Distal Radius Malunion: Surgical Correction & Osteotomy Guide
Key Takeaway
Distal radius malunion remains a significant cause of posttraumatic wrist disability, altering radiocarpal biomechanics and distal radioulnar joint kinematics. Surgical correction via corrective osteotomy is indicated for symptomatic patients with unacceptable radiographic parameters, such as dorsal tilt exceeding 20 degrees or radial shortening over 5mm. This guide details evidence-based evaluation, preoperative planning, step-by-step surgical approaches, and advanced fixation techniques to restore native anatomy and optimize functional outcomes.
DISTAL RADIUS MALUNION: PATHOPHYSIOLOGY AND BIOMECHANICS
Despite significant improvements in fracture treatment and internal fixation technologies since the early 1980s, malunion remains a common and challenging cause of residual disability following distal radial fractures. Modern orthopedic investigators have definitively refuted Abraham Colles’ 1814 observation that despite persistent deformity, the wrist will eventually "enjoy perfect freedom in all its motions and be completely exempt from pain."
While it is true that not all distal radial malunions are symptomatic—especially in elderly patients with low functional demands where no further treatment is indicated—posttraumatic wrist deformities in younger, active patients are frequently disabling enough to warrant complex surgical correction.
Etiology of Malunion
Fracture characteristics and the quality of initial treatment directly contribute to the development of a malunion. Common etiologies include:
* Failure to achieve an accurate initial anatomic reduction.
* Failure to maintain reduction due to inadequate immobilization or premature cast removal.
* Severe comminution, particularly involving the articular surface.
* Poor bone stock (severe osteoporosis).
* Unrecognized disruption of the distal radioulnar ligaments leading to instability.
Efforts to reduce the incidence of malunion have focused heavily on refining the indications and techniques for the surgical management of acute distal radial fractures, favoring rigid internal fixation over conservative casting in unstable patterns.
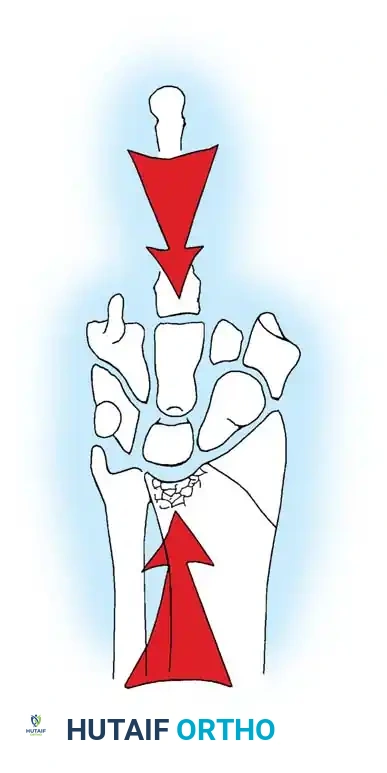
Biomechanical Consequences
Malunions of the distal radius may present with extraarticular deformities, intraarticular malalignment, distal radioulnar joint (DRUJ) incongruity, or a combination of these features. Extraarticular deformities typically manifest as radial shortening and excessive dorsal or volar tilt of the distal radial articular surface.
