Total Wrist Arthrodesis & Scaphoid Subluxation Guide
Key Takeaway
Total wrist arthrodesis is a highly reliable salvage procedure for end-stage radiocarpal and midcarpal arthritis. Utilizing the Weiss and Hastings technique with a contoured dynamic compression plate ensures rigid fixation and optimal positioning. Concurrently, recognizing rotary subluxation of the scaphoid—often presenting with a positive Watson shift test and dorsal intercalated segment instability (DISI)—is critical to preventing progressive carpal collapse and advanced arthritic degeneration.
TOTAL ARTHRODESIS OF THE WRIST
Total wrist arthrodesis remains the gold-standard salvage procedure for patients suffering from end-stage pancarpal arthritis, severe carpal instability, paralytic deformities, or post-traumatic conditions such as advanced Scapholunate Advanced Collapse (SLAC) or Scaphoid Nonunion Advanced Collapse (SNAC). The primary goal of the procedure is to provide a stable, painless wrist while maximizing the functional capacity of the hand and digits.
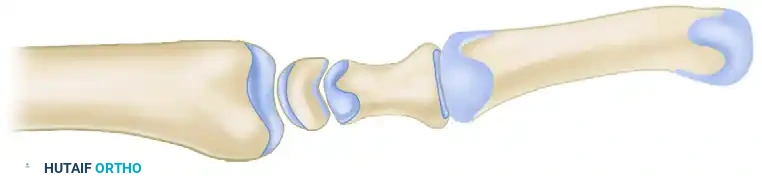
The technique popularized by Weiss and Hastings utilizes a rigid dorsal plate spanning the radius, carpus, and third metacarpal. This method provides superior biomechanical stability, high fusion rates, and eliminates the need for prolonged postoperative cast immobilization.
Preoperative Planning and Biomechanics
Successful wrist arthrodesis requires meticulous preoperative planning. The functional position of the wrist is generally accepted to be 10 to 15 degrees of extension with slight ulnar deviation. This position maximizes the mechanical advantage of the extrinsic finger flexors, optimizing grip strength.
Clinical Pearl: Excessive wrist extension (greater than 20 degrees) should be avoided, as it can lead to extensor tendon irritation, fatigue of the intrinsic hand musculature, and difficulty with perineal care and other activities of daily living.
Surgical Technique: The Weiss and Hastings Approach
The following step-by-step technique details the application of a contoured dynamic compression plate augmented with local bone graft.
1. Incision and Exposure
- Incision: Make a 10- to 15-cm dorsal longitudinal incision centered precisely over the radiocarpal joint, extending from the distal radius to the mid-shaft of the long finger (third) metacarpal.
- Superficial Dissection: Incise the subcutaneous tissues sharply. It is imperative to identify and protect the dorsal sensory branches of the radial nerve radially and the dorsal branch of the ulnar nerve ulnarly.
- Retinacular Release: Incise the extensor retinaculum longitudinally between the third and fourth extensor compartments. Transpose the extensor pollicis longus (EPL) tendon radially to protect it during the procedure.
- Deep Exposure: Elevate the second and fourth extensor compartments subperiosteally. Expose the dorsal aspect of the distal radius, the carpus, and the long finger metacarpal.
2. Joint Preparation and Decortication
- Tubercle Excision: Use a sharp osteotome to excise Lister's tubercle from the distal radius. This provides a flat surface for plate application and yields valuable local autograft.
- Decortication: Meticulously decorticate the dorsal one-fourth of the scaphoid, lunate, capitate, and the third carpometacarpal (CMC) joint.
Surgical Warning: Do not include the ulnar midcarpal joints (triquetrohamate) or the second (index) carpometacarpal joint in the fusion mass unless they exhibit frank arthritic changes. Preserving micro-motion at the index CMC joint significantly improves postoperative hand function and grip accommodation.

3. Bone Graft Harvesting
- Utilize a large (6-mm cup) curet to harvest cancellous bone graft from the distal radius. The optimal harvest site is located slightly to the lateral (radial) side of the excised Lister's tubercle. This local graft is highly osteogenic and avoids the morbidity associated with iliac crest bone graft harvesting.
