Eden-Lange Procedure: Scapular Stabilization for Trapezius Palsy

Key Takeaway
Join us in the OR for a detailed masterclass on the Eden-Lange procedure, a crucial technique for stabilizing the scapula in trapezius palsy. We'll meticulously cover patient selection, precise anatomical dissection, muscle transfer techniques, and critical neurovascular considerations. This guide provides an immersive, step-by-step approach to restoring shoulder girdle function and alleviating pain, emphasizing intraoperative decision-making and complication avoidance.
Comprehensive Introduction and Patho-Epidemiology
The Eden-Lange procedure represents a cornerstone in the reconstructive armamentarium for orthopedic surgeons managing the profoundly debilitating condition of trapezius palsy. Originally described independently by Eden in 1924 and Lange in 1951, this "triple transfer" technique involves the strategic repositioning of the levator scapulae, rhomboid minor, and rhomboid major to restore dynamic scapular stability. This is not a procedure undertaken lightly; it is a complex biomechanical reconstruction designed to salvage shoulder function when primary nerve repair is no longer viable. The primary goals are the alleviation of intractable shoulder girdle pain, the correction of severe cosmetic deformity, and the restoration of functional forward elevation and abduction by re-establishing a stable fulcrum for the deltoid and rotator cuff.
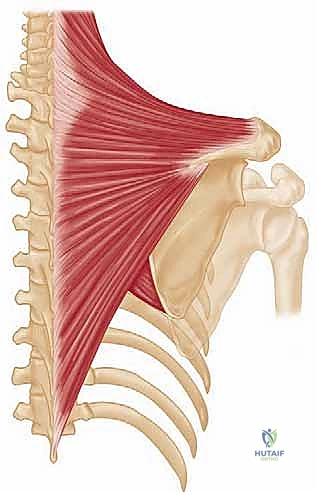
Trapezius palsy almost exclusively results from a disruption of cranial nerve XI, the spinal accessory nerve. Unlike many other major motor nerves, the spinal accessory nerve possesses a uniquely superficial and vulnerable course through the posterior cervical triangle. Here, it lies enveloped only by skin, subcutaneous fat, and a thin layer of investing deep cervical fascia. Because the spinal accessory nerve provides the sole motor innervation to the trapezius muscle, any significant insult to this nerve results in complete paralysis of the muscle. The trapezius is a massive, broad, and superficial muscle that serves as the primary dynamic stabilizer of the scapula, responsible for elevation, retraction, and upward rotation. Its loss catastrophically disrupts the intricate force couples of the shoulder girdle.
The etiology of spinal accessory nerve palsy is overwhelmingly iatrogenic. The most frequent causative event is a seemingly benign cervical lymph node biopsy in the posterior triangle of the neck. Surgeons operating in this region must maintain a high index of suspicion and meticulous surgical technique, yet injuries remain a persistent clinical reality. Other established causes include radical neck dissections for head and neck malignancies, blunt or penetrating trauma (including severe traction injuries to the shoulder girdle), viral neuritis, and exceedingly rare complications following internal jugular vein catheterization or carotid endarterectomy. Regardless of the etiology, the resulting biomechanical deficit is uniform and devastating.
Patients presenting with trapezius palsy exhibit a classic constellation of signs and symptoms that must be recognized promptly. The hallmark physical finding is lateral winging of the scapula. Due to the unopposed pull of the serratus anterior and pectoralis minor, the scapula translates laterally and inferiorly, with the inferior angle rotating outward. This must be carefully distinguished from the medial winging seen in serratus anterior palsy (long thoracic nerve injury). Furthermore, patients present with a profoundly asymmetric, drooping shoulder neckline due to trapezius atrophy, severe weakness in active forward elevation and abduction (rarely exceeding 90 degrees), and a deep, aching pain in the shoulder and neck. This pain is multifactorial, stemming from traction on the brachial plexus, compensatory muscle spasm in the levator and rhomboids, and mechanical impingement due to altered scapulohumeral rhythm.
