Comprehensive Introduction and Patho-Epidemiology
Biceps tendon lesions and superior labrum anterior-posterior (SLAP) tears represent a highly complex and frequently overlapping continuum of shoulder pathology. These entities may be inflammatory, degenerative, or traumatic in origin, and they require a nuanced understanding of glenohumeral kinematics for accurate diagnosis and management. The pathological cascade can affect multiple distinct but biomechanically linked anatomical sites, including the attachment to the supraglenoid tubercle, the SLAP complex, the tendon proper (both intraarticular and extraarticular segments), and the stabilizing bicipital arch. Historically, the long head of the biceps tendon (LHBT) was viewed merely as a vestigial structure; however, contemporary orthopedic science recognizes its critical role as a dynamic depressor of the humeral head and an anterior stabilizer of the glenohumeral joint, particularly in positions of vulnerability such as extreme abduction and external rotation.
Epidemiologically, the presentation of biceps and SLAP pathology is distinctly bimodal. In the younger, highly active demographic—specifically overhead athletes such as baseball pitchers, tennis players, and volleyball attackers—these lesions frequently result from repetitive microtrauma. The extreme torsional forces generated during the late cocking and early acceleration phases of the throwing motion place unprecedented stress on the biceps anchor. Conversely, in the older population (typically patients over the age of 40 to 50), biceps pathology is almost universally degenerative and intimately associated with rotator cuff disease. In this cohort, chronic impingement, diminished vascularity in the critical zone of the tendon, and progressive failure of the rotator interval structures lead to tendinosis, partial tearing, and eventual subluxation or rupture of the LHBT.
The concept of the "hourglass" biceps deformity, robustly described by Boileau et al., further illustrates the chronic degenerative cascade. This morphological alteration is characterized by chronic inflammation, intraarticular hypertrophy, and mechanical triggering of the enlarged tendon as it attempts to glide through the unyielding proximal bicipital groove during joint motion. The persistence of this mechanical triggering inevitably results in pulley instability, structural failure of the stabilizing ligaments, and profound anterior shoulder pain. Recognizing this bimodal distribution and the differing underlying patho-anatomical mechanisms is absolutely critical for the orthopedic surgeon, as it dictates a divergent algorithmic approach to surgical intervention, heavily influencing the decision between labral repair, biceps tenodesis, and simple tenotomy.
Furthermore, dynamic arthroscopic evaluation has revolutionized our understanding of the prevalence of these lesions. Lafosse et al. demonstrated in a landmark study of 200 consecutive patients undergoing arthroscopic rotator cuff repair that 45% exhibited anterior, posterior, or combined biceps instability. Crucially, larger rotator cuff tears directly correlated with a higher incidence and severity of biceps instability. Failure to recognize and address this occult biceps instability during concomitant cuff repair remains one of the primary etiologies of persistent, debilitating postoperative pain. Therefore, a comprehensive understanding of both the epidemiology and the progressive patho-anatomy is the foundational prerequisite for successful surgical management.
Detailed Surgical Anatomy and Biomechanics
The bicipital arch is a critical, highly specialized anatomical conglomerate responsible for the stabilization of the LHBT as it exits the glenohumeral joint and enters the intertubercular groove. This arch is not a simple osseous tunnel but rather a dynamic, soft-tissue sling composed of the superior glenohumeral ligament (SGHL) and the coracohumeral ligament (CHL). These structures converge at the superior aspect of the bicipital groove. This ligamentous sling is dynamically and statically reinforced anteriorly by the superior fibers of the subscapularis tendon and posteriorly by the leading edge of the supraspinatus tendon. Disruption of this intricate arch leads to medial subluxation or frank dislocation of the biceps tendon, a condition that is rarely isolated and almost invariably accompanied by significant rotator cuff pathology.
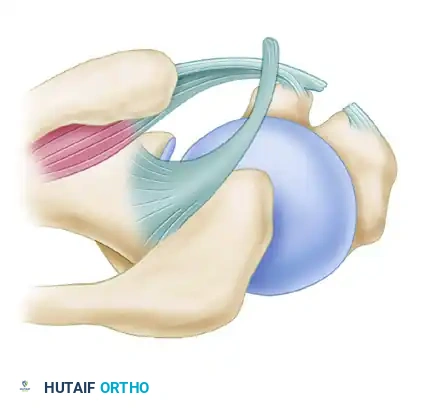
Figure 1: Normal anatomy of the bicipital arch and rotator interval.
Biceps instability is classified based on the progressive structural failure of this pulley system and the specific involvement of adjacent rotator cuff tendons. A deep understanding of this classification is paramount for preoperative planning and intraoperative decision-making.
