Comprehensive Introduction and Patho-Epidemiology
The management of deep, full-thickness articular cartilage defects in the young, active patient remains one of the most formidable challenges in orthopedic surgery. Unlike bone, articular cartilage possesses a notoriously poor intrinsic healing capacity due to its avascular, aneural, and alymphatic nature. When we encounter significant osteochondral defects—particularly those exceeding 2 to 3 square centimeters—traditional marrow stimulation techniques such as microfracture invariably fail over time. These techniques yield mechanically inferior fibrocartilage, predominantly composed of Type I collagen, which cannot withstand the complex shear and compressive forces of the human knee. In this context, Osteochondral Allograft (OCA) Transplantation emerges not merely as a salvage procedure, but as a primary, definitive reconstructive masterclass. It is the only technique capable of restoring mature, architecturally native hyaline cartilage and structurally sound subchondral bone in a single stage.
The patho-epidemiology of these lesions is diverse, often presenting a complex clinical puzzle. Patients typically fall into the young to middle-aged demographic (15 to 50 years old) and present with an insidious onset of mechanically mediated joint pain, recurrent effusions, and functional limitations. The etiology is broadly categorized into traumatic and atraumatic origins. Traumatic lesions frequently result from high-energy impaction or shearing forces. For instance, a classic pivot-shift mechanism during an anterior cruciate ligament (ACL) rupture often results in a profound compaction injury to the lateral femoral condyle. Similarly, transient lateral patellar dislocations frequently yield shearing osteochondral fractures of the medial patellar facet or the lateral trochlear ridge.
Conversely, atraumatic etiologies are heavily dominated by Osteochondritis Dissecans (OCD). While the precise pathogenesis of OCD remains a subject of academic debate—with theories ranging from repetitive microtrauma and localized ischemia to genetic predispositions—the end result is a focal area of subchondral bone necrosis leading to overlying cartilage delamination. These lesions classically manifest on the lateral aspect of the medial femoral condyle. Regardless of the etiology, by the time these patients reach the operating theater for an allograft, they have often endured a protracted clinical course. Many have a history of prior, failed cartilage restoration attempts, such as autologous chondrocyte implantation (ACI) or osteochondral autograft transfer (OATS). This history of prior surgical intervention signifies a hostile joint environment and dictates a meticulous, comprehensive approach to joint restoration.



Understanding the natural history of these defects is paramount. Small, asymptomatic lesions may be observed, but symptomatic, full-thickness defects (Outerbridge Grade IV or ICRS Grade 3/4) alter the complex tribology of the knee. The "pothole" effect increases rim stresses on the adjacent healthy cartilage, initiating a cascade of enzymatic degradation and mechanical wear that inevitably progresses to early-onset, unicompartmental osteoarthritis. Therefore, the biological imperative of osteochondral allograft transplantation is to halt this degenerative cascade by seamlessly integrating a viable, structurally identical composite tissue graft into the defect, thereby normalizing joint contact pressures and restoring pain-free kinematics.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of knee anatomy and biomechanics is the absolute foundation of successful osteochondral allograft transplantation. We must first consider the ultrastructure of the tissue we are replacing. Native articular cartilage is a highly specialized, viscoelastic tissue. Its extracellular matrix is heavily populated by a dense network of Type II collagen fibrils, which provide immense tensile strength, and aggrecan-rich proteoglycans, which draw in water to provide compressive resilience. The tissue is organized into distinct zones—superficial, transitional, deep, and calcified—each with specific chondrocyte orientations and mechanical properties. A fresh osteochondral allograft preserves this intricate architecture, delivering viable mature chondrocytes embedded within their native matrix, anchored securely to a subchondral bone base.