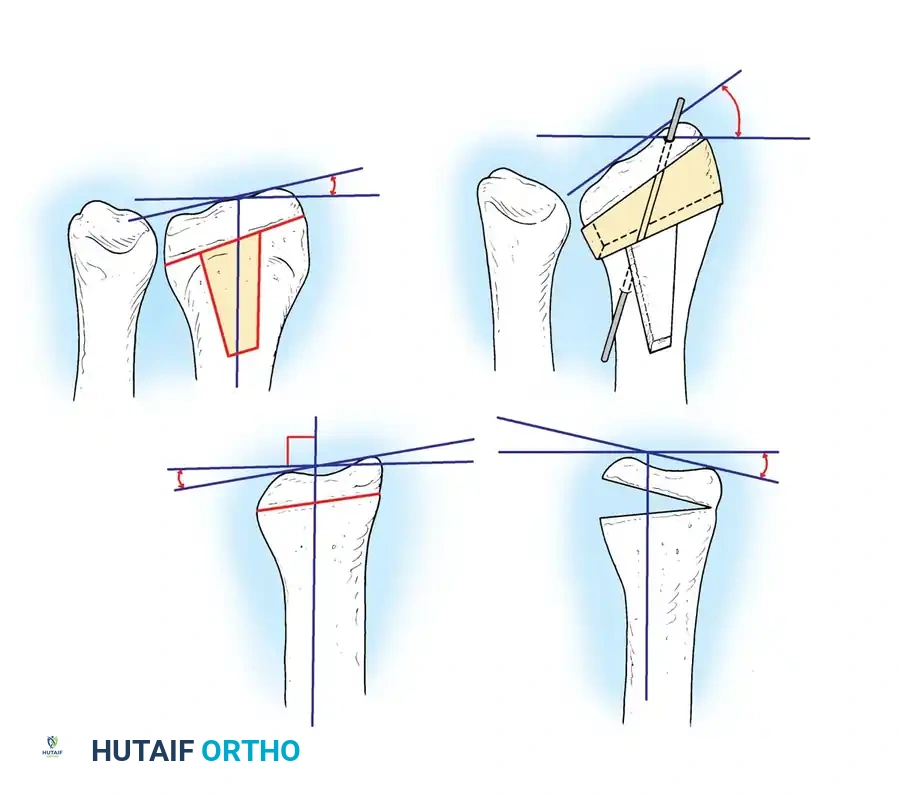
Clinical Pearl: Radiographic measurement of an intact, native distal radius demonstrates an average of 22 to 23 degrees of radial inclination, 11 to 12 mm of radial height, 11 to 12 degrees of volar tilt, and ± 2 mm of ulnar variance. Deviations from these parameters exponentially alter load transmission across the carpus.
Laboratory studies by Short et al. and Pogue et al. demonstrated that 20 to 30 degrees of dorsal tilt significantly alters the force distribution across the radiocarpal joint, shifting load abnormally onto the dorsal radiocarpal ligaments and the ulnar carpus.
Fernandez appropriately suggested that this degree of deformity should be classified as a "prearthritic condition." Furthermore, Zemel found that more than 10 degrees of dorsal tilt leads to decreased wrist flexion, and 6 mm of radial shortening causes profound dysfunction and impingement at the DRUJ.
CLINICAL AND RADIOGRAPHIC EVALUATION
Clinical Presentation
Pain, stiffness, weakness, and cosmetic deformity are the hallmark complaints in patients presenting with distal radial malunions.
* Pain Localization: Pain may be localized to the radiocarpal joint, the DRUJ, or both.
* Carpal Instability: Altered mechanics can induce carpal instability patterns causing midcarpal pain. Dorsally tilted malunions frequently result in Dorsal Intercalated Segment Instability (DISI) patterns. Conversely, die-punch fractures of the lunate facet can produce Volar Intercalated Segment Instability (VISI) patterns.
- Range of Motion Deficits: Decreased wrist flexion is typical of dorsally tilted malunions, whereas extension is limited with volarly tilted malunions (e.g., malunited Smith fractures). Loss of radial inclination impairs ulnar deviation.
- Neurological and Tendinous Complications: Symptoms of median nerve compression (carpal tunnel syndrome) may result from a dorsally tilted malunion increasing volar compartment pressure. Attritional ruptures of extensor tendons—most commonly the extensor pollicis longus (EPL)—and occasionally flexor tendons are well-documented sequelae.
Radiographic Criteria for Intervention
Plain anteroposterior (AP) and lateral radiographs of both wrists in neutral rotation are mandatory. The uninjured wrist serves as a critical template for surgical reconstruction.
While no absolute radiographic criteria define a "significant" malunion, several parameters correlate strongly with poor functional outcomes:
* Intraarticular Incongruity: Knirk and Jupiter, alongside Hastings and Leibovic, established that radiocarpal joint incongruity > 2 mm leads to poor results and inevitable posttraumatic arthritis.
* DRUJ Step-off: A 1 to 2 mm step-off at the DRUJ produces significant mechanical symptoms.
* Dorsal Angulation: Stockley and Porter noted that dorsal angulation > 20 degrees and radial inclination < 10 degrees cause a profound loss of grip strength.
