Full Question & Answer Text (for Search Engines)
Question 1:
A 35-year-old carpenter sustains a deep laceration to his proximal volar forearm. After wound closure, he is unable to make an 'OK' sign, demonstrating an extended distal interphalangeal joint of the index finger and an extended interphalangeal joint of the thumb. Which of the following muscles is most likely spared in this specific isolated nerve injury?
Options:
- Flexor pollicis longus
- Flexor digitorum profundus to the index finger
- Flexor digitorum profundus to the middle finger
- Pronator quadratus
- Flexor carpi radialis
Correct Answer: Flexor carpi radialis
Explanation:
The patient has an Anterior Interosseous Nerve (AIN) palsy, characterized by the inability to form the 'OK' sign due to paralysis of the Flexor Pollicis Longus (FPL) and the Flexor Digitorum Profundus (FDP) to the index (and often middle) finger. The AIN also innervates the Pronator Quadratus. The Flexor Carpi Radialis (FCR) is innervated by the main branch of the median nerve before it gives off the AIN, and is therefore spared in an isolated AIN injury.
Question 2:
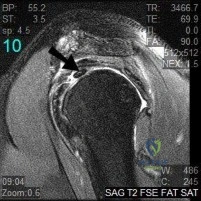
A 24-year-old athlete sustains a traction injury to the shoulder, presenting with weakness in forward elevation and isolated sensory loss over the lateral aspect of the proximal arm. An MRI reveals a compressive lesion within the quadrangular space. What anatomical structure forms the medial border of this space?
Options:
- Teres minor
- Teres major
- Surgical neck of the humerus
- Long head of the triceps
- Lateral head of the triceps
Correct Answer: Long head of the triceps
Explanation:
The quadrangular space transmits the axillary nerve and the posterior circumflex humeral artery. Its borders are: Superiorly - Teres minor; Inferiorly - Teres major; Medially - Long head of the triceps; Laterally - Surgical neck of the humerus. The patient's symptoms (deltoid weakness and lateral arm sensory loss) are classic for axillary nerve pathology.
Question 3:
When repairing a bucket-handle tear of the medial meniscus, a surgeon places sutures in the extreme peripheral 'red-red' zone. The primary arterial supply to this peripheral 10-30% of the meniscus is derived directly from which of the following?
Options:
- Middle genicular artery
- Medial inferior genicular artery
- Descending branch of the lateral circumflex femoral artery
- Popliteal artery
- Anterior tibial recurrent artery
Correct Answer: Medial inferior genicular artery
Explanation:
The vascular supply to the peripheral 10-30% of the medial meniscus is primarily provided by the medial inferior genicular artery and the medial superior genicular artery. The lateral meniscus is supplied by the lateral inferior genicular artery. The middle genicular artery pierces the posterior capsule to supply the cruciate ligaments.
Question 4:
A 22-year-old man sustains a proximal pole fracture of the scaphoid. The high risk of avascular necrosis in this region is due to the retrograde blood supply primarily derived from which of the following vessels?
Options:
- Palmar carpal branch of the radial artery
- Dorsal carpal branch of the radial artery
- Superficial palmar arch
- Deep palmar arch
- Anterior interosseous artery
Correct Answer: Dorsal carpal branch of the radial artery
Explanation:
The primary blood supply to the scaphoid (supplying 70-80% of the bone, including the entire proximal pole) is from the dorsal carpal branch of the radial artery. It enters the scaphoid at the dorsal ridge distally and flows in a retrograde fashion proximally, making proximal pole fractures highly susceptible to nonunion and avascular necrosis.
Question 5:
During a surgical approach for a highly comminuted talar body fracture, the surgeon notes damage to the artery of the tarsal canal. This artery is the predominant blood supply to the talar body. From which parent vessel does it originate?
Options:
- Anterior tibial artery
- Posterior tibial artery
- Peroneal artery
- Dorsalis pedis artery
- Lateral plantar artery
Correct Answer: Posterior tibial artery
Explanation:
The artery of the tarsal canal is a branch of the posterior tibial artery and supplies the majority of the talar body. It forms an anastomotic sling with the artery of the sinus tarsi (which arises from branches of the perforating peroneal and anterior lateral malleolar arteries).
