Comprehensive Introduction and Patho-Epidemiology
Lesser toe deformities, encompassing hammer toe, claw toe, and mallet toe variants, are among the most ubiquitous forefoot pathologies encountered by the orthopaedic foot and ankle surgeon. While frequently conflated in generalized clinical parlance, these deformities represent highly distinct pathoanatomical entities with unique biomechanical etiologies, requiring highly specific surgical algorithms. A profound, nuanced understanding of the delicate equilibrium between intrinsic and extrinsic musculature, complex joint kinematics, and the dynamic flexibility of the deformity is paramount for selecting the appropriate surgical intervention and avoiding debilitating postoperative complications. The primary objective of surgical intervention is the restoration of a plantigrade, dynamically stable, and pain-free forefoot capable of accommodating standard footwear without focal pressure points.
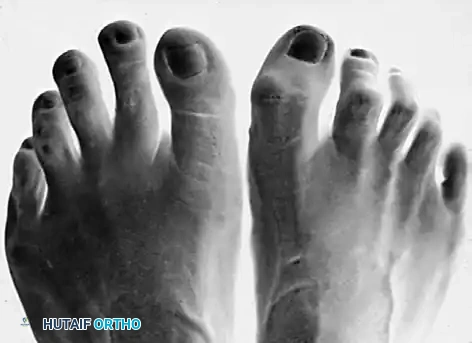
The precise nomenclature of these deformities dictates the anatomical focus of the reconstructive effort. A true hammer toe is defined by an abnormal, rigid, or flexible flexion posture isolated primarily to the proximal interphalangeal (PIP) joint. In a classic hammer toe presentation, the metatarsophalangeal (MTP) joint and the distal interphalangeal (DIP) joint may remain relatively flexible, resting in a neutral or slightly hyperextended position depending on the chronicity of the condition. Conversely, a claw toe is characterized by a more insidious, complex multi-joint deformity involving primary hyperextension of the MTP joint inextricably combined with secondary flexion contractures of both the PIP and DIP joints. A mallet toe, less common but equally problematic, involves an isolated flexion deformity of the DIP joint with neutral alignment of the PIP and MTP joints.

The epidemiology of lesser toe deformities demonstrates a strong predilection for the female demographic, largely attributed to the prolonged use of constrictive, narrow toe-box footwear and high-heeled shoes that force the MTP joints into prolonged hyperextension while simultaneously crowding the phalanges. However, the patho-epidemiology extends far beyond mere extrinsic compression. Claw toe deformities are classically driven by an intrinsic-minus state, often secondary to underlying neurologic conditions such as Charcot-Marie-Tooth disease, diabetic peripheral neuropathy, or direct trauma to the medial and lateral plantar nerves. In this intrinsic-minus model, the loss of lumbrical and interosseous function eliminates the primary flexors of the MTP joint and extensors of the interphalangeal joints, allowing the powerful extrinsic muscles (extensor digitorum longus [EDL] and flexor digitorum longus [FDL]) to run unchecked, driving the toe into the classic clawed posture. Conversely, isolated hammer toes frequently present without an identifiable neurologic deficit, driven instead by anatomical variants such as a long second ray, advanced hallux valgus causing under-riding or over-riding mechanical pressure, or inflammatory arthropathies that attenuate the plantar plate and collateral ligament complexes.
