Operative Management of Camptodactyly: The Smith Tendon Release Technique
Key Takeaway
The Smith tendon release is a comprehensive surgical intervention for severe or progressive camptodactyly. This technique systematically addresses the anatomical structures contributing to proximal interphalangeal joint flexion contractures. Key steps include volar skin Z-plasties, release of abnormal fascial bands, mobilization of the intrinsic apparatus, and management of flexor digitorum superficialis anomalies. Proper execution and strict adherence to postoperative extension splinting protocols are critical for correcting central slip attenuation and achieving optimal functional outcomes.
Introduction to the Smith Tendon Release
Camptodactyly is a complex, non-traumatic flexion deformity of the proximal interphalangeal (PIP) joint, most commonly affecting the small finger. While mild, non-progressive cases are often managed conservatively with static or dynamic splinting, severe or rapidly progressive deformities require surgical intervention. The Smith Tendon Release is a highly systematic, step-wise surgical approach designed to address the multifactorial pathoanatomy of camptodactyly.
The deformity is rarely isolated to a single anatomical structure. Instead, it involves a cascade of contractures affecting the volar skin, digital fascia, intrinsic musculature, flexor digitorum superficialis (FDS), and the volar plate. Furthermore, chronic flexion leads to secondary attenuation of the extensor mechanism's central slip. The Smith technique provides a comprehensive algorithm to sequentially release or lengthen these tethering structures while preserving the delicate biomechanical balance of the digit.
This guide provides an exhaustive, textbook-level analysis of the Smith Tendon Release, detailing the surgical anatomy, step-by-step operative technique, and rigorous postoperative rehabilitation protocols required for optimal outcomes.
Surgical Anatomy and Pathomechanics
To successfully execute the Smith release, the surgeon must possess a profound understanding of the digital pathoanatomy associated with PIP joint flexion contractures.
The Digital Fascia and Skin
In chronic camptodactyly, the volar skin becomes deficient, acting as a primary tether. Beneath the skin, the digital fascia hypertrophies. Specifically, Grayson’s ligaments—which normally originate from the volar aspect of the flexor tendon sheath and insert into the volar skin—become contracted, forming tough, linear fibrous bands that restrict PIP extension.
The Intrinsic Apparatus and Lumbricals
The intrinsic muscles, particularly the lumbricals and interossei, often exhibit anomalous anatomy in camptodactyly.
* Anomalous Lumbrical Insertion: The lumbrical may insert abnormally into the proximal phalanx, the volar plate, or even the FDS tendon proximal to the A1 pulley, rather than its normal insertion into the radial lateral band.
* Lateral Band Subluxation: Chronic PIP flexion causes the lateral bands of the extensor mechanism to subluxate volarly, shifting their axis of pull volar to the PIP joint's center of rotation. This converts them from extensors to secondary flexors of the PIP joint.
The Flexor Digitorum Superficialis (FDS)
The FDS is frequently the primary deforming force in camptodactyly. Abnormalities generally fall into two categories:
1. Shortened FDS: The muscle-tendon unit is intact but structurally short, creating a dynamic tether.
2. Proximal Aplasia: The proximal muscle belly is absent, and only a fibrotic distal tendon remnant is present, acting as an unyielding static tether.
The Central Slip
Chronic flexion posture places continuous tension on the central slip of the extensor digitorum communis (EDC) at its insertion on the middle phalanx base. Over time, this structure attenuates (stretches), resulting in an extensor lag even after the volar tethering structures are released.
💡 Clinical Pearl: Central Slip Management
A fundamental tenet of the Smith technique is that attenuation of the central slip should never be treated with surgical plication or exploration. Surgical intervention on the central slip in this setting frequently leads to severe scarring and loss of flexion. Instead, central slip attenuation is managed exclusively through strict postoperative extension splinting, which allows the tendon to shorten and remodel dynamically.
Preoperative Evaluation and Indications
Indications for Surgery
- Progressive PIP joint flexion contracture exceeding 40 to 50 degrees.