Detailed Surgical Anatomy and Biomechanics
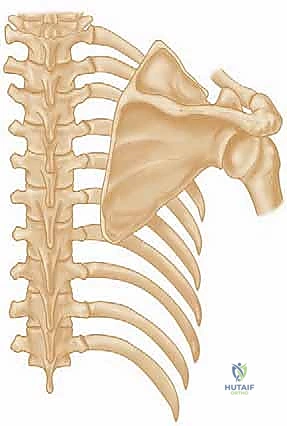
Mastery of the Eden-Lange procedure demands an intimate, three-dimensional understanding of the posterior shoulder and cervical anatomy. The surgeon must navigate a landscape of vital neurovascular structures while manipulating large muscle bellies to achieve precise biomechanical vectors. The trapezius itself, originating from the external occipital protuberance, nuchal ligament, and spinous processes of C7 through T12, normally inserts in a continuous V-shaped line along the lateral third of the clavicle, the acromion, and the spine of the scapula. Its three functional segments (upper, middle, and lower) work synergistically to elevate, retract, and upwardly rotate the scapula, providing a stable platform for the glenohumeral joint during arm elevation.
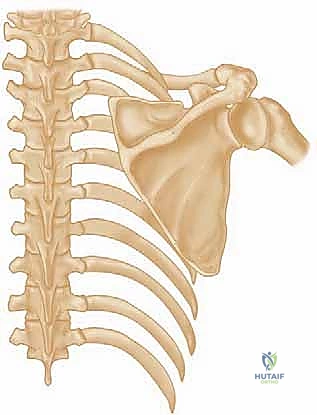
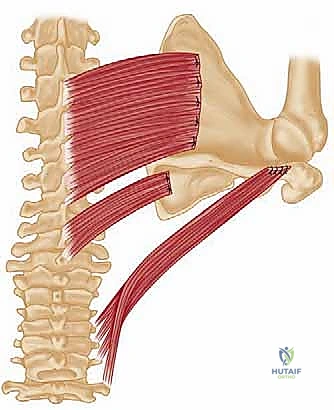
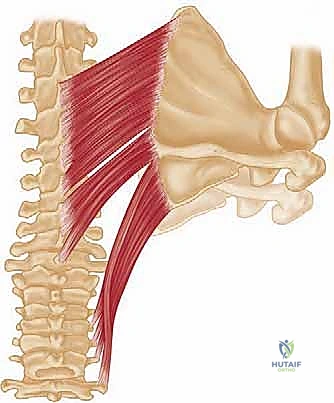
The success of the Eden-Lange transfer relies entirely on the robust health and appropriate redirection of three donor muscles: the levator scapulae, the rhomboid minor, and the rhomboid major. The levator scapulae originates from the transverse processes of C1-C4 and inserts onto the superior angle of the scapula. The rhomboid minor originates from the nuchal ligament and C7-T1 spinous processes, inserting at the medial border of the scapula at the level of the spine. The larger rhomboid major originates from T2-T5 spinous processes and inserts along the medial border of the scapula from the spine to the inferior angle. In their native anatomical positions, these muscles primarily elevate and retract the scapula, but they also act as downward rotators—a vector that must be fundamentally altered during the transfer to simulate trapezius function.

The neurovascular anatomy in this region is unforgiving, and iatrogenic injury during the transfer will guarantee clinical failure. The dorsal scapular nerve (DSN) is the most critical structure to protect. Originating primarily from the C5 nerve root, the DSN pierces the scalenus medius and courses inferiorly, deep to the levator scapulae and the rhomboids, providing their sole motor innervation. During the detachment of these muscles from the medial border of the scapula, the surgeon is operating mere millimeters from the DSN. Similarly, the transverse cervical artery (TCA), typically a branch of the thyrocervical trunk, accompanies the DSN to provide the primary blood supply to these muscles. Ligation of the superficial branch may occasionally be necessary for mobilization, but the deep branch must be meticulously preserved to prevent ischemic necrosis of the transferred muscle units.