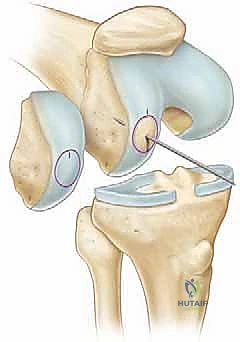
Topographically, the knee joint is an unforgiving environment. The distal femur is not a simple sphere; it features a complex, varying radius of curvature. The medial femoral condyle is generally larger, more curved, and extends further distally than the lateral condyle. The lateral condyle is broader in the anteroposterior dimension. The trochlear groove presents its own unique geometry, with a deeper central sulcus and a more prominent lateral facet to resist lateral patellar translation. When performing an allograft procedure, the surgeon must act as a precise biological carpenter. The donor graft must be harvested from the exact topographical match of the donor condyle to perfectly replicate the recipient's native articular contour. A mismatch of even 1 to 2 millimeters in articular step-off will lead to exponential increases in peak contact pressures, resulting in premature graft failure and reciprocal "kissing" lesions on the opposing articular surface.
From a surgical approach perspective, navigating the neurovascular and muscular anatomy requires extreme vigilance. While the standard parapatellar arthrotomies (medial or lateral) are generally safe, deep dissection and instrumentation demand respect for the posterior structures. The popliteal artery and vein, along with the tibial nerve, lie in close proximity to the posterior capsule. When addressing far posterior condylar lesions, particularly during the guide pin placement and subsequent reaming of the recipient socket, the trajectory must be perfectly controlled. Plunging past the posterior cortex with a reamer is a catastrophic complication. Furthermore, the muscular intervals utilized—such as the subvastus or midvastus approaches—should be carefully managed to preserve the dynamic stabilizers of the patella, minimizing postoperative extensor mechanism dysfunction.
Biomechanically, the success of the graft is inextricably linked to the overall mechanical alignment of the lower extremity and the integrity of the menisci. The meniscus is a critical secondary stabilizer and load-sharer, transmitting up to 50% of the compressive load in extension and 85% in 90 degrees of flexion. An osteochondral allograft placed in a meniscus-deficient compartment is doomed to fail due to point-loading. Similarly, the mechanical axis of the limb dictates load distribution. A patient with a medial femoral condyle defect and concurrent varus malalignment will subject the medial compartment to massive, unphysiologic stress. It is an absolute biomechanical law in cartilage restoration that any significant malalignment (typically >2-3 degrees from neutral) must be corrected with a concurrent or staged realignment osteotomy (e.g., High Tibial Osteotomy or Distal Femoral Osteotomy). Failure to respect these biomechanical principles renders the allograft procedure futile.
Exhaustive Indications and Contraindications
Patient selection is arguably the most critical determinant of success in osteochondral allograft transplantation. The ideal candidate is a highly motivated, young to middle-aged adult (typically between 15 and 50 years of age) with high physical demands who presents with a symptomatic, focal, full-thickness (ICRS Grade III or IV) unipolar articular cartilage defect. The size of the lesion is a primary indication; while smaller lesions (<2 cm²) might be amenable to OATS or microfracture, defects larger than 2 cm², and particularly those exceeding 3 cm², are the classic domain of fresh osteochondral allografts. Furthermore, the depth of the lesion is a crucial factor. Pathologies that involve significant subchondral bone loss, such as deep OCD lesions, avascular necrosis (AVN), or cystic changes following failed microfracture, necessitate the bone-replacing capacity of an osteochondral allograft.
Conversely, the contraindications must be strictly observed to prevent predictable failures. Diffuse, multicompartmental osteoarthritis is an absolute contraindication; placing a focal graft into a globally degenerated joint is akin to patching a sinking ship. Inflammatory arthropathies (e.g., Rheumatoid Arthritis) represent a hostile, cytokine-rich environment that will rapidly degrade the graft. "Kissing lesions"—where both the femoral condyle and the corresponding tibial plateau have full-thickness defects—are generally considered a strong relative, if not absolute, contraindication, as the altered tribology of the opposing surface will shear the new graft.
