INTRODUCTION TO LESSER TOE DEFORMITIES
Lesser toe deformities, specifically hammer toes and claw toes, represent a complex interplay of biomechanical imbalances within the forefoot. These conditions are characterized by progressive contractures of the interphalangeal and metatarsophalangeal (MTP) joints, leading to significant pain, altered gait mechanics, and the formation of intractable hyperkeratotic lesions.
A hammer toe is classically defined by an abnormal flexion contracture at the proximal interphalangeal (PIP) joint, often accompanied by a mild extension deformity at the MTP joint, while the distal interphalangeal (DIP) joint remains neutral or hyperextended. Conversely, a claw toe involves hyperextension at the MTP joint combined with flexion contractures at both the PIP and DIP joints, typically resulting from a global intrinsic minus foot or neuromuscular pathology.
When conservative management—such as extra-depth footwear, crest pads, and orthoses—fails to alleviate symptoms, surgical intervention becomes necessary. The cornerstone of correcting a moderate, rigid hammer or claw toe deformity is the PIP joint resection arthroplasty (condylectomy), often augmented by soft tissue balancing at the MTP joint.
Clinical Pearl: The primary goal of lesser toe surgery is not merely cosmetic straightening, but the restoration of a pain-free, plantigrade foot that can comfortably accommodate standard footwear. A slightly flexed, stable toe is functionally superior to a rigidly straight, fused toe.
PREOPERATIVE EVALUATION AND BIOMECHANICS
Pathoanatomy
The stability of the lesser toes relies on a delicate balance between the extrinsic musculature (extensor digitorum longus [EDL], flexor digitorum longus [FDL]) and the intrinsic musculature (lumbricals, interossei). In a hammer toe deformity, the intrinsic muscles fail to flex the MTP joint and extend the IP joints. This allows the EDL to hyperextend the MTP joint, while the FDL unopposedly flexes the PIP joint. Over time, the plantar plate and collateral ligaments contract, converting a flexible deformity into a rigid one.
Clinical Assessment
A thorough clinical examination must differentiate between flexible and rigid deformities, as this dictates the surgical approach.

FIGURE 83-16 A: Moderate hammer toe deformity demonstrating a fixed contracture at the proximal interphalangeal joint. Note the extensor tightness at the metatarsophalangeal joint, though without a fixed extension contracture.
- The Kelikian Push-Up Test: Apply pressure to the plantar aspect of the metatarsal head. If the MTP joint extension and PIP joint flexion correct, the deformity is flexible. If it remains fixed, osseous resection and capsular release are required.
- Neurovascular Status: Assess pedal pulses and capillary refill. Severe deformities in vasculopathic patients carry a high risk of postoperative ischemia.
- Skin Integrity: Evaluate the dorsal PIP joint for ulceration or severe hyperkeratosis, which will dictate the incision placement.
SURGICAL TECHNIQUE: PIP JOINT RESECTION ARTHROPLASTY
The following step-by-step protocol details the correction of a moderate hammer toe or claw toe deformity utilizing a dorsal elliptical incision, PIP joint resection, and extensor tendon balancing.
1. Incision and Superficial Dissection
Meticulous handling of the soft tissue envelope is critical to prevent skin necrosis and ensure optimal wound healing.
- Incision Planning: Create a dorsal elliptical incision centered directly over the PIP joint. The ellipse should measure approximately 5 to 6 mm in width to excise redundant skin and the associated hyperkeratotic lesion. Extend the incision 2 to 3 mm laterally on either side to provide adequate exposure of the collateral ligaments.

FIGURE 83-16 B: Dorsal elliptical incision planned over the proximal interphalangeal joint.
- Superficial Dissection: Excise the elliptical island of skin. It is imperative to remove only the skin initially. Carefully dissect through the subcutaneous tissue, identifying and preserving the dorsal venous network where possible. Cauterize small crossing vessels to maintain a bloodless field.