* Sagittal Tilt: Fourrier et al. concluded that a loss of sagittal tilt of 20 to 30 degrees causes significant functional impairment.
Table 55-2: Radiographic Criteria for Acceptable Healing of Distal Radial Fractures (Graham & Hastings)
* Radioulnar length: Radial shortening of < 5 mm at DRUJ compared with contralateral wrist.
* Radial inclination: Inclination on PA film ≥ 15 degrees.
* Radial tilt: Sagittal tilt on lateral projection between 15-degree dorsal tilt and 20-degree volar tilt.
* Articular incongruity: Intraarticular step-off ≤ 2 mm at the radiocarpal joint.
Advanced imaging is often required. Computed Tomography (CT) is invaluable for evaluating DRUJ congruity (axial views) and the articular surface. MRI or arthrography is indicated to evaluate the integrity of the triangular fibrocartilage complex (TFCC) and intercarpal ligaments.
INDICATIONS AND CONTRAINDICATIONS FOR SURGERY
Surgical Indications
Operative intervention is indicated for distal radial malunions presenting with pain and functional deficits severe enough to interfere significantly with daily activities, coupled with correlative radiographic deformity.
Surgical Warning: Operative treatment is seldom indicated for minimally symptomatic patients, regardless of the severity of the radiographic or cosmetic deformity. The exception is a young, active patient (< 40 years old) with a deformity highly likely to become symptomatic (e.g., articular step-off > 2 mm, > 20 degrees dorsal angulation).
The CRPS Contraindication
Surgery is strictly contraindicated in patients with active Complex Regional Pain Syndrome (CRPS), historically known as Reflex Sympathetic Dystrophy Syndrome (RSDS).
* Early Stages: Characterized by extreme soft-tissue swelling, exquisite tenderness, and pain on motion.
* Late Stages: Circulatory changes occur; skin becomes purplish, cold, and hyperhidrotic. Joint stiffness becomes profound.
* Diagnosis: Three-phase delayed image bone scanning is diagnostic. Kozin et al. suggest abnormalities in any phase correlate with CRPS, while Mackinnon and Holder emphasize third-phase abnormalities.
* Management: CRPS must be treated and resolved before any reconstructive surgery. Treatment includes minimal immobilization, active/passive exercises, sympathetic blocks, and aggressive hand therapy. Surgery must be delayed until symptoms are static or definitively improving.
PREOPERATIVE PLANNING AND TEMPLATING
Meticulous preoperative planning is the cornerstone of a successful corrective osteotomy. The surgeon must determine the exact degree of correction required in the sagittal, coronal, and axial planes.
Using the contralateral normal wrist as a template, the surgeon calculates the osteotomy angle and the dimensions of the required bone graft.
The center of rotation of angulation (CORA) must be identified to ensure that the osteotomy corrects both the angular deformity and the translational displacement without creating secondary deformities.
SURGICAL TECHNIQUES: CORRECTIVE OSTEOTOMY
Procedures for distal radial malunions fall into three categories:
1. Radial Deformity Correction: Intraarticular and extraarticular osteotomies.
2. DRUJ Pathology Treatment: Ulnar shortening, hemiresection arthroplasty, Sauvé-Kapandji, or Darrach procedures.
3. Salvage Procedures: Limited/total wrist arthrodesis or proximal row carpectomy.
Extraarticular Malunion with Dorsal Angulation (Osteotomy and Grafting)
Osteotomy and bone grafting are most commonly indicated for malunited Colles fractures in active patients. The goal is to restore volar tilt, radial length, and inclination.