- Failure of a rigorous, 6-month trial of conservative management (dynamic/static splinting and stretching).
- Functional impairment in activities of daily living.
- Deformity interfering with the development of normal hand function in pediatric patients.
Clinical Assessment: The Tenodesis Test
The preoperative physical examination must include a dynamic assessment of the FDS and the intrinsic muscles.
* FDS Assessment: Passively extend the wrist and metacarpophalangeal (MCP) joints. If the PIP joint contracture worsens or cannot be passively extended, the FDS is structurally short.
* Intrinsic Tightness (Bunnell Test): Assess PIP joint flexion with the MCP joint held in extension versus flexion to evaluate intrinsic versus extrinsic tightness.
Radiographic Evaluation
Standard posteroanterior, lateral, and oblique radiographs of the affected digit are mandatory. In long-standing cases, adaptive bony changes may be present, such as flattening of the condyles of the proximal phalanx or narrowing of the PIP joint space.
⚠️ Surgical Warning: Bony Abnormalities
Do not attempt to surgically correct or explore preoperatively detected bony abnormalities at the neck of the proximal phalanx or the articular surfaces of the PIP joint. Intra-articular osteotomies or recontouring in the setting of camptodactyly yield no functional benefit and significantly increase the risk of intractable postoperative stiffness.
Step-by-Step Surgical Technique
The Smith Tendon Release is performed under regional or general anesthesia with a well-padded proximal tourniquet to ensure a bloodless surgical field. Loupe magnification is highly recommended.
1. Incision and Skin Management
The surgical approach must address the absolute shortage of volar skin.
* Make a standard volar linear incision along the affected digit.
* Immediately convert this linear incision into multiple Z-plasties.
* Crucial Geometry: Ensure that the central limbs of the Z-plasties are placed transversely directly over the flexion creases of the PIP and distal interphalangeal (DIP) joints. This prevents the formation of longitudinal scar contractures that could recreate the deformity.
* Carefully elevate the full-thickness skin flaps, preserving the subdermal vascular plexus to prevent flap necrosis.
2. Fascial Release and Neurovascular Protection
- Identify the neurovascular bundles early and protect them throughout the procedure. In severe contractures, the bundles may be displaced centrally or encased in fibrotic tissue.
- Identify and resect the tough, linear fibrous bands of the digital fascia.
- Specifically target and release the bony attachments of Grayson’s ligaments. Cleland’s ligaments (which lie dorsal to the neurovascular bundle) are typically spared unless they are clearly contributing to the contracture.
3. Mobilization of the Intrinsic Apparatus
- Examine the lateral bands of the intrinsic apparatus and the interosseous muscles.
- Free the lateral bands from any abnormal, widespread attachments to the lateral sides of the proximal phalanx. These abnormal tethers prevent the lateral bands from gliding dorsally during PIP extension.
- Verification: Apply proximal traction to the lateral bands. This maneuver should confirm that PIP joint extension is now mechanically possible. If the joint remains locked, further volar release is required.
4. Assessment of the Central Slip
Once the volar fascial and intrinsic tethers are released, evaluate the integrity of the central slip.
* Flex the patient's wrist and MCP joints to relax the extrinsic extensors.
* Observe the PIP joint. If an extensor lag is present at the PIP joint under these conditions, it confirms attenuation of the central slip.
* Action: Do nothing surgically. Note the attenuation for the postoperative splinting protocol. Do not expose or plicate the central slip.
5. Lumbrical Muscle Exploration
- Trace the lumbrical muscle from its origin in the palm to its insertion.
- Identify any abnormal insertions (e.g., adherent to the proximal phalanx capsule, inserting into the volar plate, or inserting into the FDS tendon proximal to the A1 pulley).
- Release any anomalous lumbrical insertions that contribute to the flexion tether.
6. FDS Evaluation and Management
The management of the FDS is the most critical and technically demanding portion of the Smith release. Perform an intraoperative tenodesis test: extend the wrist and observe PIP extension. If the PIP cannot be fully extended, the FDS is short and must be addressed.