FIGURE 83-16 C: Superficial dissection demonstrating the preservation of dorsal veins, making targeted cauterization easier and minimizing postoperative edema.
2. Extensor Tendon and Capsular Management
- Tendon Resection: Excise a slightly smaller segment of the underlying extensor tendon and the dorsal capsule of the PIP joint.
- Preserving the Distal Stump: It is crucial to leave a 2-mm remnant of the extensor tendon attached to the dorsal base of the middle phalanx. This stump will serve as a critical anchor point during the final closure.
- Proximal Retraction: The proximal end of the transected extensor tendon will naturally retract beneath the proximal skin flap. Do not aggressively chase it at this stage; it can be easily retrieved distally during the closure phase.
3. Joint Exposure and Ligamentous Release
Achieving adequate exposure of the proximal phalangeal head requires a systematic release of the collateral ligaments.
- Positioning for Release: Flex the PIP joint to approximately 20 degrees while applying longitudinal traction to the distal and middle phalanges.
- Collateral Ligament Sectioning: Using a small-blade knife (e.g., a #15 blade), section the collateral ligaments from outside in on both the medial and lateral sides of the joint. Place the blade between the skin and the ligament, turning the cutting edge inward toward the joint space.
Surgical Warning: Keep the blade strictly within the confines of the joint capsule to avoid inadvertent injury to the plantar neurovascular bundles, which run immediately plantar and lateral to the collateral ligaments.
- Acute Flexion: Once the collateral ligaments and dorsal capsule are completely sectioned, the PIP joint can be acutely flexed to 90 degrees. This maneuver delivers the head and neck of the proximal phalanx directly into the surgical wound.

FIGURE 83-16 D: The dorsal capsule, both collateral ligaments, and the extensor tendon are sectioned transversely, allowing the toe to be acutely flexed.
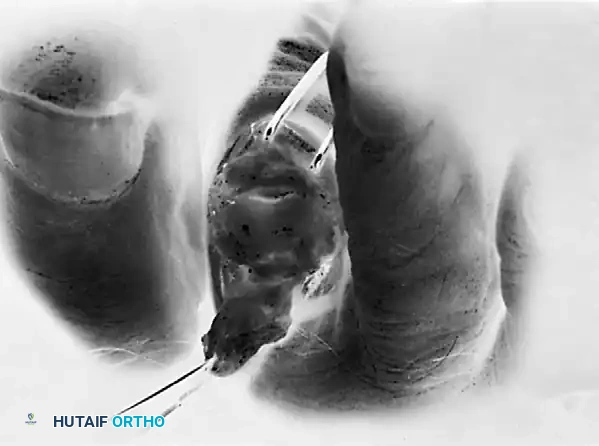
FIGURE 83-16 E: The extensor tendon is dissected proximally to the junction of the middle and distal thirds of the proximal phalanx, fully exposing the osseous anatomy.
4. Osseous Resection (Condylectomy)
The goal of the bone resection is to decompress the joint sufficiently to allow the toe to rest in a neutral alignment without soft tissue tension.
- Bone Removal: Using a sharp rongeur or a small-blade power sagittal saw, resect the head and neck of the proximal phalanx. Typically, the distal 25% to 30% of the proximal phalanx is excised.
- Contouring: Smooth any sharp cortical edges or bony prominences with a rasp or rongeur. A smooth, flat surface prevents postoperative irritation and allows the middle phalanx to rest flush against the proximal phalangeal remnant.
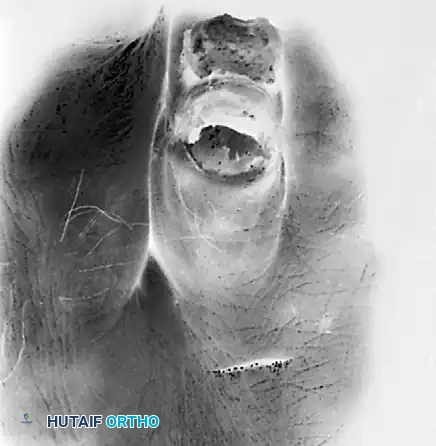
FIGURE 83-16 F: The distal 25% to 30% of the proximal phalanx is excised, allowing it to rest congruently on the middle phalanx. Note the small dorsal incision proximally for the adjunctive extensor tenotomy.