Biomechanically, the Eden-Lange procedure is a masterclass in vector realignment. By transferring the levator scapulae laterally along the spine of the scapula (or to the acromion), its line of pull is lateralized, transforming it into a more effective scapular elevator and upward rotator, mimicking the upper trapezius. Transferring the rhomboid minor and major laterally into the supraspinous and infraspinous fossae, respectively, changes their moment arms. Instead of simply retracting and downwardly rotating the medial border, their new lateralized insertions allow them to stabilize the scapula against the thoracic wall and contribute to upward rotation when the arm is elevated. This re-establishes the critical force couple with the serratus anterior, restoring the dynamic fulcrum necessary for the deltoid to elevate the arm without the scapula slipping laterally and inferiorly.
Exhaustive Indications and Contraindications
The decision to proceed with an Eden-Lange transfer requires a rigorous patient selection process. This is a major reconstructive salvage procedure, and inappropriate application will lead to suboptimal outcomes and high patient dissatisfaction. The primary indication is a chronic, symptomatic trapezius palsy that has definitively failed conservative management or is no longer amenable to primary nerve repair or nerve grafting.
Timing is a critical variable in the decision-making algorithm. If a spinal accessory nerve injury is identified acutely (within 3 to 6 months), primary nerve repair, neurolysis, or nerve grafting is the absolute gold standard and should be attempted by a qualified microsurgeon. However, if the patient presents late—typically beyond 12 to 18 months post-injury—motor endplate degeneration within the trapezius becomes irreversible. At this chronic stage, nerve procedures are futile, and regional muscle transfer becomes the only viable surgical option to restore function and alleviate the debilitating traction pain associated with the drooping shoulder girdle.
A mandatory prerequisite for the Eden-Lange procedure is the presence of fully functional, innervated donor muscles. The levator scapulae and both rhomboids must demonstrate normal strength (Grade 5/5 on manual muscle testing) and normal electromyographic (EMG) activity. Furthermore, the serratus anterior must be intact. The Eden-Lange procedure relies on re-establishing a force couple; if the serratus anterior is also paralyzed (a combined long thoracic and spinal accessory nerve injury), the Eden-Lange transfer alone will fail to stabilize the scapula, and a more complex, multi-staged reconstructive approach or scapulothoracic fusion must be considered.
Contraindications must be strictly observed to avoid catastrophic surgical failures. Generalized myopathies, muscular dystrophies, or progressive neurodegenerative disorders are absolute contraindications, as the donor muscles will eventually succumb to the systemic disease process. A stiff glenohumeral joint (adhesive capsulitis) or severe glenohumeral osteoarthritis are relative contraindications; the shoulder must have full passive range of motion prior to a muscle transfer, or the newly transferred muscles will simply tether the scapula without restoring functional arm elevation.
| Category | Specific Criteria | Rationale |
|---|---|---|
| Absolute Indications | Chronic CN XI palsy (>12-18 months) | Motor endplates in trapezius are irreversibly degenerated; nerve repair is futile. |
| Absolute Indications | Failed primary nerve repair | Persistent symptomatic palsy despite prior microsurgical intervention. |
| Absolute Indications | Intact Dorsal Scapular Nerve (DSN) | Donor muscles (levator, rhomboids) must be fully innervated and functional (Grade 5/5). |
| Relative Indications | Intractable traction pain | The procedure effectively addresses the brachial plexus traction caused by the drooping shoulder. |
| Absolute Contraindications | Concomitant Serratus Anterior Palsy | The necessary force couple for upward rotation cannot be re-established. Consider fusion. |
| Absolute Contraindications | Denervated donor muscles | Transferring paralyzed muscles provides no dynamic stability and will stretch out. |
| Relative Contraindications | Severe Glenohumeral Stiffness | Lack of passive ROM will negate the functional benefits of the scapular stabilization. |
| Relative Contraindications | Non-compliant patient | Post-operative rehabilitation is rigorous and prolonged; failure to comply ruins the transfer. |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative preparation for the Eden-Lange procedure extends far beyond routine surgical clearance; it requires a comprehensive neuro-orthopedic evaluation. The foundation of this planning is a high-quality electrodiagnostic study (EMG/NCS). The EMG is non-negotiable; it serves a dual purpose. First, it definitively confirms the complete denervation of the trapezius, ruling out neurapraxia or partial injuries that might still recover spontaneously. Second, and most importantly, it verifies the absolute integrity of the dorsal scapular nerve and the robust electrical activity of the levator scapulae and rhomboid muscles. Proceeding without this confirmation risks transferring compromised muscle units.