Furthermore, uncorrected mechanical abnormalities are absolute contraindications until addressed. As previously discussed, malalignment must be corrected via osteotomy. Ligamentous instability (e.g., ACL deficiency) must be stabilized, either prior to or concurrently with the allograft procedure. Morbid obesity (BMI > 35) places exponential stress on the joint and significantly increases the risk of graft subsidence and failure. Finally, patients who are unwilling or unable to comply with the rigorous, prolonged postoperative rehabilitation protocol should not be offered this procedure.
| Category | Specific Criteria / Conditions | Clinical Rationale |
|---|---|---|
| Primary Indications | Symptomatic focal full-thickness defects (ICRS Grade III/IV) | Restores native hyaline architecture. |
| Lesion size > 2.0 cm² | Exceeds the biological capacity of autograft/microfracture. | |
| Deep osteochondral lesions (OCD, AVN, subchondral cysts) | Requires structural subchondral bone restoration. | |
| Revision of failed prior cartilage procedures (ACI, OATS) | Rescues hostile biological environments. | |
| Relative Contraindications | Age > 50 years | Decreased biological healing capacity; arthroplasty may be superior. |
| BMI > 35 kg/m² | Excessive mechanical load increases risk of graft subsidence. | |
| "Kissing lesions" (Bipolar disease) | Altered opposing surface tribology accelerates graft wear. | |
| Tobacco use | Impairs microvascular integration of the osseous portion. | |
| Absolute Contraindications | Diffuse Osteoarthritis (Kellgren-Lawrence Grade III/IV) | Global joint failure cannot be treated with focal resurfacing. |
| Inflammatory Arthropathy (e.g., Rheumatoid Arthritis) | Systemic inflammatory cytokines will destroy the allograft. | |
| Active joint infection or history of recent septic arthritis | High risk of catastrophic graft infection and failure. | |
| Uncorrected malalignment or ligamentous instability | Abnormal biomechanical forces guarantee mechanical failure. |
Pre-Operative Planning, Templating, and Patient Positioning
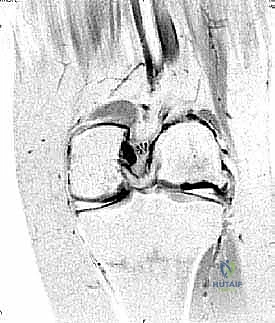
Meticulous preoperative planning is the hallmark of the master surgeon. The process begins with comprehensive imaging. Standard weight-bearing radiographs, including a 45-degree flexion posteroanterior (Rosenberg) view, lateral, and Merchant views, are mandatory to assess joint space narrowing and patellofemoral tracking. A full-length, standing hip-to-ankle radiograph is absolutely critical to calculate the mechanical axis and plan any necessary concomitant osteotomies. However, the gold standard for defining the osteochondral lesion is high-resolution Magnetic Resonance Imaging (MRI). We rely on fluid-sensitive sequences (T2-weighted or proton density with fat suppression) to precisely map the surface area, depth, and exact topographic location of the defect. Advanced MRI techniques, such as T2 mapping or dGEMRIC, can also be utilized to assess the biochemical health of the surrounding "normal-appearing" cartilage.
Once the lesion is quantified, the complex logistics of allograft procurement begin. We utilize fresh osteochondral allografts, as freezing destroys chondrocyte viability. Grafts are harvested from donors under strict American Association of Tissue Banks (AATB) guidelines, undergoing rigorous serological and microbiological testing to minimize disease transmission (e.g., HIV, Hepatitis B/C, Syphilis). Because cartilage is largely immunoprivileged—lacking blood vessels and possessing a dense matrix that hides chondrocyte antigens—ABO blood typing and HLA matching are not required, nor is systemic immunosuppression. The critical factor is time. Chondrocyte viability peaks at the time of harvest and slowly declines. Current protocols allow for storage at 4°C in specialized nutrient media for up to 28 days, though most surgeons prefer implantation between days 14 and 21, balancing the time required for infectious disease clearance with optimal cellular viability.
Templating involves matching the donor to the recipient. The tissue bank utilizes the recipient's MRI or CT data to match the donor's distal femur based on size (anteroposterior and mediolateral dimensions) and radius of curvature. A mismatch here complicates the surgery immensely. The surgeon must review these matching metrics prior to accepting the graft. Once the graft arrives and is cleared for surgery, the patient is brought to the operating room.