4. Plate Selection and Application
- Implant Selection: Select a pre-contoured 3.5-mm dynamic compression plate (DCP) designed specifically for wrist arthrodesis. The plate must be of sufficient length to ensure that at least six bone cortices (three screws) are engaged in the distal metacarpal, and six bone cortices are engaged in the distal radius.

- Fixation Sequence: The order of screw placement is critical for achieving compression and maintaining alignment.
- Distal Fixation: After positioning the plate, secure the distal screws to the third metacarpal first. This establishes the distal anchor.
- Graft Placement: Before securing the proximal screws, pack the harvested cancellous bone graft from the distal radius tightly into the denuded radiocarpal and midcarpal joint spaces.
- Proximal Fixation: Fix the plate to the distal radius. Utilizing the dynamic compression holes will help compress the carpus against the radius.
- Carpal Fixation: Place one or two cancellous lag screws through the midportion of the plate directly into selected carpal bones, most critically the capitate. This neutralizes the fusion mass and prevents intercalated segment toggle.
Surgical Pitfall: Unless the distal radioulnar joint (DRUJ) is overtly symptomatic and arthritic, do not include it in the fusion or impinge upon it with the plate. Preserving forearm pronosupination is vital for patient outcomes.
5. Radiographic Confirmation and Closure
- Obtain intraoperative fluoroscopy (AP and Lateral views) to confirm hardware placement, screw length, and joint compression. Ensure the plate holds the wrist in the optimal 10 to 15 degrees of extension.


- Deflate the tourniquet, achieve meticulous hemostasis, and place a closed suction drain if necessary.
- Capsular Closure: Close the dorsal capsule over the plate using interrupted sutures to provide a soft-tissue interposition layer.
- Retinacular Closure: Repair the extensor retinaculum, leaving the EPL transposed subcutaneously to prevent attrition rupture against the hardware.
- Close the skin and apply a bulky compressive dressing supported by a volar short-arm splint.
Postoperative Protocol
Patients are typically immobilized in a short-arm splint for 10 to 14 days to allow for soft tissue healing. Following suture removal, a removable thermoplastic splint is fabricated. Active and passive digital range of motion exercises are initiated immediately to prevent tendon adhesions. The splint is worn between exercises and at night for approximately 6 to 8 weeks, or until radiographic evidence of trabecular bridging across the fusion sites is observed.
ROTARY SUBLUXATION OF THE SCAPHOID (SCAPHOLUNATE DISSOCIATION)
While total wrist arthrodesis is the definitive treatment for end-stage carpal collapse, recognizing and treating the precursor injuries is paramount. The most common and clinically significant form of carpal instability is rotary subluxation of the scaphoid, driven by scapholunate dissociation.
Pathoanatomy and Kinematics
The scaphoid serves as the critical mechanical link between the proximal and distal carpal rows. Its stability relies on a complex network of intrinsic and extrinsic ligaments. The primary stabilizer of the scapholunate articulation is the scapholunate interosseous ligament (SLIL), particularly its thick, robust dorsal subregion. Secondary stabilizers include the long radiolunate ligament and the radioscaphocapitate (RSC) ligament.
When these ligaments are disrupted, the synchronous motion of the proximal carpal row is lost. Biomechanically, the scaphoid has an inherent tendency to flex volarly, while the triquetrum has a tendency to extend dorsally. The lunate, caught in the middle, is normally balanced by these opposing forces.
Upon complete rupture of the SLIL and secondary stabilizers, the scaphoid rotates dorsally at its proximal pole and assumes a vertical, flexed orientation. Uncoupled from the scaphoid, the lunate follows the mechanical pull of the intact lunotriquetral ligament and extends dorsally. This divergent collapse pattern is clinically recognized as Dorsal Intercalated Segment Instability (DISI).
Classification
Watson and Black categorized rotary subluxation of the scaphoid into four distinct clinical stages, which dictate the treatment algorithm:
1. Dynamic: Instability is only apparent under mechanical load or stress maneuvers. Standard static radiographs appear normal.