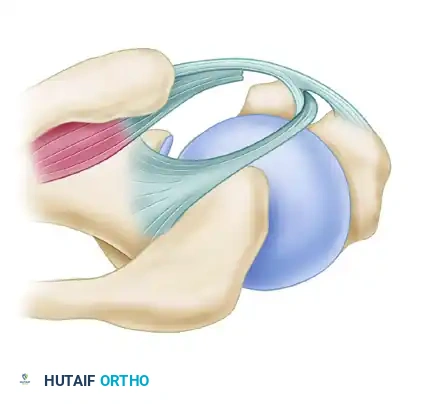
Figure 2: Type 1 Instability. Characterized by tears of the subscapularis without involvement of the medial head of the coracohumeral ligament.
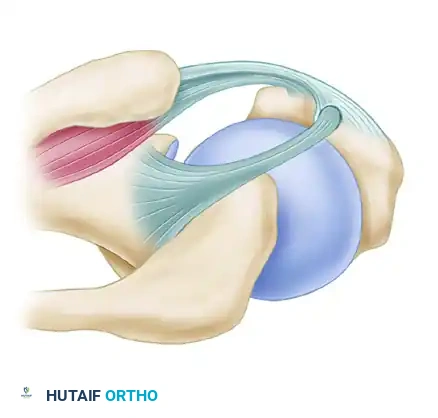
Figure 3: Type 2 Instability. Occurs without tears of the subscapularis but involves the medial head of the coracohumeral ligament.
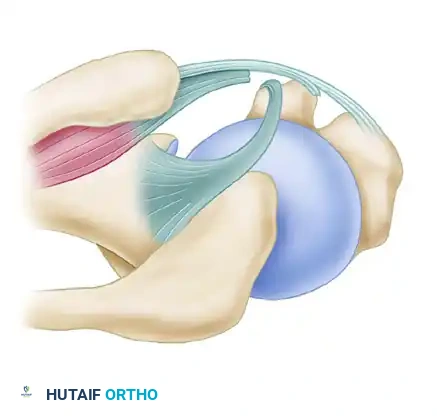
Figure 4: Type 3 Instability. Involves tears of the subscapularis combined with involvement of the medial head of the coracohumeral ligament.
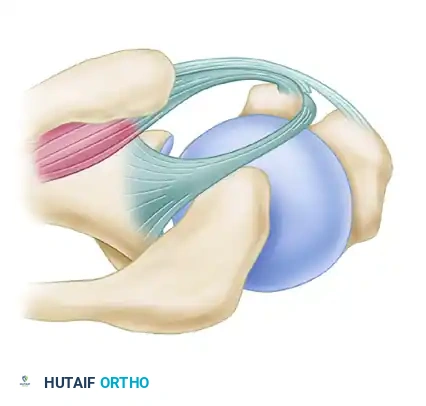
Figure 5: Type 4 Instability. Characterized by tears of the supraspinatus and the lateral head of the coracohumeral ligament.
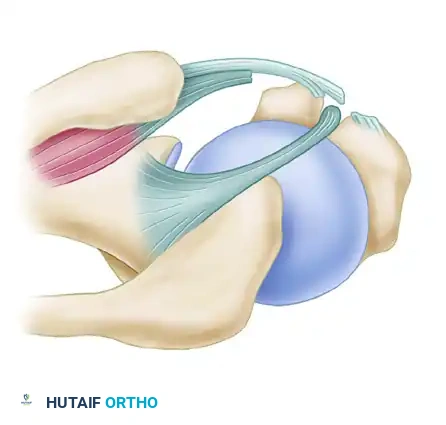
Figure 6: Type 5 Instability. A massive disruption involving tears of the subscapularis, both the medial and lateral heads of the coracohumeral ligament, and the leading edge of the supraspinatus tendon.
Biomechanically, the pathogenesis of SLAP lesions in the overhead athlete is intimately tied to the "peel-back" mechanism. During the late cocking phase of throwing, the shoulder is placed in a position of extreme abduction and maximal external rotation. In this precise position, the vector of the biceps tendon shifts dramatically posterior to the longitudinal axis of the humerus. If the posteroinferior capsule is contracted—a condition clinically recognized as glenohumeral internal rotation deficit (GIRD)—the humeral head is subjected to an obligate posterosuperior translation.
This posterosuperior shift acts as a fulcrum, twisting the base of the biceps tendon and transmitting a massive torsional, peel-back force directly to the superior labral anchor. Over time, this repetitive cyclic loading exceeds the tensile strength of the labral attachment to the supraglenoid tubercle, resulting in structural failure and a Type II SLAP tear. Neutralizing this specific torsional force is the primary biomechanical objective of surgical SLAP repair. A tight posteroinferior capsule is the primary initiator of this pathological cascade; thus, addressing capsular contracture through targeted rehabilitation or surgical release is just as critical as the anatomical repair of the labrum itself.