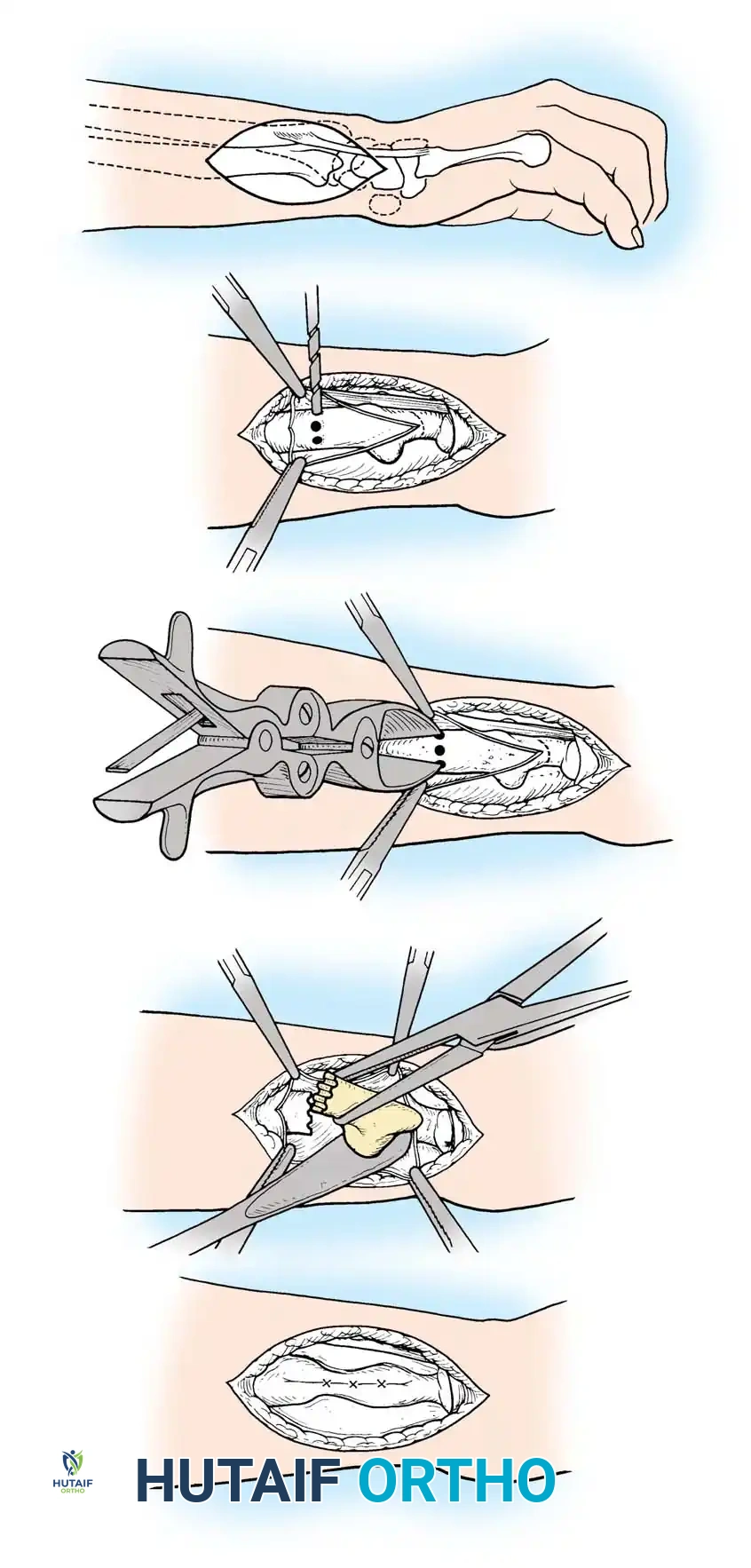
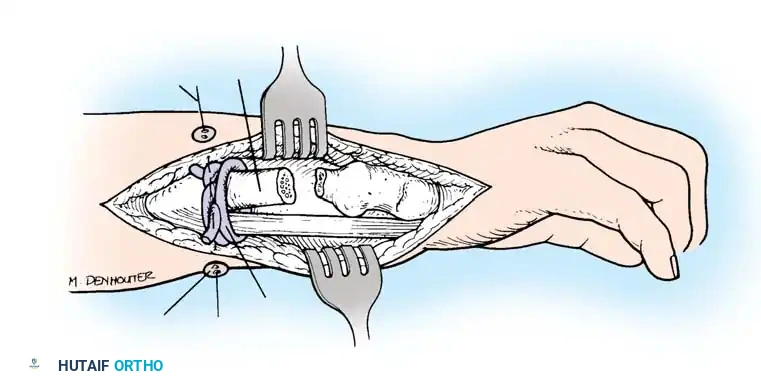
Step 1: Surgical Approach and Exposure
Depending on the deformity and planned fixation, a volar (modified Henry) or dorsal approach is utilized. Modern techniques heavily favor the volar approach using fixed-angle locking plates, as it avoids dorsal tendon irritation and allows for excellent restoration of the volar cortical buttress.