Detailed Surgical Anatomy and Biomechanics
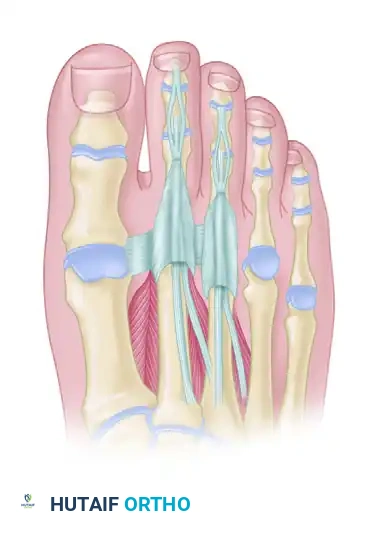
The structural stability and dynamic function of the lesser toes rely on an exquisitely delicate equilibrium between the osseous architecture, the capsuloligamentous restraints, and the dynamic interplay of the extrinsic and intrinsic musculature. The osseous anatomy comprises the metatarsal head, which articulates with the concave base of the proximal phalanx. The MTP joint is a condyloid joint, inherently unstable in the sagittal plane if not for the robust plantar plate—a thick, fibrocartilaginous structure originating from the metatarsal neck and inserting firmly onto the plantar base of the proximal phalanx. The plantar plate is the primary static stabilizer against MTP joint hyperextension. The collateral ligaments, originating from the dorsal-lateral aspects of the metatarsal head and inserting into the plantar-lateral bases of the proximal phalanx and the plantar plate itself, provide crucial coronal and transverse plane stability.
The musculotendinous anatomy is characterized by the complex extensor hood mechanism, which dictates the posture of the entire ray. The EDL tendon courses dorsally, splitting into a central slip that inserts on the base of the middle phalanx and two lateral slips that converge to insert on the base of the distal phalanx. The extensor digitorum brevis (EDB) joins the EDL lateral to the second, third, and fourth toes. The intrinsic muscles—the lumbricals and interossei—are the critical modulators of this system. The lumbricals course plantar to the deep transverse metatarsal ligament, placing their axis of pull plantar to the MTP joint (acting as flexors) before coursing dorsally to insert into the medial aspect of the extensor wing, thereby acting as extensors of the PIP and DIP joints. The interossei course dorsal to the deep transverse metatarsal ligament, contributing to abduction/adduction and assisting in MTP flexion and IP extension.

Biomechanically, the pathogenesis of claw and hammer toes can be understood through the concepts of flexor stabilization, flexor substitution, and extensor substitution. Flexor stabilization is the most common etiology, occurring in a flexible pes planovalgus foot where the FDL fires early and longer during the stance phase to stabilize the hypermobile forefoot, overpowering the interossei and driving the IP joints into flexion. Extensor substitution occurs during the swing phase in patients with cavus foot types or anterior compartment weakness; the EDL over-activates to assist in ankle dorsiflexion, aggressively hyperextending the MTP joints. Flexor substitution is the least common, occurring when the triceps surae is weak, and the deep posterior compartment muscles (FDL, FHL, tibialis posterior) attempt to substitute for heel lift, causing late-stance toe gripping. Understanding these specific dynamic imbalances is critical, as failure to address the underlying biomechanical driver will inevitably lead to surgical failure and deformity recurrence.

Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for lesser toe deformities must be predicated on a thorough clinical evaluation, failure of comprehensive conservative management, and a clear understanding of the patient's functional demands and physiological limitations. Surgery is rarely indicated for purely cosmetic reasons, as the inherent risks of lesser toe reconstruction—including stiffness, floating toe, and vascular compromise—outweigh aesthetic benefits. The primary indication for surgical correction is persistent, debilitating pain that limits the patient's activities of daily living and has proven refractory to non-operative measures such as wide toe-box footwear, custom orthoses with metatarsal offloading pads, crest pads, and judicious corticosteroid injections for localized synovitis.
Specific surgical indications include the presence of intractable plantar keratoses (IPK) secondary to MTP joint hyperextension, painful dorsal heloma durum (corns) over the PIP or DIP joints that ulcerate or become recurrently inflamed, and progressive deformity that threatens to cross over or under adjacent digits, thereby disrupting the global biomechanics of the forefoot. In the diabetic or neuropathic population, a rigid hammer or claw toe that has led to pre-ulcerative lesions or recalcitrant ulcerations is an urgent indication for prophylactic surgical correction to avert deep space infection, osteomyelitis, and subsequent amputation. The surgeon must carefully weigh the flexibility of the deformity, as this dictates the invasiveness of the procedure; flexible deformities may be managed with soft-tissue rebalancing, whereas rigid, fixed contractures mandate osseous resection, osteotomy, or arthrodesis.