Exhaustive Indications and Contraindications
The surgical decision-making process for biceps tendon and SLAP lesions is highly complex and must be meticulously tailored to the patient's physiological age, functional demands, chronicity of symptoms, and concomitant glenohumeral pathology. The modern orthopedic paradigm has shifted significantly over the last decade, moving away from universal SLAP repairs in middle-aged patients toward a more aggressive utilization of biceps tenodesis. This shift is driven by outcome data demonstrating unacceptably high rates of postoperative stiffness and persistent pain following labral repairs in patients over the age of 35 to 40.
Arthroscopic SLAP repair is strictly indicated for young, highly active patients—specifically overhead athletes—who possess a morphologically healthy, robust biceps tendon but present with a mechanically detachable superior labrum (Type II or Type IV SLAP lesions). In this highly specific cohort, restoring the anatomical footprint of the superior labrum is essential to re-establish the critical tension of the superior glenohumeral ligament and the dynamic stabilizing effect of the biceps anchor. Conversely, SLAP repair is generally contraindicated in older patients, those with advanced degenerative joint disease, or those with significant morphological tearing or tendinosis of the LHBT itself. In these scenarios, repairing the labrum while leaving a diseased tendon in situ will almost certainly lead to clinical failure.
Biceps tenodesis has emerged as the workhorse procedure for a vast array of LHBT pathology. It is indicated for patients presenting with chronic subacromial impingement, persistent bicipital tendinitis refractory to conservative management, structural disruption exceeding 50% of the tendon's cross-sectional area, frank biceps subluxation (Types 1-5 instability), or the presence of an hourglass deformity. Tenodesis removes the diseased portion of the tendon from the joint and the unyielding bicipital groove while maintaining the length-tension relationship of the biceps muscle belly, thereby preserving supination strength and preventing the cosmetic "Popeye" deformity. Depending on surgeon preference and concomitant pathology, this can be performed high in the groove (suprapectoral) or low (subpectoral) using interference screws, cortical buttons, or suture anchors.
Biceps tenotomy is a highly effective, technically straightforward procedure indicated primarily for older patients (typically >55-60 years) with lower functional demands, massive irreparable rotator cuff tears, or those who do not perform heavy manual labor or require maximal supination torque. While concerns exist regarding cosmetic deformity and subjective cramping, extensive literature, including studies by Osbahr et al. and Walch et al., demonstrates exceptionally high satisfaction rates (up to 87%) and excellent pain relief with tenotomy. Poor outcomes following tenotomy are typically associated with preoperative high-riding humeri and advanced fatty infiltration of the rotator cuff, where the loss of the biceps' minimal head-depressing effect exacerbates superior escape.
| Surgical Intervention | Primary Indications | Relative/Absolute Contraindications | Biomechanical Objective |
|---|---|---|---|
| Arthroscopic SLAP Repair | Young overhead athletes (<35 yrs); Acute traumatic Type II/IV SLAP; Healthy LHBT tissue; Normal bicipital groove anatomy. | Age > 40 years; Degenerative labral fraying (Type I); Significant LHBT tendinosis; Concomitant advanced rotator cuff disease; Stiff shoulder (adhesive capsulitis). | Restore native superior labral footprint; Neutralize peel-back forces; Re-tension the SGHL/biceps anchor complex. |
| Biceps Tenodesis | Age 35-55 years; Active laborers; LHBT tearing >50%; Biceps subluxation/pulley lesions; Hourglass deformity; Failed SLAP repair. | Low-demand elderly patients; Massive irreparable cuff tears with superior escape (relative); Active local infection. | Eliminate intraarticular pathology and groove pain; Preserve length-tension relationship; Prevent cosmetic deformity. |
| Biceps Tenotomy | Age > 55-60 years; Low functional demands; Sedentary lifestyle; Massive irreparable cuff tears; Severe medical comorbidities precluding longer surgery. | Young active patients; Heavy laborers; Patients highly concerned with cosmetic appearance; Pre-existing severe cramping. | Rapid, definitive elimination of pain generated by the LHBT and bicipital groove; Minimal operative time. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning begins with a meticulous clinical examination. The diagnosis of SLAP and biceps lesions is notoriously difficult due to the lack of a single pathognomonic physical sign and the high incidence of concomitant shoulder pathology. A battery of provocative tests must be employed. O'Brien's active compression test, Speed's test, Yergason's test, and the dynamic shear test are routinely utilized. However, the surgeon must interpret these with caution, as their sensitivity and specificity are highly variable. The most reliable clinical indicator is often deep, poorly localized anterior shoulder pain that is exacerbated by overhead activities, combined with a positive peel-back sign elicited during dynamic examination.