Question 6:
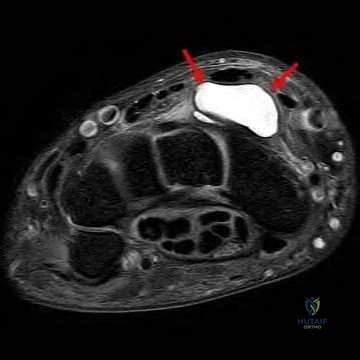
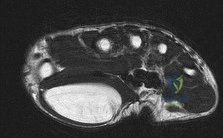
A patient sustains a distal radius fracture and undergoes volar locked plating. Three months postoperatively, she develops an inability to actively extend the interphalangeal joint of her thumb. During exploration, a ruptured tendon is found within the third dorsal extensor compartment. Which of the following bony landmarks does this tendon natively use as a fulcrum?
Options:
- Radial styloid
- Lister's tubercle
- Ulnar styloid
- Scaphoid tubercle
- Pisiform
Correct Answer: Lister's tubercle
Explanation:
The tendon of the Extensor Pollicis Longus (EPL) resides solely within the 3rd dorsal extensor compartment. It uses Lister's tubercle (the dorsal tubercle of the radius) as a fulcrum to angle towards the thumb. EPL rupture is a known complication following both conservative and surgical management of distal radius fractures.
Question 7:
A surgeon is performing an extensile lateral approach for a calcaneus fracture. The sural nerve is at risk of iatrogenic injury. At what approximate distance proximal to the insertion of the Achilles tendon does the sural nerve typically cross the lateral border of the Achilles tendon?
Options:
- 2 cm
- 5 cm
- 10 cm
- 15 cm
- 20 cm
Correct Answer: 10 cm
Explanation:
Anatomical studies show that the sural nerve crosses the lateral border of the Achilles tendon on average at 9.8 cm (approximately 10 cm) proximal to its calcaneal insertion. Knowledge of this landmark is critical during Achilles tendon repairs and lateral approaches to the hindfoot to avoid painful neuromas.
Question 8:
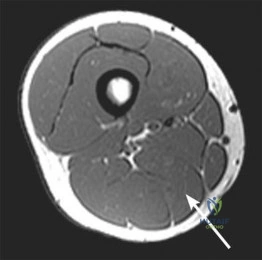
A 45-year-old male undergoes a biopsy for a soft tissue mass located in the femoral triangle. Which of the following accurately describes the medial border of the femoral triangle?
Options:
- Medial border of the sartorius
- Lateral border of the sartorius
- Medial border of the adductor longus
- Lateral border of the adductor longus
- Inguinal ligament
Correct Answer: Medial border of the adductor longus
Explanation:
The femoral triangle is bounded superiorly by the inguinal ligament, laterally by the medial border of the sartorius muscle, and medially by the medial border of the adductor longus muscle. The floor consists of the iliopsoas and pectineus. The contents (lateral to medial) are Nerve, Artery, Vein, Empty space, Lymphatics (NAVEL).
Question 9:
During a deltopectoral approach to the shoulder for a hemiarthroplasty, the internervous plane is developed. Which of the following statements regarding the handling of the cephalic vein during this approach is anatomically correct?
Options:
- It should be retracted medially to preserve venous drainage of the deltoid.
- It should be retracted laterally to preserve venous drainage of the deltoid.
- It is a direct tributary to the external jugular vein.
- It runs in the internervous plane between the axillary and median nerves.
- It must be ligated routinely to expose the subscapularis.
Correct Answer: It should be retracted laterally to preserve venous drainage of the deltoid.
Explanation:
The deltopectoral approach uses the internervous plane between the deltoid (axillary nerve) and pectoralis major (medial and lateral pectoral nerves). The cephalic vein lies in this interval. It is generally recommended to retract the cephalic vein laterally with the deltoid to preserve its primary venous tributaries, which originate from the deltoid muscle.
Question 10:
The volar approach to the radius (Henry approach) utilizes two different internervous planes depending on the region of the forearm. Proximally, the plane is between the brachioradialis and the pronator teres. Which nerves supply these two muscles, respectively?
Options:
- Radial and Ulnar
- Median and Radial
- Radial and Median
- Musculocutaneous and Median
- Radial and Anterior Interosseous
Correct Answer: Radial and Median
Explanation:
The proximal internervous plane of the volar Henry approach is between the Brachioradialis (innervated by the Radial nerve) and the Pronator Teres (innervated by the Median nerve). The distal internervous plane is between the Brachioradialis (Radial nerve) and the Flexor Carpi Radialis (Median nerve).