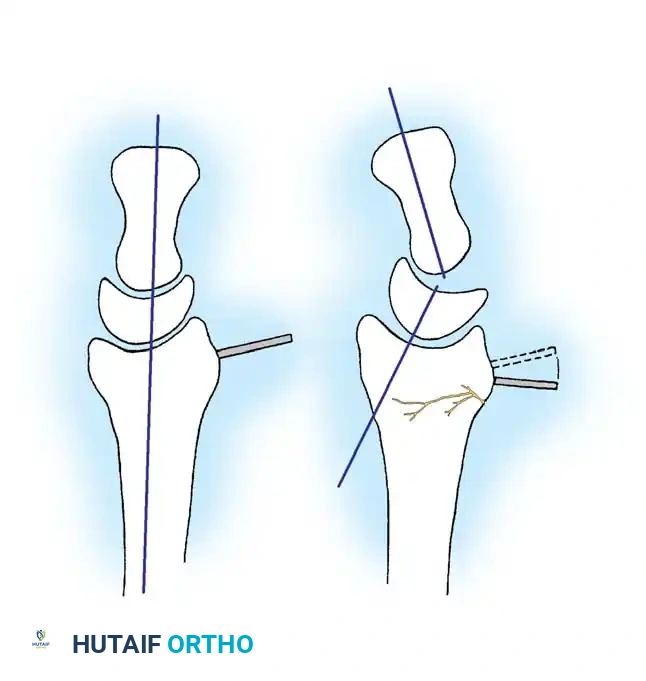
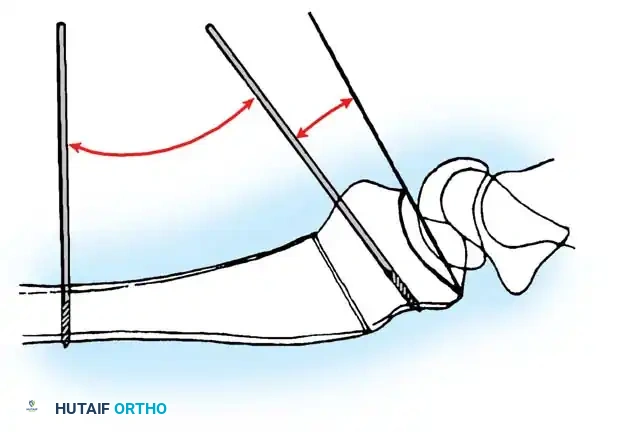
Step 2: Osteotomy Execution
Once the malunion site is exposed, K-wires are often placed parallel to the joint surface and perpendicular to the radial shaft to visually represent the planned correction angle.
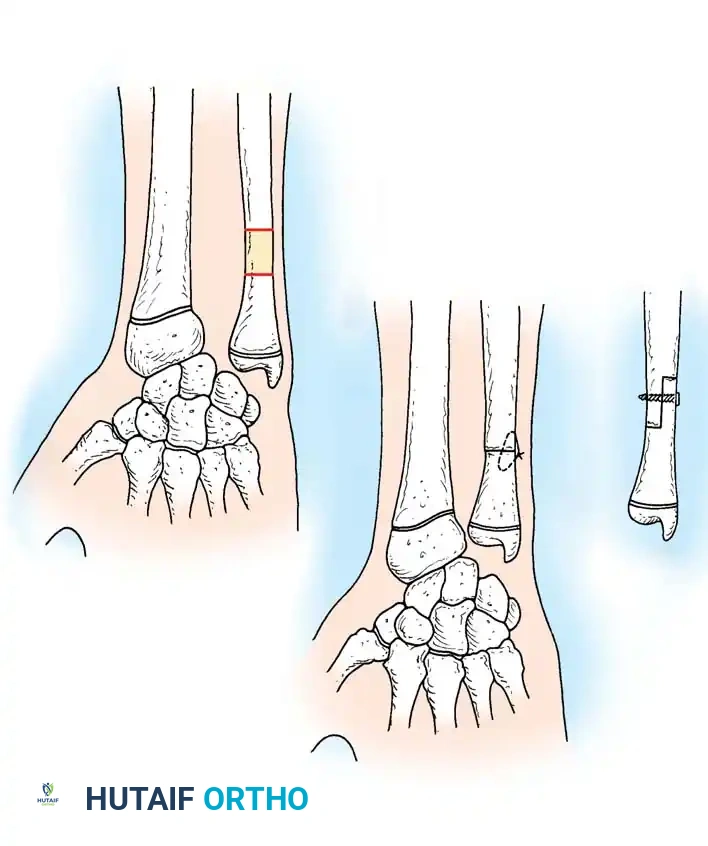
- Insert a 3.2-mm drill guide to the bone, and drill several holes in the radius along the planned osteotomy line to prevent thermal necrosis and control the osteotomy path.