Advanced imaging is mandatory for surgical templating. Magnetic Resonance Arthrography (MRA) remains the gold standard for evaluating the superior labral complex and the capsuloligamentous structures. The intraarticular gadolinium distends the joint, allowing for the visualization of contrast extending between the superior labrum and the glenoid rim. The surgeon must meticulously evaluate the axial, coronal, and sagittal oblique sequences. The ABER (abduction and external rotation) view is particularly sensitive for detecting posterosuperior labral tears and undersurface rotator cuff delamination. Preoperative templating should include an assessment of glenoid morphology, the presence of paralabral cysts (which may compress the suprascapular nerve and require decompression), and the exact degree of fatty infiltration of the rotator cuff muscles utilizing the Goutallier classification.
Patient positioning is a critical decision that influences visualization, traction, and the ease of specific surgical steps. Arthroscopic shoulder surgery can be performed in either the lateral decubitus or the beach chair position. For isolated SLAP repairs, the lateral decubitus position is heavily favored by many academic surgeons. This position utilizes dual-axis traction (longitudinal and lateral), which significantly distracts the glenohumeral joint, providing unparalleled visualization of the superior labrum and the posteroinferior capsule. The traction effectively opens the subacromial space and the joint, facilitating complex suture management and anchor placement.
Conversely, the beach chair position is often preferred when concomitant extraarticular procedures, such as an open subpectoral biceps tenodesis or a mini-open rotator cuff repair, are anticipated. The beach chair position provides an anatomical orientation that is highly intuitive, allows for unhindered rotation of the humerus throughout the procedure, and avoids the traction-related neurapraxias occasionally seen with the lateral decubitus position. Regardless of the chosen position, meticulous padding of all bony prominences and strict adherence to safe traction limits (typically less than 10-15 pounds) are absolute prerequisites to prevent catastrophic neurological complications. Hypotensive regional anesthesia, specifically an ultrasound-guided interscalene block combined with general anesthesia, is employed to minimize intraoperative bleeding, optimize visualization, and provide robust immediate postoperative analgesia.
Step-by-Step Surgical Approach and Fixation Technique
The execution of a mechanically effective SLAP repair demands meticulous attention to detail, precise portal placement, and advanced arthroscopic suturing skills. The overarching biomechanical goal is to neutralize the peel-back forces by positioning a tight suture loop just posterior to the root of the biceps, thereby securing the labrum to a meticulously prepared bleeding bone bed on the supraglenoid tubercle.
1. Diagnostic Arthroscopy and Portal Placement
The procedure commences with a comprehensive 15-point diagnostic arthroscopy through a standard posterior viewing portal. The surgeon must dynamically evaluate the biceps by internally and externally rotating the humerus in 0 to 30 degrees of abduction, followed by meticulous probing to evaluate static stability. The "drive-through" sign and the dynamic "peel-back" test are performed. A positive peel-back test confirms the mechanical instability of the superior labrum.
Standard posterior and anterior working portals are established. However, for superior labral lesions that extend posteriorly to overlie the posterosuperior quadrant, standard portals provide an inadequate angle of approach, leading to dangerous "skiving" of the drill on the glenoid rim. Therefore, a specialized posterolateral portal—the Portal of Wilmington—is absolutely required.
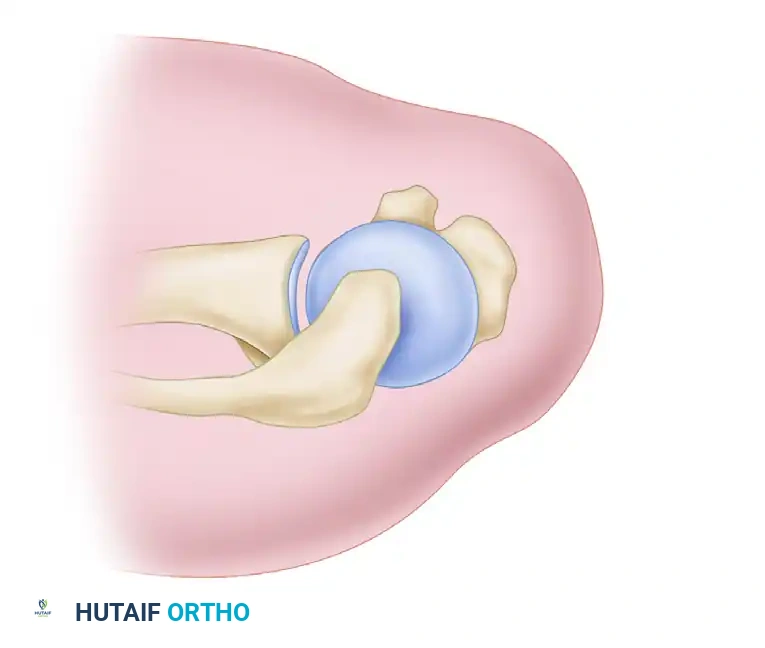
Figure 7: The Posterolateral Portal (Portal of Wilmington) is located 1 cm lateral and 1 cm anterior to the posterior acromial angle. It provides the optimal trajectory for anchor placement in the posterosuperior quadrant.