Question 11:
When performing an anterior approach to the hip (Smith-Petersen), the internervous plane is between the sartorius and the tensor fasciae latae superficially. Which of the following structures is at greatest risk of iatrogenic injury during the superficial dissection?
Options:
- Femoral nerve
- Lateral femoral cutaneous nerve
- Superior gluteal nerve
- Medial femoral circumflex artery
- Ascending branch of the lateral femoral circumflex artery
Correct Answer: Lateral femoral cutaneous nerve
Explanation:
During the anterior approach to the hip (Smith-Petersen), the superficial internervous plane is between the Sartorius (Femoral nerve) and the Tensor Fasciae Latae (Superior Gluteal nerve). The Lateral Femoral Cutaneous Nerve (LFCN) typically crosses over the sartorius 2-3 cm distal to the ASIS and is at high risk of injury during this superficial dissection.
Question 12:
A runner presents with chronic, recalcitrant heel pain. A nerve block of the first branch of the lateral plantar nerve (Baxter's nerve) completely resolves his pain temporarily. If left untreated and compression worsens, which of the following muscles would primarily demonstrate denervation changes on an MRI?
Options:
- Abductor hallucis
- Flexor digitorum brevis
- Quadratus plantae
- Abductor digiti minimi
- Adductor hallucis
Correct Answer: Abductor digiti minimi
Explanation:
Baxter's nerve is the first branch of the lateral plantar nerve. It courses between the deep fascia of the abductor hallucis and the medial aspect of the quadratus plantae, then beneath the calcaneus to supply the abductor digiti minimi muscle. Entrapment causes heel pain mimicking plantar fasciitis and can lead to atrophy of the abductor digiti minimi.
Question 13:
During an anatomic anterior cruciate ligament (ACL) reconstruction, the surgeon specifically addresses both the anteromedial (AM) and posterolateral (PL) bundles. Which of the following best describes the biomechanical role and tension pattern of the PL bundle?
Options:
- It is tight in flexion and primarily controls anteroposterior translation.
- It is tight in extension and primarily controls rotatory stability.
- It is tight in flexion and primarily controls rotatory stability.
- It is tight in extension and primarily controls anteroposterior translation.
- It remains isometric throughout the entire range of motion.
Correct Answer: It is tight in extension and primarily controls rotatory stability.
Explanation:
The ACL consists of the Anteromedial (AM) and Posterolateral (PL) bundles. The AM bundle tightens in flexion and is the primary restraint to anterior tibial translation. The PL bundle tightens in extension and is the primary restraint to rotatory loads (e.g., pivot shift). Thus, the PL bundle is most critical for rotatory stability near extension.
Question 14:
The posterior cruciate ligament (PCL) consists of two distinct bundles: the anterolateral (AL) and the posteromedial (PM). Which of the following statements accurately describes the tension pattern of these bundles?
Options:
- The AL bundle is tight in flexion, and the PM bundle is tight in extension.
- The AL bundle is tight in extension, and the PM bundle is tight in flexion.
- Both bundles are tightest in full extension.
- Both bundles are tightest in 90 degrees of flexion.
- The PM bundle is isometric, while the AL bundle tightens in extension.
Correct Answer: The AL bundle is tight in flexion, and the PM bundle is tight in extension.
Explanation:
The PCL has two main bundles. The Anterolateral (AL) bundle is larger and stronger; it is tight in flexion and lax in extension. The Posteromedial (PM) bundle is smaller; it is tight in extension and lax in flexion.
Question 15:
During a knee arthroscopy, a distinct ligamentous structure is identified passing directly anterior to the posterior cruciate ligament (PCL). It originates from the posterior horn of the lateral meniscus and inserts onto the lateral aspect of the medial femoral condyle. What is the proper anatomical name of this structure?
Options:
- Ligament of Wrisberg
- Ligament of Humphry
- Coronary ligament
- Transverse meniscal ligament
- Oblique popliteal ligament
Correct Answer: Ligament of Humphry
Explanation:
The meniscofemoral ligaments attach the posterior horn of the lateral meniscus to the medial femoral condyle. The Ligament of Humphry passes Anterior to the PCL, whereas the Ligament of Wrisberg passes Posterior to the PCL. (Mnemonic: 'H' comes before 'W' in the alphabet, just as Anterior comes before Posterior).
Question 16:
The cruciate anastomosis of the thigh is a vital collateral network that can provide distal limb perfusion in the setting of an acute occlusion of the superficial femoral artery. Which of the following vessels is NOT a component of this anatomotic ring?