- Complete the osteotomy using a thin oscillating saw or sharp osteotomes.
- In some historical or minimally invasive techniques, after drilling, the surgeon may perform a manual osteoclasis to complete the break, preserving the opposite periosteal hinge.
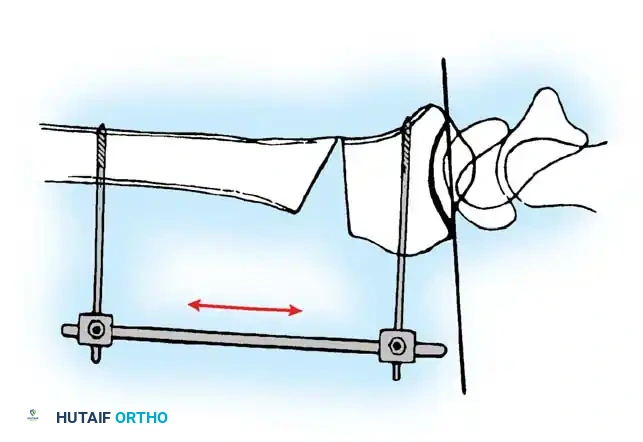
Step 3: Deformity Correction and Distraction
The osteotomy is opened to correct the dorsal tilt and restore radial length. This can be achieved using a lamina spreader inserted into the osteotomy gap or via a temporary external fixator applied to the radius and metacarpals to provide controlled distraction.
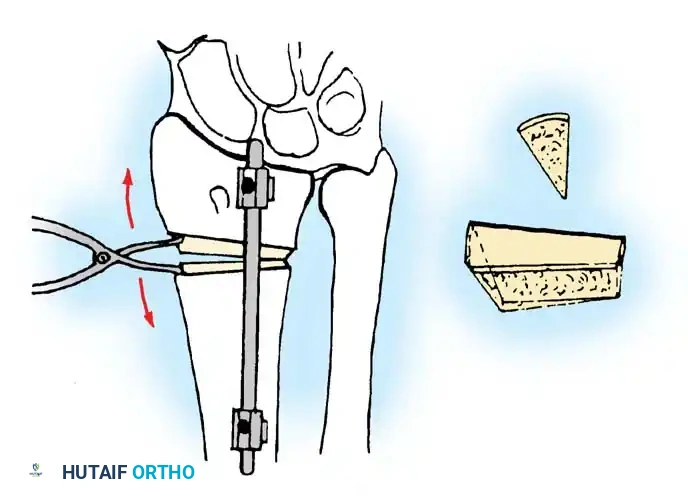