To minimize iatrogenic damage to the rotator cuff, a 3.5-mm Spear Guide is passed blindly but precisely through the musculotendinous junction of the infraspinatus. Because of its small diameter, the Spear Guide is vastly preferred over a standard 7-mm arthroscopy cannula for this specific approach, minimizing morbidity to the cuff tissue. This posterolateral portal is used strictly for percutaneous anchor placement; all subsequent suture passage and knot-tying for the posterior anchor are accomplished through the established anterosuperior cannula.
2. Footprint Preparation and Anchor Insertion
Healing of the labrum requires robust biological integration. The superior glenoid rim, specifically the footprint of the superior labrum beneath the biceps anchor, must be meticulously prepared. An arthroscopic rasp or a motorized burr is utilized to decorticate the bone, removing all fibrous tissue and cartilage until a bleeding, punctate cancellous bone bed is achieved. Care must be taken not to remove excessive bone, which could compromise anchor purchase.
Once the footprint is prepared, a double-loaded 3-mm suture anchor (or a modern knotless equivalent) is introduced through the Portal of Wilmington. The trajectory must be precisely 45 degrees to the articular surface to avoid penetrating the articular cartilage of the glenoid face or plunging dangerously into the suprascapular notch.
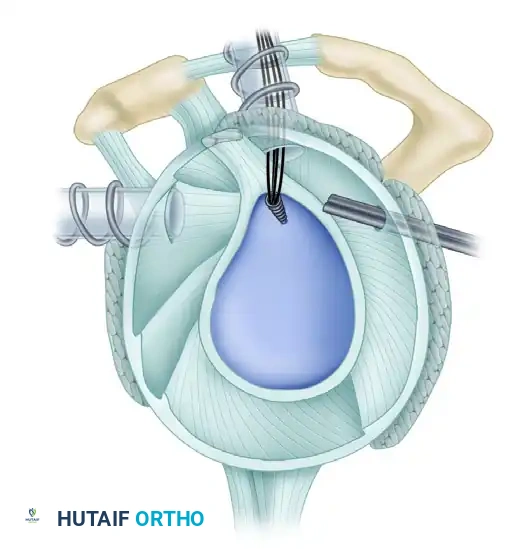
Figure 8: A double-loaded 3-mm anchor prepared for insertion.
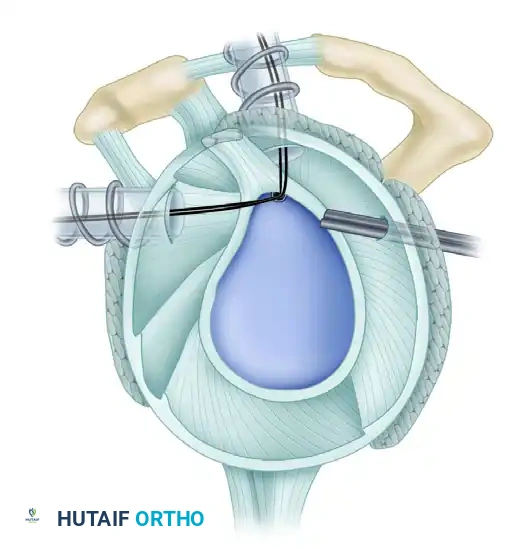
Figure 9: Precise anchor placement at the base of the biceps root.
3. Suture Passage and Management
Suture management is the most technically demanding aspect of the procedure and is critical to prevent postoperative knot impingement on the humeral head articular cartilage. A vertical suture passed through the labrum or a horizontal mattress suture passed behind the biceps is highly effective. Laboratory biomechanical studies confirm that the pull-out strength of these different suture configurations is comparable, provided the tissue bite is substantial.
Specialized penetrating instruments, such as Birdbeak suture passers (Arthrex, Naples, FL), are utilized to penetrate the labrum from superior to inferior.
* The 45-degree Birdbeak is ideal for passing sutures posterior to the biceps tendon through the anterosuperior cannula.