- Assessing Tension: Extend the toe to a neutral position at the PIP joint. Palpate the joint space to feel for tightness or abutment between the articular surface of the middle phalanx and the resected end of the proximal phalanx.
- Refining the Resection: If the joint feels tight or if the toe springs back into flexion, remove an additional 2 to 3 mm of bone. Inadequate bone resection is a primary cause of recurrent deformity.
5. Adjunctive Soft Tissue Balancing at the MTP Joint
In moderate hammer toe deformities, addressing the PIP joint alone may be insufficient if there is residual extensor tightness at the MTP joint.
- Evaluating MTP Extension: Hold the patient's ankle in a neutral (90-degree) position. If the MTP joint rests in hyperextension, an extensor tenotomy is indicated.
- Percutaneous EDL Tenotomy: Perform a percutaneous tenotomy of the extensor digitorum longus (EDL) over the neck of the metatarsal. Carefully avoid the dorsal veins.
- Stretching the Contracture: Following the tenotomy, acutely flex the toe at least 60 to 70 degrees at the MTP joint. This stretches the contracted dorsal capsule and allows the MTP joint to rest in a neutral position while the ankle is at neutral.
- EDB Tenotomy: Occasionally, the extensor digitorum brevis (EDB) tendon also contributes to the deformity. The EDB tendon is located immediately lateral and slightly plantarward to the EDL at the level of the metatarsal neck and should be sectioned if tight.
6. Wound Closure and Dynamic Tenodesis
The closure technique is not merely for skin approximation; it acts as a dynamic tenodesis to maintain the correction and provide a slight, functional degree of flexion.
- Suture Technique: Utilize a 3-0 or 4-0 nonabsorbable suture (e.g., Nylon or Prolene).
- The Core Stitch:
- Enter the proximal skin edge.
- Pass the needle through the proximal stump of the extensor tendon (retrieving it from beneath the skin flap).
- Enter the distal remnant of the extensor tendon (the 2-mm stump attached to the middle phalanx) from its joint surface.
- Exit through the distal skin edge.
- Correcting Lateral Deviation: By slightly canting (angling) this core stitch, a few degrees of mild lateral or medial deviation can be simultaneously corrected.
- Finalizing Closure: Tie the core stitch with the toe held in the desired alignment. Suture the medial and lateral corners of the wound with simple interrupted stitches. An initial mattress stitch can be utilized if the skin edges tend to invert.
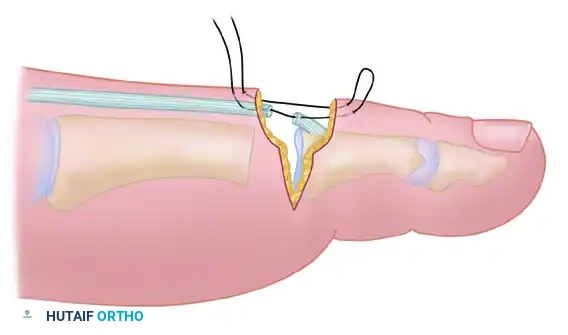
FIGURE 83-16 G: Final closure of the wound. The specialized suturing technique acts as a dorsal tension band, holding the PIP joint in acceptable alignment with only a few degrees of functional flexion.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The success of a PIP resection arthroplasty relies heavily on meticulous postoperative splinting. Because internal fixation (such as a Kirschner wire) is often omitted in this specific technique, the external dressing serves as the primary stabilizing force.
The Postoperative Dressing
Surgical Pitfall: A loose or poorly applied dressing will inevitably lead to loss of correction and recurrent deformity. The dressing must be conforming, binding, and structurally sound.