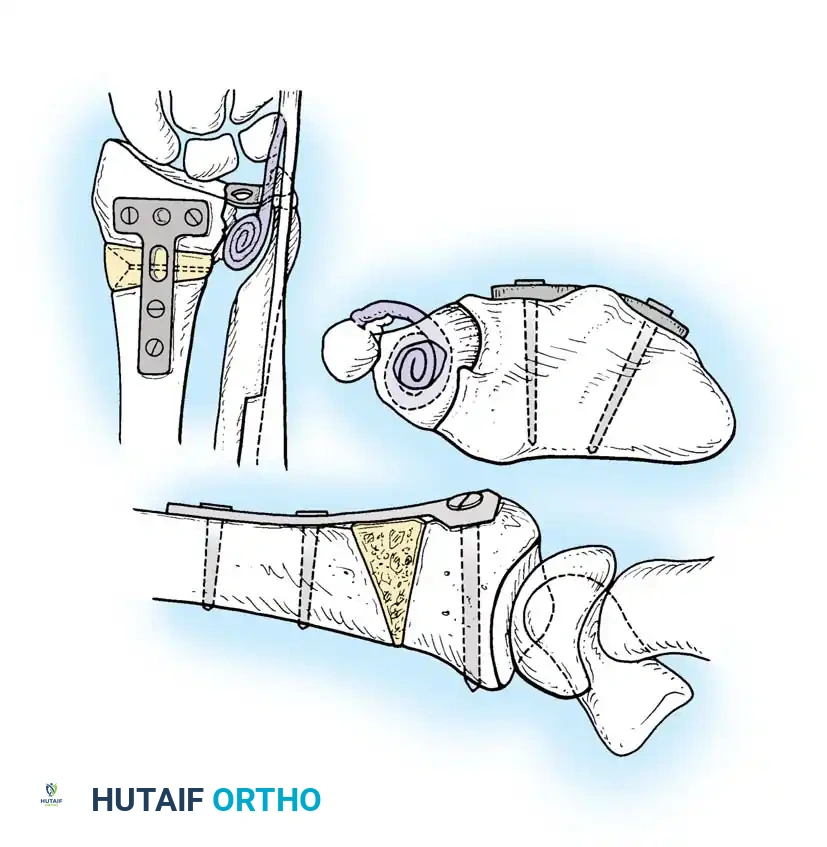
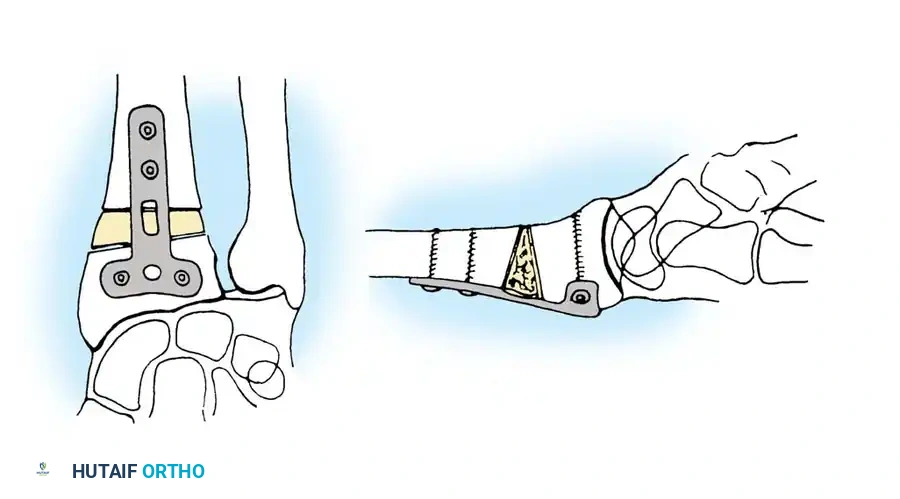
Step 4: Bone Grafting
Once the anatomic parameters (volar tilt, radial height, inclination) are restored, the resulting defect must be grafted.
* Structural Graft: A tricortical iliac crest bone graft is shaped to match the calculated defect (usually a trapezoidal wedge) and impacted into the osteotomy site.
* Cancellous Graft/Substitutes: If rigid volar locking plate fixation is used, the defect can often be filled with cancellous autograft, allograft, or osteoconductive bone substitutes, relying on the plate for structural stability.