* The 22-degree Birdbeak is optimal for passing sutures anterior to the biceps through the anterior cannula.
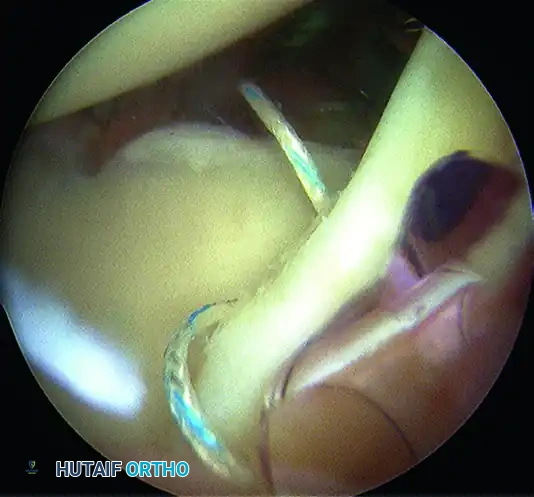
Figure 10: Anterior cannula positioning for optimal trajectory.
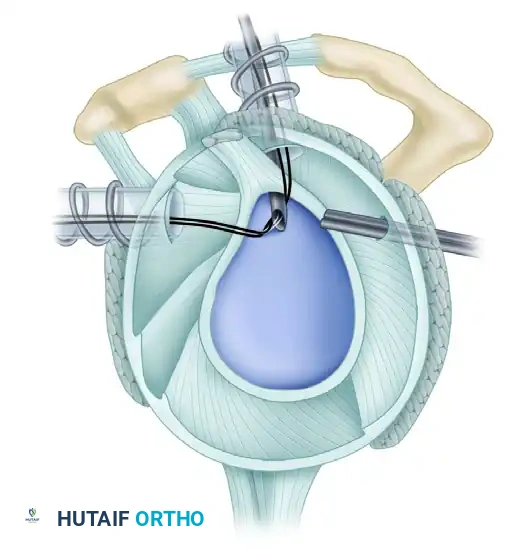
Figure 11: Sutures passed through the biceps anchor complex.
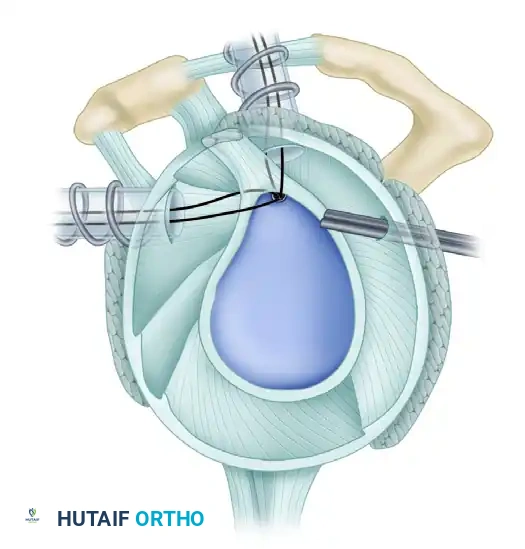
Figure 12: Suture retrieved posterior to the biceps tendon to neutralize peel-back.
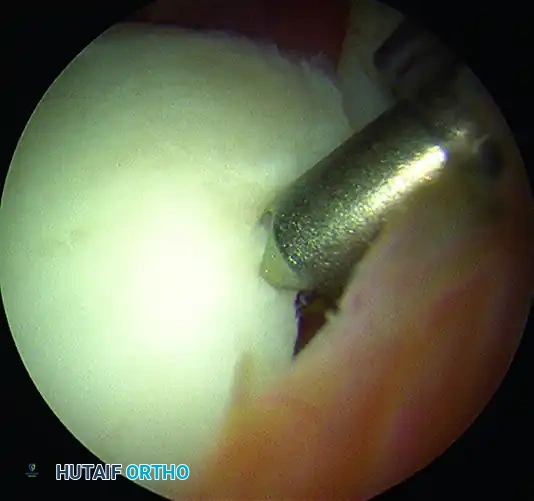
Figure 13: Suture retrieved anterior to the biceps tendon.
Alternatively, for complex tears or friable tissue, a suture shuttle device (e.g., a spectrum or lasso) allows for highly precise, atraumatic placement with minimal soft tissue disruption.