Advanced imaging is highly recommended to complete the pre-operative picture. While a standard five-view radiographic shoulder series is obtained to rule out osseous deformities or arthropathy, Magnetic Resonance Imaging (MRI) of the shoulder and cervical spine is invaluable. MRI assesses the degree of fatty infiltration and atrophy within the trapezius, confirming chronicity. Furthermore, it evaluates the integrity of the rotator cuff. A massive, irreparable rotator cuff tear in the setting of trapezius palsy significantly alters the expected functional outcome and may necessitate a combined procedure or a shift in surgical strategy toward a reverse total shoulder arthroplasty if the patient is of appropriate age.
Patient counseling is arguably as critical as the surgical technique itself. The surgeon must set realistic expectations. Patients must understand that the Eden-Lange procedure is a salvage operation; it will not restore a "normal" shoulder. The primary realistic goals are the significant reduction of chronic neck and shoulder pain, the elimination of the cosmetic drooping, and the restoration of functional, but likely not full, overhead elevation (typically achieving 120 to 140 degrees of active forward flexion). The patient must also be mentally and physically prepared for a grueling, multi-month postoperative rehabilitation protocol involving strict initial immobilization.
In the operating room, precise patient positioning is paramount for optimal surgical exposure and intraoperative assessment of muscle tension. While some surgeons prefer the prone position, the lateral decubitus position is widely considered superior for this specific procedure. The patient is placed in the lateral decubitus position on a beanbag with all bony prominences meticulously padded. The operative arm is prepped and draped entirely free, allowing for full, unencumbered manipulation of the glenohumeral and scapulothoracic joints during the case. A sterile arm positioner (such as a Spider or TRIMANO arm) is highly advantageous for holding the arm in specific degrees of abduction and external rotation during the final tensioning and fixation of the muscle transfers. Fluoroscopy should be positioned to enter from the anterior aspect of the patient to assist with precise drill hole placement in the scapular body.
Step-by-Step Surgical Approach and Fixation Technique
Incision and Superficial Dissection
The surgical approach requires a wide, extensile exposure of the posterior hemithorax and scapula. The incision begins superiorly at the level of the C7 spinous process, roughly midway between the vertebral column and the medial border of the scapula. It extends inferiorly, paralleling the medial border of the scapula, and then curves gently outward (laterally) toward the posterior axillary fold, terminating a few centimeters distal to the inferior angle of the scapula. This J-shaped or curvilinear incision provides access to the entire medial border and the supraspinous and infraspinous fossae.

Following skin incision, dissection proceeds through the subcutaneous fat to identify the superficial fascia of the trapezius. In the setting of chronic palsy, the trapezius will be profoundly atrophied, appearing as a thin, translucent, and fibrotic sheet rather than a robust muscle belly. This atrophic trapezius is carefully incised in line with the skin incision and elevated as thick medial and lateral fasciocutaneous flaps. The lateral flap is elevated all the way to the spine of the scapula and the acromion, while the medial flap is elevated to expose the spinous processes. Meticulous hemostasis is maintained using electrocautery to ensure a clear operative field for the delicate neurovascular dissection that follows.
Identification and Mobilization of Donor Muscles
With the trapezius reflected, the underlying donor muscles—the levator scapulae, rhomboid minor, and rhomboid major—are brought into full view. The dissection begins superiorly with the levator scapulae. The muscle is identified as it descends from the cervical spine to insert on the superior angle of the scapula. Using blunt dissection, the areolar tissue surrounding the levator is cleared, and a vessel loop is passed around its belly for control.

Attention is then turned to the rhomboids. The distinct separation between the rhomboid minor (inserting at the base of the scapular spine) and the larger rhomboid major (inserting along the medial border down to the inferior angle) is identified. Vessel loops are similarly utilized to isolate these muscle bellies.