Contraindications to lesser toe surgery must be rigorously respected to prevent catastrophic ischemic complications. The most absolute contraindication is inadequate vascular perfusion. A comprehensive vascular assessment is mandatory; absent palpable pedal pulses necessitate non-invasive arterial studies. An Ankle-Brachial Index (ABI) of less than 0.5, or absolute toe pressures below 40 mm Hg, generally preclude elective forefoot surgery due to the unacceptably high risk of postoperative necrosis and failure of wound healing. Active localized or systemic infection, severe uncontrolled diabetes mellitus (HbA1c > 8.5%), and profound medical comorbidities that prohibit safe anesthesia are also absolute contraindications. Relative contraindications include heavy tobacco use, which significantly impairs microvascular perfusion and bone healing, and severe, unmanageable psychiatric or cognitive disorders that would prevent strict adherence to postoperative weight-bearing and splinting protocols.
| Category | Indications for Surgical Intervention | Contraindications (Absolute and Relative) |
|---|---|---|
| Clinical Presentation | Painful, fixed, or progressive deformity refractory to shoe modification. | Asymptomatic deformity (cosmetic concerns only). |
| Dermatological | Recurrent dorsal heloma durum, apical ulcerations, intractable plantar keratoses (IPK). | Active, untreated local bacterial or fungal infection. |
| Vascular Status | Adequate perfusion (Palpable pulses, ABI > 0.9, Toe pressure > 40 mmHg). | Absolute: Severe peripheral arterial disease (ABI < 0.5). |
| Neurological | Neuropathic ulceration risk mitigation (prophylactic correction). | Relative: Severe Charcot neuroarthropathy in acute phase. |
| Biomechanical | Cross-over toe deformity, MTP joint dislocation, severe plantar plate rupture. | Inability to comply with postoperative offloading/splinting. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning begins with a meticulous, systematic physical examination designed to isolate the specific anatomical drivers of the deformity and assess the flexibility of each joint in the affected ray. The surgeon must evaluate the MTP, PIP, and DIP joints independently. The Kelikian push-up test is the cornerstone of this evaluation: firm pressure is applied to the plantar aspect of the metatarsal head, simulating the ground reaction forces of the stance phase of gait. If the PIP and DIP joints straighten and the MTP joint reduces to a neutral alignment, the deformity is deemed flexible, and soft-tissue procedures (such as a flexor-to-extensor transfer or EDL lengthening) may suffice. If the deformity persists despite plantar pressure, it is classified as rigid or fixed, necessitating osseous intervention such as a PIP resection arthroplasty, PIP arthrodesis, or a metatarsal shortening osteotomy.

Evaluating the stability of the MTP joint is equally critical. The Lachman test (dorsal-plantar drawer test) of the MTP joint assesses the integrity of the plantar plate and collateral ligaments. A positive drawer test, characterized by dorsal translation of the proximal phalanx on the metatarsal head without a firm endpoint, indicates plantar plate attenuation or rupture. Furthermore, the surgeon must differentiate between an interdigital (Morton's) neuroma and idiopathic synovitis or plantar plate pathology, as these frequently present with overlapping symptoms of forefoot pain. Neuroma pain is typically localized to the interdigital web space and is exacerbated by lateral compression of the forefoot (Mulder's click), whereas synovitis or plantar plate tears present with pinpoint tenderness directly over the MTP joint capsule, particularly the dorsofibular aspect, and pain exacerbated by forced passive MTP hyperextension.