2. Static: Permanent, fixed deformity visible on standard resting radiographs.
3. With Degenerative Arthritis: Progressive articular wear leading to Scapholunate Advanced Collapse (SLAC).
4. Secondary: Subluxation occurring secondary to other carpal pathologies, such as Kienböck's disease (avascular necrosis of the lunate).
Clinical Evaluation
The classic mechanism of injury is a high-energy fall on an extended, ulnarly deviated wrist. Unfortunately, the severity of the initial trauma is frequently underestimated, leading to a misdiagnosis of an "uncomplicated wrist sprain."
Patients typically present with chronic, activity-related dorsal radial wrist pain, localized swelling, and a subjective sense of weakness or "giving way" during grip activities. On physical examination, point tenderness is elicited directly over the dorsal scapholunate interval (just distal to Lister's tubercle). Range of motion, particularly wrist flexion, is often limited.
Provocative Maneuvers
Two highly specific physical examination maneuvers are essential for diagnosing scaphoid instability:
1. The Watson Scaphoid Shift Test:
* Technique: The examiner faces the patient. To examine the right wrist, the examiner uses their right hand (and vice versa). The examiner places four fingers on the dorsum of the distal radius and places their thumb firmly on the volar scaphoid tuberosity.
* The patient's wrist is initially placed in ulnar deviation, which aligns the scaphoid longitudinally with the axis of the forearm.
* While maintaining firm dorsal-directed pressure on the scaphoid tuberosity, the examiner passively moves the wrist into radial deviation.
* Positive Finding: In a normal wrist, the scaphoid flexes smoothly, pushing the examiner's thumb volarly. In an unstable wrist, the thumb pressure prevents normal scaphoid flexion. Instead, the proximal pole of the scaphoid is driven dorsally out of the elliptical radial fossa, subluxating over the dorsal rim of the radius. This elicits a painful "clunk" and reproduces the patient's symptoms.
2. The "Catch-Up Clunk" Test:
* As the wrist is moved under load from radial deviation to ulnar deviation, the scaphoid normally extends smoothly.
* In the presence of rotary subluxation, the uncoupled lunate remains in a volar-flexed position until sufficient capsular tension is generated. It then suddenly snaps or "catches up" into alignment with the scaphoid, producing a palpable and audible clunk.
Radiographic Evaluation
Accurate radiographic interpretation is critical for diagnosing static instability and planning surgical intervention.
Anteroposterior (AP) View
- Scapholunate Gap (Terry Thomas Sign): A widening of the scapholunate interval greater than 2 mm is highly suspicious for dissociation. A gap greater than 3 mm is considered pathognomonic.
- Clenched Fist View: If dynamic instability is suspected, an AP view taken with the patient actively clenching their fist will drive the capitate proximally into the scapholunate interval, exacerbating the gap and unmasking the instability.
- Cortical Ring Sign: As the scaphoid flexes volarly, it is viewed end-on (axial projection) on the AP radiograph. The distal pole appears as a dense, foreshortened cortical ring.
Lateral View
The lateral radiograph is the definitive study for diagnosing DISI deformity and quantifying the degree of carpal collapse.
* Scaphoid Orientation: The scaphoid appears vertically oriented rather than lying at its normal oblique angle.
* Scapholunate Angle: The normal angle between the longitudinal axis of the scaphoid and the longitudinal axis of the lunate ranges from 30 to 80 degrees (mean 47 degrees). In a DISI deformity, the scaphoid flexes and the lunate extends, resulting in a scapholunate angle greater than 60 degrees.
* Capitolunate Angle: The normal angle between the capitate and the lunate is nearly collinear (less than 20 degrees). In DISI, the lunate extension creates a capitolunate angle greater than 20 degrees.
Clinical Pearl: A scapholunate gap of 2 mm is not universally symptomatic and may represent a normal variant in some patients. Always obtain bilateral comparative radiographs to assess the patient's baseline ligamentous laxity before recommending surgical intervention.
Early recognition of rotary subluxation of the scaphoid allows for soft-tissue reconstruction or limited intercarpal fusions. Failure to diagnose this condition inevitably leads to altered carpal kinematics, progressive articular shear forces, and the eventual need for salvage procedures such as the total wrist arthrodesis detailed above.
You Might Also Like