The most critical and treacherous phase of the operation is the detachment of these muscles from the scapula. The dorsal scapular nerve and the descending branch of the transverse cervical artery lie immediately deep to the insertion of the rhomboids and the levator on the medial border of the scapula. The surgeon must carefully elevate the muscles off the bone using a combination of sharp dissection and an elevator, staying strictly on the bone to avoid plunging deep into the neurovascular bundle. As the muscles are freed, they are mobilized medially. Fibrous bands tethering the neurovascular pedicle may need to be carefully released to allow for adequate lateral excursion of the muscles without placing tension on the nerve or artery.
Preparation of the Scapular Insertion Sites
Once the donor muscles are fully mobilized and protected, the recipient sites on the scapula must be prepared. The modern modification of the Eden-Lange procedure involves transferring the rhomboid minor into the supraspinous fossa and the rhomboid major into the infraspinous fossa. To achieve this, the fascia overlying the supraspinatus and infraspinatus muscles is incised. The muscle bellies of the supraspinatus and infraspinatus are gently elevated from their respective fossae using a Cobb elevator.
During the elevation of the supraspinatus and infraspinatus, the surgeon must exercise extreme caution to protect the suprascapular nerve and artery. These structures course through the suprascapular notch, run along the floor of the supraspinous fossa, wrap around the spinoglenoid notch, and enter the infraspinous fossa. Dissection should remain superficial to the deep fascia of these muscles where possible, or if subperiosteal elevation is performed, the neurovascular bundle must be directly visualized and protected. The bony surfaces of the supraspinous and infraspinous fossae, as well as the spine of the scapula, are lightly decorticated with a burr or rasp to create a bleeding bone bed, optimizing the biological environment for soft-tissue-to-bone healing.
Muscle Transfer, Tensioning, and Fixation
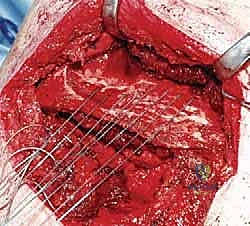
The final phase involves the precise routing, tensioning, and fixation of the transfers. Heavy, non-absorbable, braided sutures (e.g., #2 or #5 FiberWire) are woven into the tendinous ends of the levator scapulae, rhomboid minor, and rhomboid major using a locking Krackow or Bunnell technique to ensure a massive, pull-out resistant grip on the tissue.
The levator scapulae is routed laterally. In the classic description, it is transferred to the lateral aspect of the scapular spine. In modern variations, to maximize its moment arm for elevation, it may be tunneled subcutaneously and attached directly to the acromion. Fixation is achieved using robust suture anchors or transosseous bone tunnels.
The rhomboid minor is transferred laterally into the prepared supraspinous fossa, and the rhomboid major is transferred laterally into the infraspinous fossa. Fixation here is typically achieved by passing the sutures through transosseous drill holes made in the scapular body, tying them over cortical bone bridges on the deep (anterior) surface of the scapula, or utilizing modern, broad-footprint suture anchors if bone quality permits.

Crucially, the tensioning of these muscles must be performed with the arm held in approximately 60 to 90 degrees of abduction and slight external rotation. The scapula must be manually reduced into a neutral, retracted, and upwardly rotated position against the thoracic wall. The sutures are tied securely under maximum physiological tension. If the transfers are tied with the arm adducted, they will be too loose to provide dynamic stability when the patient attempts to elevate the arm.
Complications, Incidence Rates, and Salvage Management
The Eden-Lange procedure is a major reconstructive undertaking with a steep learning curve, and complications, while manageable, can significantly compromise the final outcome. The most devastating intraoperative complication is iatrogenic injury to the dorsal scapular nerve (DSN). The DSN is intimately associated with the deep surface of the donor muscles. If the DSN is transected or subjected to severe traction during mobilization, the transferred rhomboids and levator will become denervated, rendering the entire procedure a failure and leaving the patient with profound, uncorrectable winging. Meticulous, direct visualization of the nerve during the release from the medial scapular border is the only way to mitigate this risk.
Another significant neurologic risk involves the suprascapular nerve. During the preparation of the supraspinous and infraspinous fossae for the rhomboid transfers, aggressive use of elevators or poorly placed transosseous drill holes can compress or sever the suprascapular nerve at the spinoglenoid notch. This results in iatrogenic denervation of the infraspinatus and supraspinatus, adding a devastating external rotation weakness to the patient's existing pathology. Surgeons must maintain a healthy respect for the floor of the fossae and utilize fluoroscopy to guide drill placement safely away from the notch.