Radiographic evaluation requires standard weight-bearing anteroposterior (AP), lateral, and oblique views of the foot. The AP view is scrutinized for MTP joint congruency, subluxation, or frank dislocation, as well as the relative lengths of the metatarsals (the metatarsal parabola). A severely long second metatarsal is a frequent culprit in second MTP joint instability and cross-over toe deformities, often necessitating a Weil shortening osteotomy. The lateral view helps quantify the degree of dorsal MTP subluxation and the severity of the PIP and DIP flexion contractures. Patient positioning for lesser toe reconstruction is typically supine, with a bump placed under the ipsilateral hip to internally rotate the leg to a neutral position, ensuring the toes point directly toward the ceiling. A calf or thigh tourniquet is utilized to provide a bloodless surgical field, though it must be deflated prior to final closure if there is any concern regarding the vascular viability of the reconstructed digits.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution for correcting lesser toe deformities must be systematic, addressing the pathology from proximal to distal, or distal to proximal, depending on the surgeon's preference, but always ensuring that both the osseous and soft-tissue components are fully rebalanced. For a rigid hammer toe with an associated MTP joint contracture, a combined approach utilizing a PIP joint resection arthroplasty (or arthrodesis) alongside an MTP joint soft-tissue release and potential Weil osteotomy is the gold standard. The procedure begins with a dorsal longitudinal incision extending from the distal aspect of the metatarsal head to the distal interphalangeal joint. This approach allows comprehensive access to the MTP, PIP, and the extensor mechanism while safely navigating between the dorsal neurovascular bundles, which must be meticulously retracted medially and laterally.
For the correction of the fixed PIP flexion contracture, the extensor tendon is identified and a transverse tenotomy or a Z-lengthening is performed over the PIP joint. A thorough collateral ligament release and dorsal capsulotomy are executed to fully expose the head and neck of the proximal phalanx. Using a microsaw or a sharp bone rongeur, the distal articular cartilage and the condyles of the proximal phalanx are resected perpendicular to the long axis of the bone (the DuVries technique). If an arthrodesis is planned, the base of the middle phalanx is also denuded of cartilage to expose bleeding subchondral bone. The osteotomy site is then reduced. The surgeon must ensure that the bone resection is sufficient to allow the toe to rest in a neutral, rectus alignment without any residual tension on the neurovascular bundles.
Attention is then directed to the MTP joint. If a rigid hyperextension deformity exists, a stepwise soft-tissue release is performed: first, a dorsal capsulotomy; second, an EDL Z-lengthening; third, release of the collateral ligaments. If the MTP joint remains subluxated or the metatarsal is excessively long, a Weil osteotomy is indicated. The metatarsal head is exposed, and a microsaw is used to create an osteotomy parallel to the plantar aspect of the foot (typically angled 10 to 15 degrees plantar-proximal to dorsal-distal to prevent plantar depression of the metatarsal head). The capital fragment is shifted proximally 2 to 5 mm to decompress the joint and is fixed with a single, countersunk twist-off screw or a headed compression screw. Finally, the entire ray is stabilized. While modern intramedullary implants (e.g., shape-memory nitinol staples or PEEK implants) are gaining popularity for PIP arthrodesis, the traditional and highly reliable method involves driving a 1.1-mm (0.045-inch) Kirschner wire (K-wire) antegrade from the PIP joint out through the tip of the toe, and then retrograde across the PIP joint, the MTP joint, and into the metatarsal shaft to maintain the corrected alignment during the initial 4 to 6 weeks of soft-tissue healing.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, lesser toe reconstruction carries a distinct profile of complications that the orthopaedic surgeon must be prepared to anticipate and manage. One of the most frustrating and functionally limiting complications is the "floating toe" deformity, characterized by the toe's inability to purchase the ground during the stance phase of gait. This occurs in up to 10-15% of cases and is typically the result of over-resection of the proximal phalanx, excessive dorsal MTP joint release, over-shortening of a Weil osteotomy (which alters the intrinsic muscle mechanics), or failure to adequately repair or address a deficient plantar plate. Salvage of a symptomatic floating toe is complex and may require a flexor-to-extensor tendon transfer to restore plantarflexion power, or a revision bone block arthrodesis to restore digital length and tension the intrinsic musculature.