Options:
- Inferior gluteal artery
- Medial femoral circumflex artery
- Lateral femoral circumflex artery
- First perforating artery of the profunda femoris
- Superior gluteal artery
Correct Answer: Superior gluteal artery
Explanation:
The cruciate anastomosis of the upper thigh is formed by the union of four arteries: the inferior gluteal artery (descending branch), the lateral femoral circumflex artery (transverse branch), the medial femoral circumflex artery (transverse branch), and the first perforating artery of the profunda femoris (ascending branch). The superior gluteal artery does not participate directly in the cruciate anastomosis.
Question 17:
A neonate presents with an adducted, internally rotated shoulder, extended elbow, and pronated forearm ('waiter's tip' posture) following shoulder dystocia during vaginal delivery. Injury to the upper trunk of the brachial plexus (C5-C6) is identified. Which of the following nerves originates directly from the upper trunk and would likely be affected in a pre-ganglionic injury at this level?
Options:
- Dorsal scapular nerve
- Long thoracic nerve
- Suprascapular nerve
- Medial pectoral nerve
- Thoracodorsal nerve
Correct Answer: Suprascapular nerve
Explanation:
The suprascapular nerve originates directly from the upper trunk (C5-C6) of the brachial plexus. The dorsal scapular and long thoracic nerves originate directly from the nerve roots (C5 and C5-C7, respectively). The medial pectoral and thoracodorsal nerves originate from the medial and posterior cords, respectively. Injury to the suprascapular nerve results in loss of external rotation and abduction initiation, contributing to the Erb's palsy posture.
Question 18:
A trauma surgeon is applying a lateral plate to the humerus for a highly displaced midshaft fracture. To safely expose the bone distally, the path of the radial nerve must be meticulously protected. At what approximate distance proximal to the lateral epicondyle does the radial nerve typically pierce the lateral intermuscular septum to enter the anterior compartment of the arm?
Options:
- 2-3 cm
- 5-6 cm
- 10-12 cm
- 15-16 cm
- 18-20 cm
Correct Answer: 10-12 cm
Explanation:
The radial nerve runs in the spiral groove of the posterior humerus and typically pierces the lateral intermuscular septum approximately 10 to 12 cm proximal to the lateral epicondyle to enter the anterior compartment of the arm. It then travels distally between the brachialis and brachioradialis muscles.
Question 19:
A 28-year-old rock climber presents with a painful 'bowstringing' deformity of his dominant long finger after hearing a loud 'pop' while dynamically loading a one-finger pocket hold. He likely ruptured the two most biomechanically critical annular pulleys. Which pulleys are these, and what are their anatomical origins?
Options:
- A1 and A3, originating primarily from the volar plates
- A2 and A4, originating primarily from the proximal and middle phalanges
- A1 and A5, originating primarily from the metacarpal and distal phalanx
- A2 and A4, originating primarily from the volar plates
- A1 and A3, originating primarily from the proximal and middle phalanges
Correct Answer: A2 and A4, originating primarily from the proximal and middle phalanges
Explanation:
The A2 and A4 pulleys are the most critical for preventing bowstringing of the flexor tendons. They have osseous origins: the A2 pulley arises from the periosteum of the proximal phalanx, and the A4 pulley arises from the periosteum of the middle phalanx. The A1, A3, and A5 pulleys originate primarily from the volar plates of the MP, PIP, and DIP joints, respectively.
Question 20:
A 40-year-old male is stabbed in the back, resulting in a spinal cord hemisection (Brown-Séquard syndrome) at the T8 level on the right side. Assuming a pure hemisection, which of the following physical examination findings will be distinctly present in the right lower extremity?
Options:
- Loss of pain and temperature sensation
- Loss of proprioception and vibration sensation
- Flaccid paralysis with absent reflexes
- Normal motor function with profound hyperalgesia
- Loss of all sensory modalities
Correct Answer: Loss of proprioception and vibration sensation
Explanation:
Brown-Séquard syndrome is characterized by a spinal cord hemisection. The dorsal columns (proprioception, vibration, light touch) cross in the medulla, so a lesion causes ipsilateral loss. The corticospinal tract (motor) crosses in the lower medulla, causing ipsilateral spastic paralysis below the lesion (not flaccid). The spinothalamic tract (pain, temperature) crosses in the spinal cord within 1-2 levels of entry, leading to contralateral loss of pain and temperature.