Mechanical failure of the transfer is a persistent concern, particularly in the early postoperative period. Suture pullout from the muscle belly, knot slippage, or anchor pullout from osteopenic scapular bone will result in immediate loss of tension and recurrent winging. This is most often caused by inadequate fixation techniques (failing to use locking stitches like a Krackow), insufficient decortication of the bone bed, or patient non-compliance with strict postoperative immobilization. If acute mechanical failure is identified clinically or via MRI, early revision surgery to re-anchor the muscles is mandatory.
Postoperative stiffness, particularly loss of internal rotation, is a common and somewhat expected sequela due to the tethering effect of the transferred muscles and the prolonged immobilization required for healing. While aggressive physical therapy can mitigate this, some degree of permanent motion loss is often the trade-off for restored stability. Infection and hematoma formation are standard risks of any large open procedure and are managed with meticulous hemostasis, prophylactic antibiotics, and, if necessary, prompt surgical evacuation.
| Complication | Estimated Incidence | Prevention & Salvage Strategy |
|---|---|---|
| Dorsal Scapular Nerve Injury | < 2% | Prevention: Meticulous subperiosteal dissection on the medial scapula; identify and protect the neurovascular bundle. Salvage: Scapulothoracic fusion if paralysis is permanent. |
| Suprascapular Nerve Injury | 1 - 3% | Prevention: Avoid deep dissection near the spinoglenoid notch; use fluoroscopy for drill holes. Salvage: Nerve exploration/grafting if identified early; tendon transfers (e.g., L'Episcopo) for ER loss. |
| Mechanical Failure / Pullout | 5 - 10% | Prevention: Use heavy #2 or #5 non-absorbable sutures with locking Krackow weaves; robust bone anchors or cortical bone bridges; strict post-op bracing. Salvage: Acute revision and re-fixation. |
| Recurrent Scapular Winging | 10 - 15% | Prevention: Tension the transfer with the arm in 60-90° abduction; ensure donor muscles are grade 5/5 pre-op. Salvage: Scapulothoracic fusion. |
| Post-operative Stiffness | 15 - 25% | Prevention: Adhere strictly to the phased rehab protocol; avoid over-tensioning beyond neutral scapular position. Salvage: Prolonged physical therapy; arthroscopic capsular release (rarely indicated). |
Phased Post-Operative Rehabilitation Protocols
The surgical execution of the Eden-Lange procedure is only half the battle; the postoperative rehabilitation protocol is equally critical to the ultimate success of the reconstruction. The transferred muscles must heal securely to their new bony insertions before they can be subjected to the immense forces required to stabilize the scapula. A premature return to active motion or a failure of patient compliance will inevitably result in stretching or catastrophic rupture of the repair.
Phase I: Strict Immobilization and Protection (Weeks 0 to 6)
Immediately postoperatively, the patient is placed in a custom orthosis or a specialized shoulder abduction brace (often an "airplane" splint) that holds the arm in approximately 60 degrees of abduction, 30 degrees of forward flexion, and neutral rotation. This position removes all tension from the transferred levator and rhomboids, allowing the soft-tissue-to-bone healing process to begin undisturbed. During this six-week phase, absolutely no active or passive glenohumeral motion is permitted. Rehabilitation is strictly limited to active range of motion of the cervical spine, elbow, wrist, and hand to prevent distal stiffness and deep vein thrombosis.
Phase II: Controlled Passive and Active-Assisted Motion (Weeks 6 to 12)
At the six-week mark, clinical healing is typically sufficient to begin weaning the patient from the abduction brace. The brace is initially removed for therapy sessions and gradually discontinued over a 2-to-3-week period. The focus of Phase II is restoring passive range of motion (PROM) and introducing active-assisted range of motion (AAROM). Therapists must be highly skilled, focusing on re-educating the transferred muscles to fire in their new biomechanical roles. Gentle, supine forward elevation and external rotation are initiated. Aggressive stretching, particularly cross-body