- Application: Use a soft dressing, such as 2-inch conforming gauze, to wrap the forefoot. Use 1/2-inch tape to secure the operated toe in the exact desired position, often buddy-taping it to an adjacent, stable toe.
- K-Wire Contingency: If the dressing is deemed insufficient to hold the toe in perfect alignment, the surgeon must have a low threshold to percutaneously drive a 0.045-inch or 0.062-inch Kirschner wire across the DIP and PIP joints for rigid stabilization.

FIGURE 83-17: The postoperative dressing must be conforming and binding enough to hold the toe in the exact corrected position. If stability is questionable, a Kirschner wire should be utilized.
Weight-Bearing and Recovery Timeline
- 0 to 72 Hours: Strict elevation of the foot above heart level to minimize edema and prevent wound dehiscence. Weight-bearing to tolerance is permitted strictly in a rigid, wooden-soled postoperative shoe.
- 12 to 16 Days: The patient returns to the clinic for suture removal. The toe is carefully reassessed, and a new conforming dressing is applied to maintain the corrected position for an additional 2 weeks.
- 4 Weeks: The wooden-soled shoe is typically discontinued. The dressing and taping can usually be removed at this stage.
- Extended Taping: If the deformity exhibits any tendency to recur or if the soft tissues remain lax, buddy taping should be continued for an additional 2 to 4 weeks.
Expected Outcomes
When executed correctly, this technique yields a stable PIP joint that retains a few degrees of active motion. Clinically, a toe that is gently flexed and compliant is far more pleasing to the patient—and accommodates footwear much better—than a rigidly fused, perfectly straight toe that may abut the toe box of a shoe.
MANAGEMENT OF SEVERE DEFORMITIES
While the aforementioned technique is highly effective for moderate deformities, severe, long-standing contractures—particularly those involving multi-planar instability such as crossover toes—require a more aggressive surgical algorithm.
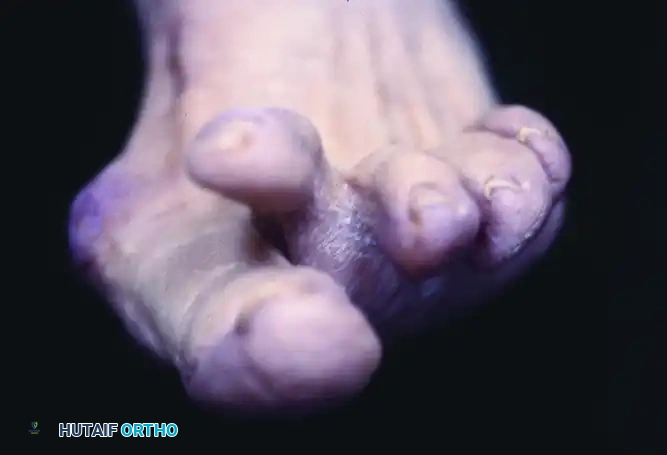
FIGURE 83-18: A severe crossover hammer toe deformity. Such complex presentations often require extensive soft tissue releases, flexor-to-extensor tendon transfers (Girdlestone-Taylor procedure), and rigid internal fixation.
In cases of severe crossover deformity, the plantar plate is often attenuated or ruptured, and the collateral ligaments are severely contracted asymmetrically. These cases necessitate formal MTP joint arthrotomy, extensive sequential releases, potential metatarsal shortening osteotomies (Weil osteotomy), and prolonged K-wire fixation to restore the transverse and sagittal plane alignment.
CONCLUSION
The operative correction of moderate hammer and claw toe deformities via PIP joint resection arthroplasty is a highly reliable procedure when precise surgical principles are followed. Success hinges on adequate osseous resection to decompress the joint, meticulous soft tissue balancing at the MTP level, and rigorous postoperative splinting. By adhering to this evidence-based approach, orthopedic surgeons can reliably restore forefoot biomechanics, alleviate pain, and achieve excellent long-term functional outcomes for their patients.