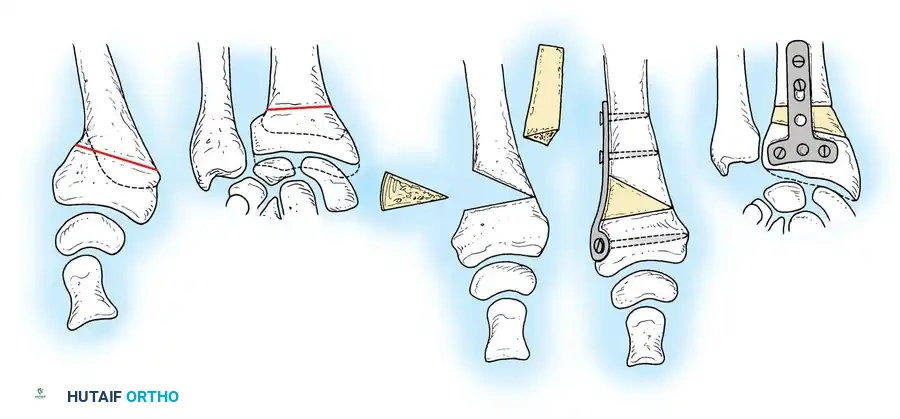
Step 5: Internal Fixation
Rigid internal fixation is applied. While dorsal plates were historically used, volar locking plates are now the gold standard. The plate is applied to the volar surface, compressing the graft and rigidly holding the corrected articular block.
- Apply a long arm, above-elbow cast or a rigid splint postoperatively depending on the stability of the fixation and bone quality.
MANAGEMENT OF THE DISTAL RADIOULNAR JOINT (DRUJ)
Distal radial osteotomy alone often corrects DRUJ incongruence by restoring the native sigmoid notch alignment. However, specific DRUJ procedures are required if incongruity persists or if arthritic changes are present.
Table 55-3: Guidelines for Treatment of DRUJ in Radial Malunions
| Radius Parameters | Radioulnar Length | DRUJ Reducible by Radial Osteotomy | Potential for DRUJ Congruity | Reconstruction Indicated |
| :--- | :--- | :--- | :--- | :--- |
| Unacceptable | Unacceptable | Yes | Yes | Distal Radial Osteotomy (DRO) |
| Acceptable | Unacceptable | Yes | Yes | Ulnar Shortening (US) |
| Unacceptable | Unacceptable | No | Yes | DRO + US (or two-stage) |
| Unacceptable | Unacceptable | No | No | DRO + DRUJ Ablation |
Ulnar Shortening Osteotomy
Oskam et al. and Flinkkilä et al. found that lengthening the distal radius more than 6 mm is usually impossible with a distal radial osteotomy alone due to soft tissue contractures. In cases with > 6 mm of radial shortening, a concomitant ulnar shortening osteotomy is required to restore ulnar variance and decompress the ulnocarpal joint.
DRUJ Ablation and Salvage Procedures
If the DRUJ is arthritic or irreversibly incongruent, salvage procedures are indicated:
* Bowers Hemiresection Interposition Arthroplasty: Resection of the articulating portion of the ulnar head with soft tissue interposition.
* Sauvé-Kapandji Procedure: Arthrodesis of the DRUJ combined with a proximal ulnar pseudarthrosis to maintain forearm rotation.

- Darrach Procedure: Resection of the distal ulna. This is technically simpler than radial osteotomy and provides excellent pain relief in older, low-demand patients. However, it does not correct the radial deformity and carries risks of ulnar stump instability and decreased grip strength.
POSTOPERATIVE PROTOCOL AND COMPLICATIONS
Rehabilitation
Postoperative management depends heavily on the rigidity of the fixation.
1. Phase I (0-2 weeks): Volar splint immobilization. Immediate active range of motion of the digits, elbow, and shoulder is mandatory to prevent stiffness and CRPS.
2. Phase II (2-6 weeks): Transition to a removable orthosis. Gentle active and active-assisted wrist ROM and forearm rotation begin.
3. Phase III (6-12 weeks): Progressive strengthening begins once radiographic evidence of graft incorporation and osteotomy union is observed.
Complications
- Nonunion/Delayed Union: Particularly at the graft-host interface. Mitigated by rigid fixation and meticulous graft preparation.
- Hardware Prominence/Tendon Irritation: More common with dorsal plating. Volar plates can irritate flexor tendons if placed distal to the watershed line.
- Loss of Correction: Can occur in severely osteoporotic bone if locking technology is not utilized or if the structural graft collapses.
- Median Nerve Neuropathy: Prophylactic carpal tunnel release should be considered during the index procedure if preoperative symptoms existed or if significant volar translation is performed during correction.
You Might Also Like