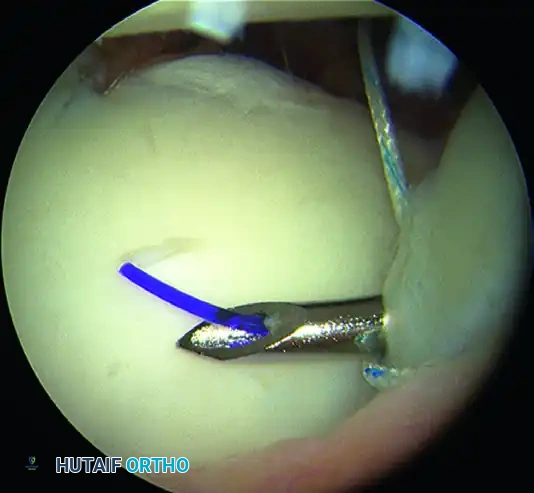
Figure 14: Passage of a suture shuttle at the base of the biceps.
If the SLAP lesion extends anteriorly beyond the 1-o’clock position (in a right shoulder), a separate suture anchor must be placed in the anterosuperior quadrant to secure the anterior extension of the labral tear and restore the tension of the middle glenohumeral ligament.
4. Knot Tying, Fixation, and Biomechanical Testing
Once all sutures are passed, meticulous knot tying is performed. The sutures must create simple loops around the labrum that are tensioned aggressively to pull the labrum down to the prepared bone bed and definitively neutralize peel-back forces. The surgeon should utilize stacked reversing half-hitches tied with a knot pusher, or complex sliding knots (e.g., the SMC or Weston knot) backed up with at least three reversing half-hitches on alternating posts for maximum knot security.
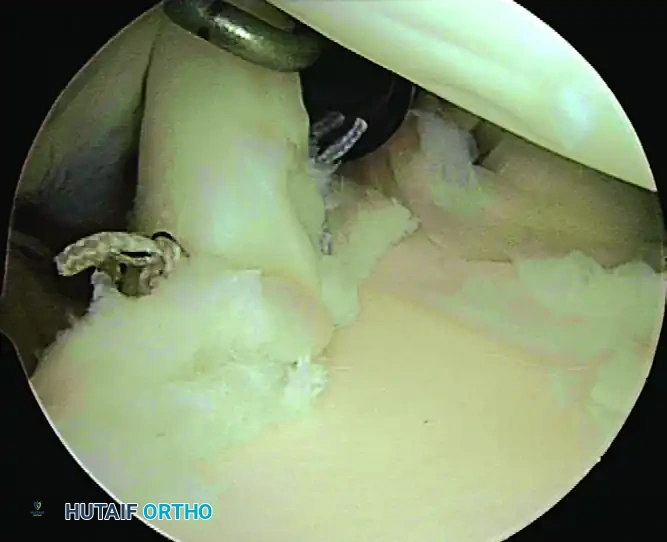
Figure 15: The completed SLAP repair, demonstrating a secure, anatomic restoration of the superior labrum.
After the repair is visually confirmed to be secure, the surgeon must unscrub the arm and perform the dynamic "peel-back" and "drive-through" tests again under direct arthroscopic visualization. A negative test indicates that the pathological biomechanics have been successfully corrected. If the drive-through sign remains positive despite a secure SLAP repair, this indicates persistent capsular laxity, and adjunctive measures for capsular tightening (e.g., inferior capsular plication or thermal shrinkage, though the latter is historically discouraged) must be strongly considered to prevent recurrent instability.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, the management of biceps tendon and SLAP lesions carries a distinct complication profile. The most frequent and debilitating complication following SLAP repair is postoperative stiffness, specifically profound deficits in external rotation. This iatrogenic adhesive capsulitis often results from over-tensioning the superior labrum, inadvertently capturing the superior glenohumeral ligament or the rotator interval during suture passage, or poor patient compliance with early rehabilitation protocols.
Hardware complications, though decreasing with the advent of biocomposite and all-suture anchors, remain a significant concern. Prominent anchors or bulky suture knots placed too close to the articular margin can cause catastrophic chondrolysis of the humeral head, leading to rapid-onset secondary osteoarthritis. Furthermore, failure of the repair, characterized by recurrent pain and a positive peel-back sign, can occur due to poor biological healing, premature return to throwing, or failure to address concomitant pathology such as GIRD or occult rotator cuff tearing.