Vascular compromise is the most catastrophic immediate postoperative complication. Aggressive correction of a severe, chronic, rigid deformity can acutely stretch the digital neurovascular bundles, leading to severe arterial spasm, intimal tear, or thrombosis. The surgeon must meticulously assess capillary refill and the color of the digit immediately upon tourniquet deflation and prior to applying the final dressing. A "white toe" indicates arterial insufficiency, while a "blue toe" suggests venous congestion. If vascular compromise is noted, the immediate salvage protocol demands the removal of the K-wire to eliminate longitudinal tension, placing the toe in slight flexion, applying warm saline compresses to induce vasodilation, and potentially applying topical papaverine. If perfusion does not return within 15 to 20 minutes, all surgical sutures must be removed to decompress the soft tissues. If the toe ultimately undergoes necrosis, a delayed partial or complete ray amputation is required.
Recurrence of the deformity is another frequent complication, particularly in patients with underlying, unaddressed neurological deficits or severe intrinsic-minus foot types. Recurrence rates range from 5% to 20% in long-term follow-up studies. Recurrence is often due to inadequate initial bony resection, failure to recognize a concomitant equinus contracture that drives forefoot overload, or the use of isolated soft-tissue procedures in a semi-rigid deformity. Salvage management for recurrent deformities typically necessitates revision surgery utilizing more rigid fixation methods, such as formal PIP joint arthrodesis with intramedullary implants, combined with more aggressive soft-tissue rebalancing, such as a Girdlestone-Taylor flexor-to-extensor transfer. Pin tract infections associated with exposed K-wires occur in approximately 2-5% of cases; these are generally superficial and respond well to a short course of oral antibiotics and local wound care, though deep infections may necessitate premature pin removal.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Strategy / Management |
|---|---|---|---|
| Floating Toe | 10% - 15% | Over-resection of bone, Weil osteotomy over-shortening, missed plantar plate tear. | Flexor-to-extensor transfer, bone block lengthening, taping. |
| Recurrence | 5% - 20% | Inadequate bone resection, unaddressed equinus, intrinsic-minus state. | Revision arthrodesis, aggressive soft-tissue rebalancing. |
| Vascular Compromise | < 1% - 2% | Over-distraction of chronic deformity, tight closure, peripheral arterial disease. | Remove K-wire, flex toe, warm compresses, remove sutures. Amputation if necrotic. |
| Pin Tract Infection | 2% - 5% | Exposed K-wire, poor patient hygiene, prolonged pin retention. | Oral antibiotics, local chlorhexidine care, premature pin removal if deep. |
| Nonunion (Arthrodesis) | 5% - 10% | Inadequate bone preparation, early pin removal, smoking. | Often asymptomatic; if painful, revision arthrodesis with bone graft and rigid implant. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation phase is as critical as the surgical execution in ensuring a successful, long-term outcome. The protocol is designed to protect the osseous reconstruction, allow for secure soft-tissue healing of the capsuloligamentous structures, and prevent the dreaded dorsal contracture that leads to a floating toe. Phase 1 (Weeks 0 to 2) focuses on strict immobilization and edema control. Immediately postoperatively, the surgical site is dressed with sterile, non-adherent gauze, and a compressive forefoot wrap is applied. Crucially, the operated toe must be splinted in a neutral to slightly plantarflexed position. This is achieved through meticulous "buddy taping," where the reconstructed digit is strapped to the adjacent, stable toe (typically the hallux or the third toe) using multiple strips of 12-mm wide adhesive surgical tape. The patient is placed in a rigid, stiff-soled postoperative shoe or a controlled ankle motion (CAM) boot. Weight-bearing is typically restricted to heel-weight-bearing or flat-foot weight-bearing, strictly avoiding any toe-off forces that could bend or break the K-wire or disrupt the osteotomy.
Phase 2 (Weeks 2 to 6) marks the transition from acute healing to early mobilization. At the 2-week postoperative visit, sutures are removed, assuming the incisions are fully healed. If a K-wire was utilized and left protruding, pin site care is meticulously reviewed with the patient to prevent superficial infections. The buddy taping is reapplied and must be maintained continuously. Patients are permitted to increase their weight-bearing status in the stiff-soled shoe as tolerated, but propulsive gait remains strictly prohibited. Between weeks 4 and 6, the K-wire is removed in the clinical setting. This is a critical juncture; once the pin is removed, the MTP joint is susceptible to dorsal contracture. Therefore, the patient is instructed to begin active and passive plantarflexion exercises of the MTP joint immediately. The patient is taught to manually grasp the toe and firmly stretch it into plantarflexion multiple times a day to maintain the excursion of the extensor tendons and prevent dorsal capsular scarring.