Patient positioning must facilitate both precise intra-articular access and dynamic assessment of joint kinematics. The patient is positioned supine on the operating table. We utilize a lateral thigh post placed proximal to the tourniquet and a foot positioner (or a commercially available leg holder) that allows the knee to be manipulated freely from full extension to at least 120 degrees of flexion. This hyperflexion is often required to access far posterior condylar lesions. A sterile tourniquet is applied high on the thigh; however, we routinely attempt to perform the procedure without inflating it. Operating without a tourniquet reduces ischemic time to the limb, minimizes postoperative quadriceps inhibition, and allows the surgeon to accurately assess the bleeding bone bed of the recipient socket, which is crucial for optimal osseous integration of the graft.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of an osteochondral allograft transplantation is an exercise in extreme precision, utilizing specialized instrumentation to create a perfect press-fit biological cylinder.
Diagnostic Arthroscopy and Lesion Preparation
We begin with a thorough diagnostic arthroscopy through standard anterolateral and anteromedial portals. This step confirms the preoperative MRI findings, assesses the integrity of the menisci and cruciate ligaments, and evaluates the global health of the articular cartilage. Once the focal defect is identified, an arthroscopic probe is used to palpate the margins. All delaminated, fibrillated, or undermined cartilage must be meticulously debrided back to a healthy, vertical, stable rim using an arthroscopic shaver and curettes. Establishing this stable perimeter is critical, as it defines the exact diameter of the required graft and prevents postoperative edge loading and fluid extravasation beneath the graft.

Arthrotomy and Recipient Socket Creation
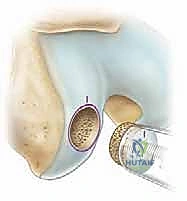
Following arthroscopic preparation, a longitudinal parapatellar arthrotomy is performed. For a medial femoral condyle defect, a medial parapatellar or subvastus approach is utilized; for a lateral defect, a lateral arthrotomy is preferred. The incision must be large enough to allow perpendicular access to the lesion. Once exposed, a specialized sizing cylinder from the allograft instrument set is placed over the defect. The goal is to encompass the entire lesion within the smallest possible circular footprint, typically ranging from 15mm to 30mm in diameter.


A guide pin is then driven through the center of the sizing cylinder, absolutely perpendicular to the surrounding healthy articular surface. This trajectory is the most critical step of the procedure; a malaligned pin will result in a proud or sunken graft edge. A cannulated counterbore reamer is passed over the pin to score the cartilage and ream the subchondral bone to a precise depth, usually between 6 to 8 millimeters. The goal is to ream just deep enough to reach healthy, bleeding cancellous bone, avoiding excessive depth that could compromise the structural integrity of the condyle. The recipient socket is then thoroughly irrigated and dilated to ensure a smooth, uniform cylinder.



Donor Graft Harvesting
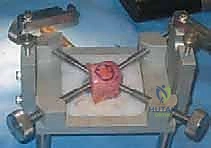
Attention is then turned to the back table, where the fresh allograft hemicondyle is secured in a specialized workstation. The surgeon identifies the exact topographic match on the donor condyle that corresponds to the recipient's defect location. Using a donor coring reamer that matches the diameter of the recipient socket, a cylindrical osseocartilaginous plug is harvested.



The depth of the recipient socket is measured at four quadrants (12, 3, 6, and 9 o'clock) to account for the contour of the condyle. These exact measurements are transferred to the donor plug, and the excess bone is carefully amputated using an oscillating saw. Crucially, the osseous portion of the donor graft is then subjected to rigorous pulsatile lavage. This step washes out the donor marrow elements—specifically the immunogenic glycoproteins and lipids—leaving behind a clean trabecular scaffold, which significantly reduces the risk of an untoward immune response and enhances creeping substitution.





Implantation and Fixation
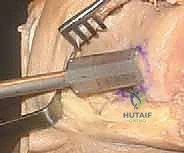
The final step is the implantation of the graft. The graft is gently aligned with the recipient socket, ensuring the topographic orientation matches perfectly. It is then inserted using a gentle press-fit technique, often requiring light tapping with an oversized tamp. The graft must "bottom out" on the host bone while simultaneously achieving a perfectly flush articular surface. A graft that is proud by even 1mm will bear excessive load and fail; a sunken graft will lead to rim overload of the native cartilage.