| Complication | Estimated Incidence | Pathophysiology / Etiology | Prevention and Salvage Management |
|---|---|---|---|
| Postoperative Stiffness (Adhesive Capsulitis) | 10% - 15% | Over-tensioning of the repair; Inadvertent capture of SGHL/capsule; Inadequate early PROM. | Prevention: Precise suture placement; aggressive early Phase I rehab. Salvage: Aggressive physical therapy; Arthroscopic capsular release if refractory >6 months. |
| Persistent Pain / Failed Repair | 15% - 25% (Higher in older patients) | Failure of biological integration; Unrecognized biceps tendinosis; Missed concomitant cuff pathology. | Prevention: Strict adherence to indications (avoid SLAP repair in >40 yrs). Salvage: Conversion to subpectoral biceps tenodesis and labral debridement. |
| Hardware Prominence / Chondrolysis | < 2% | Anchor placed too proud; Articular cartilage penetration; Prominent knot stacks abrading the humeral head. | Prevention: Insert anchors at 45-degree angle; Use knotless technology; Recess anchors 1-2mm below bone surface. Salvage: Immediate hardware removal; Cartilage restoration procedures if severe. |
| Infection | < 1% | Contamination of portals; Hematogenous spread. | Prevention: Strict sterile technique; Preoperative prophylactic antibiotics. Salvage: Arthroscopic irrigation and debridement; Intravenous antibiotics; Hardware removal if biofilm present. |
When a SLAP repair fails, revision labral repair yields notoriously poor clinical outcomes. The definitive salvage procedure for a failed SLAP repair with persistent bicipital/labral pain is an open or arthroscopic subpectoral biceps tenodesis accompanied by meticulous debridement of the failed labral tissue and removal of any offending hardware. This effectively removes the pathological pain generator from the joint while preserving the functional length of the biceps muscle.
Phased Post-Operative Rehabilitation Protocols
Rehabilitation following surgical intervention for biceps and SLAP pathology is heavily dictated by the specific type of lesion and the mechanical integrity of the repair. Types I and III SLAP lesions are typically treated with simple arthroscopic debridement; because the structural integrity of the biceps anchor remains intact and stable, rehabilitation can progress rapidly as tolerated by the patient's pain levels. Conversely, Types II and IV lesions involve an unstable biceps anchor requiring formal mechanical repair. This necessitates strict, unwavering adherence to a phased, biology-driven protocol to protect the healing repair while simultaneously restoring complex glenohumeral kinematics.
Phase I: Immediate Postsurgical (Weeks 0–2)
During the initial biological healing phase, the operated arm is immobilized in a sling equipped with a small abduction pillow to relieve tension on the superior capsule.
* Goals: Protect the nascent repair, minimize inflammation, and initiate early protected motion to prevent adhesive capsulitis.
* Exercises:
* Passive and Active-Assisted Range of Motion (P/AAROM): Flexion strictly limited to < 120 degrees; External/Internal Rotation limited to < 30 degrees (performed with the arm resting at the side, absolutely not in abduction to avoid peel-back stress).
* Table slides in forward flexion, Codman's pendulums.
* Scapular mobility exercises (retraction, depression, and elevation) to prevent scapulothoracic dyskinesia.
* Passive elbow flexion; active elbow extension limited to 30 degrees short of full extension.
* Active hand/wrist ROM and gripping exercises to promote venous return.
* Submaximal, pain-free isometrics for the rotator cuff (IR/ER, ABD/ADD).
* Precautions: Strict sling compliance is mandatory. NO active biceps contraction is permitted under any circumstances. Full active elbow extension is strictly prohibited to avoid transmitting longitudinal tension directly to the newly repaired labral anchor.
* Capsular Stretching: Patients who required a concomitant posteroinferior capsulotomy for severe GIRD must begin modified "sleeper stretches" on postoperative day 1 to prevent recurrent contracture.
Phase II: Graded AROM & Strengthening (Weeks 3–11)
Weeks 3–6:
* Goals: Discontinue the sling (typically between weeks 3 and 4), restore normal scapulohumeral rhythm, and achieve full PROM.
* Exercises:
* Progress PROM to patient tolerance in all anatomical planes.
* Initiate sleeper stretches and cross-body adduction stretches in patients who did not have a capsulotomy to address insidious posterior capsular tightness.
* Glenohumeral joint mobilizations (Maitland Grades I and II) for pain control and early capsular mobility.
* Active elbow flexion with zero resistance.
* Theraband ER/IR isometrics with the arm in neutral adduction.
* Rhythmic stabilization and Proprioceptive Neuromuscular Facilitation (PNF) diagonals with light, controlled resistance.
* Precautions: No heavy lifting. No external rotation combined with abduction > 90 degrees (the peel-back position).
Weeks 7–9:
* Goals: Achieve AROM within normal functional limits; patient should be able to reach behind the back to the thoracolumbar junction.
* Exercises:
* Progress joint mobilizations to Grades III and IV if capsular restrictions persist.
* Initiate active elbow flexion with light weights (1-5 lbs).
* Progress isotonic strengthening of the rotator cuff and periscapular musculature using Therabands and light dumbbells.
* Closed-chain exercises (e.g., wall push-ups, weight shifts) to enhance joint proprioception.
* Precautions: No lifting objects > 5 lbs away from the body.
**Weeks 10–1