Phase 3 (Weeks 6 and beyond) focuses on the return to normal function and footwear. Radiographs are obtained to confirm the consolidation of any osteotomies or arthrodeses. Patients are gradually transitioned out of the postoperative shoe and into a supportive, wide toe-box athletic shoe with a rigid shank. Buddy taping is often continued during daytime weight-bearing activities for an additional 2 to 4 weeks to provide dynamic splinting while the intrinsic musculature rehabilitates. High-impact activities, running, and the use of narrow or high-heeled footwear are generally restricted until at least 10 to 12 weeks postoperatively. The surgeon must counsel the patient that mild to moderate edema of the reconstructed digit (the "sausage toe") is a normal physiological response to forefoot surgery and may persist for 4 to 6 months before completely resolving.
Summary of Landmark Literature and Clinical Guidelines
The surgical management of lesser toe deformities has evolved significantly over the past several decades, guided by landmark biomechanical studies and rigorous clinical outcome trials. The foundational understanding of forefoot biomechanics and the intrinsic-minus foot was heavily influenced by the early works of Coughlin and Myerson, who meticulously detailed the pathophysiology of crossover toe deformities and the critical stabilizing role of the plantar plate. Their anatomical dissections and clinical series established the modern paradigm that isolated PIP joint procedures are destined to fail if concomitant MTP joint instability and hyperextension are not simultaneously addressed. This literature underscores the absolute necessity of the Lachman drawer test in the preoperative evaluation and the routine incorporation of plantar plate repairs or flexor-to-extensor transfers in the surgical algorithm.
The management of the MTP joint in the setting of severe clawing or subluxation was revolutionized by the introduction and popularization of the Weil osteotomy. Originally described by L.S. Weil and later extensively studied and modified by Barouk, the Weil osteotomy provides controlled, reliable shortening of the metatarsal, thereby decompressing the MTP joint and relaxing the contracted extrinsic extensor musculature without altering the metatarsal head's plantar articular surface. Landmark outcome studies have demonstrated that the Weil osteotomy, when combined with PIP joint arthrodesis, yields high patient satisfaction rates and reliably restores the metatarsal parabola. However, subsequent literature by Trnka et al. highlighted the biomechanical pitfall of the Weil osteotomy: the proximal shift of the capital fragment alters the axis of the interossei, converting them from flexors to extensors of the MTP joint, which is the primary driver of the postoperative floating toe complication. This has led to the modern clinical guideline recommending the removal of a dorsal parallel slice of bone during the Weil osteotomy to prevent plantar displacement of the metatarsal head, or the concurrent execution of a flexor-to-extensor transfer.
Recent literature has heavily debated the optimal fixation method for PIP joint arthrodesis. While the traditional intramedullary K-wire remains the most cost-effective and widely utilized method, retrospective cohorts and prospective randomized trials have increasingly scrutinized its complication profile, specifically regarding pin tract infections, patient discomfort, and the risk of pin migration or breakage. The advent of intramedullary shape-memory nitinol staples and radiolucent PEEK implants has provided an alternative that eliminates exposed hardware and potentially offers dynamic compression across the arthrodesis site. Recent meta-analyses comparing K-wires to modern intramedullary devices suggest that while fusion rates and final clinical alignment are comparable, intramedullary implants offer higher early patient satisfaction scores and eliminate pin-related complications, albeit at a significantly higher implant cost. Current clinical guidelines suggest that the choice of fixation should be tailored to the patient's specific anatomy, compliance level, and the surgeon's familiarity with the implant systems, maintaining that meticulous soft-tissue balancing remains the ultimate determinant of surgical success.
