peripheral vascular disease, and heavy tobacco use (which exponentially increases the risk of flap necrosis and deep infection).
* Fracture Pattern:
* Sanders Type I: Closed management.
* Sanders Type II & III: Open reduction and internal fixation (ORIF).
* Sanders Type IV: Can be treated non-operatively in poor hosts, or with ORIF and immediate primary subtalar arthrodesis in experienced hands.
Management of Open Calcaneal Fractures:
Open fractures carry a devastatingly high rate of deep infection (up to 39%), which can lead to amputation. Most open injuries result from the sustentacular spike penetrating the plantar-medial heel.
* Protocol: Urgent administration of IV antibiotics and aggressive serial irrigation and debridement.
* Lateral Wounds: May undergo open reduction through the traumatic wound with percutaneous fixation.
* Medial Wounds: If the wound is >4 cm, cannot be closed, or is unstable, provisional percutaneous fixation is applied. Definitive ORIF via an extensile lateral approach is delayed (average 18 days) until the medial soft tissues are pristine. If the medial wound is <4 cm and stable, standard ORIF can proceed once swelling subsides.
Operative Technique: Open Reduction and Internal Fixation (ORIF)
Timing of Surgery
Timing is dictated entirely by the soft tissue envelope. Surgery must be delayed until the massive initial edema has resolved, typically indicated by the presence of the "wrinkle sign" (return of skin lines on the lateral hindfoot). This usually takes 10 to 21 days. Operating through swollen, tense tissues guarantees wound dehiscence.
Positioning and Setup
The patient is placed in the lateral decubitus position on a radiolucent table. All bony prominences are padded. A beanbag is utilized to secure the torso. The operative leg is supported, and a high-thigh tourniquet is applied. Fluoroscopy must be positioned to easily obtain lateral, axial, and Brodén views without compromising the sterile field.
The Extensile Lateral Approach
The extensile lateral approach provides unparalleled access to the lateral wall, posterior facet, and calcaneocuboid joint.
- Incision: An L-shaped incision is made. The vertical limb is placed just anterior to the Achilles tendon, extending distally to the junction of the plantar and lateral skin (glabrous junction). The horizontal limb extends anteriorly along this junction toward the base of the fifth metatarsal.
- Flap Elevation: The incision is carried straight down to bone in a single layer. A full-thickness subperiosteal flap is elevated. This flap contains the sural nerve, peroneal tendons, and the calcaneofibular ligament.
- No-Touch Technique: To prevent flap necrosis, retractors (such as Kirschner wires) are placed into the talus, fibula, and cuboid to hold the flap out of the way. Never use self-retaining retractors or forceps on the skin edges.
Step-by-Step Reduction Sequence
1. Expose the Constant Fragment: The lateral wall is gently reflected outward (like opening a book) to expose the depressed posterior facet and the medial sustentacular fragment.
2. Reduce the Tuberosity: A Schanz pin is placed into the posteroinferior tuberosity. Using the pin as a joystick, the tuberosity is pulled out of varus, translated medially, and pulled plantarly to restore length, height, and alignment with the constant sustentacular fragment. This is provisionally pinned with K-wires.
3. Reconstruct the Posterior Facet: The depressed articular fragments are elevated and anatomically reduced against the talus and the sustentacular fragment. Subchondral K-wires are used to hold the articular reduction. A Brodén view is obtained to confirm absolute congruency.
4. Reduce the Anterior Process: If the calcaneocuboid joint is involved, it is reduced and pinned.
5. Reduce the Lateral Wall: The lateral wall is brought back into position, decompressing the subfibular space.
Internal Fixation
Once reduction is confirmed radiographically (Lateral, Axial, Brodén), a low-profile, anatomically contoured calcaneal locking plate is applied.
* Screws must be directed into the dense bone of the sustentaculum tali (the
📚 Medical References
You Might Also Like