If the press-fit is perfectly secure, no supplemental fixation is required. However, if the graft is large, involves the unconstrained posterior condyle, or lacks rotational stability, supplemental fixation is mandatory. This is typically achieved using bioabsorbable chondral darts or headless titanium compression screws placed outside the weight-bearing zone. The joint is then taken through a full range of motion to confirm stability and tracking before standard layered closure.
Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, osteochondral allograft transplantation is a complex biological procedure with inherent risks. The most significant complication is graft failure, which can manifest as osseous non-union, subchondral collapse, or chondral delamination. Graft failure rates hover around 15-20% at the 10-year mark, heavily influenced by patient age, lesion size, and adherence to postoperative protocols. Non-union of the osseous portion is often due to inadequate recipient bed preparation, thermal necrosis during reaming, or failure to adequately lavage the donor bone marrow. When subchondral collapse occurs, it is usually a mechanical failure due to unrecognized malalignment or premature weight-bearing.
Infection and disease transmission remain paramount concerns, though incredibly rare due to modern screening. The risk of viral transmission (HIV, HCV) is estimated to be less than 1 in 1.6 million. Bacterial infection of the graft is slightly more common but still rare (<1%), usually presenting as an acute postoperative septic joint. This requires immediate arthroscopic irrigation, debridement, and tailored intravenous antibiotics; unfortunately, severe infections often necessitate graft explantation.
Arthrofibrosis is a common postoperative hurdle, particularly given the large arthrotomy and the required period of protected weight-bearing. Incidence rates range from 5% to 10%. Patients who fail to achieve 90 degrees of flexion by 6 weeks postoperatively require aggressive intervention. Management begins with intensified physical therapy, but refractory cases may require manipulation under anesthesia (MUA) or arthroscopic lysis of adhesions to restore functional kinematics.
When an osteochondral allograft ultimately fails, the salvage options depend heavily on the patient's age and the degree of joint deterioration. In young patients with isolated graft failure, a revision allograft is technically feasible, though outcomes are generally inferior to primary procedures. For older patients, or those who have developed progressive unicompartmental or multicompartmental osteoarthritis, conversion to a Unicompartmental Knee Arthroplasty (UKA) or Total Knee Arthroplasty (TKA) becomes the definitive salvage pathway.
| Complication | Estimated Incidence | Etiology / Risk Factors | Management / Salvage Strategy |
|---|---|---|---|
| Graft Failure / Collapse | 15 - 20% (at 10 years) | Malalignment, premature weight-bearing, immune reaction, poor bone integration. | Revision OCA, Unicompartmental Arthroplasty (UKA), or Total Knee Arthroplasty (TKA). |
| Arthrofibrosis | 5 - 10% | Prolonged immobilization, excessive surgical trauma, poor pain control. | Aggressive PT, Manipulation Under Anesthesia (MUA), Arthroscopic lysis of adhesions. |
| Osseous Non-union | 2 - 5% | Thermal necrosis during reaming, inadequate marrow lavage, smoking. | Prolonged protected weight-bearing, bone stimulators, revision grafting. |
| Deep Joint Infection | < 1% | Contaminated graft, standard surgical site infection risks. | Emergent I&D, IV antibiotics, potential graft explantation if uncontrolled. |
| Disease Transmission | < 0.0001% | Viral window periods during donor screening (extremely rare). | Infectious disease consultation, systemic antiviral/antibacterial therapy. |
Phased Post-Operative Rehabilitation Protocols
The surgical procedure is only half the battle; the postoperative rehabilitation protocol is equally critical to the survival and integration of the allograft. The protocol must delicately balance the mechanical protection required for osseous integration with the early motion necessary for chondrocyte nutrition and the prevention of arthrofibrosis. Rehabilitation is strictly phased and heavily dependent on the size and location of the graft.
Phase 1: Protection and Biological Healing (Weeks 0-6)
For femoral condyle lesions, the primary goal in this phase is the protection of the