Scenario A: Proximal Aplasia (Type 2 Abnormality)
* If exploration reveals that the proximal muscle belly of the FDS is absent and only a fibrotic distal tendon remnant exists, this structure serves no functional purpose and acts solely as a tether.
* Action: Perform a complete division (tenotomy) of the abnormal FDS remnant.
Scenario B: Shortened but Intact FDS (Type 1 Abnormality)
* If the FDS tendon is anatomically normal proximally but structurally short, it must be lengthened.
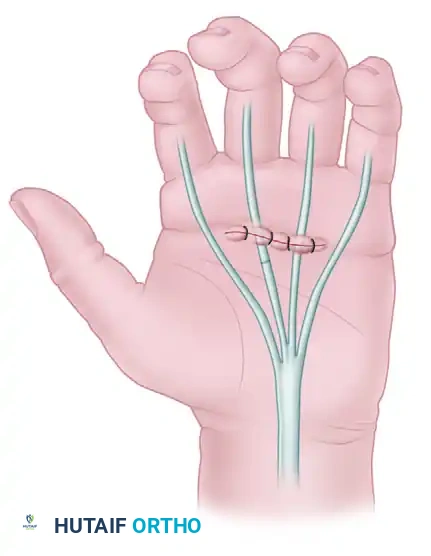
* Action: Perform a lengthening and transposition of the FDS insertions at the level of Camper's chiasma.
* Technique: Divide the two slips of the FDS insertion eccentrically. Cut the radial slip proximally and the ulnar slip distally. Suture the long proximal radial slip to the distal ulnar insertion. This fractional lengthening technique preserves the FDS's independent flexion capability while eliminating the flexion contracture.
7. Deep Capsular Releases (If Necessary)
If the PIP joint still cannot achieve full passive extension after the skin, fascia, intrinsics, and FDS have been addressed, the contracture has likely involved the joint capsule.
* Perform a sequential release of the flexor tendon sheath (A3 pulley region).
* Release the accessory collateral ligaments.
* Perform a volar plate arthrolysis by releasing the proximal check-rein ligaments of the volar plate.
* Caution: Avoid excessive release of the proper collateral ligaments to prevent iatrogenic joint instability.
8. Closure
- Deflate the tourniquet and achieve meticulous hemostasis. Hematoma formation is a primary cause of postoperative scarring and stiffness.
- Transpose the Z-plasty flaps. If there is still a critical skin shortage preventing tension-free closure with the finger in extension, a full-thickness skin graft (harvested from the hypothenar eminence or groin) may be required, though the multiple Z-plasty technique usually circumvents this need.
- Suture the skin with non-absorbable monofilament sutures.
Postoperative Care and Rehabilitation
The surgical release is only the first half of the treatment. The postoperative rehabilitation protocol is rigorous, prolonged, and absolutely critical to the success of the Smith Tendon Release. The primary goal of the postoperative phase is to maintain the surgical extension while allowing the attenuated central slip to remodel and shorten.
Phase 1: Immobilization (Weeks 0 to 4)
- Immediately postoperatively, the hand and affected digit are placed in a well-padded, rigid volar cast or thermoplastic splint.
- The wrist is positioned in neutral, the MCP joints in 45–70 degrees of flexion, and the PIP joint is maintained in absolute, full extension.
- This static extension is maintained uninterrupted for exactly 4 weeks. This period is non-negotiable, as it allows the volar skin flaps to heal and provides the biological environment necessary for the attenuated central slip to contract and restore the extensor mechanism's mechanical advantage.
Phase 2: Controlled Mobilization (Weeks 4 to 6)
At the 4-week mark, the cast is removed, and the patient is transitioned to a custom thermoplastic splint. The protocol diverges based on whether the FDS was lengthened.
-
Standard Protocol (FDS divided or not addressed):
- A splint is applied that allows for active-resisted flexion of the PIP joint.
- The patient performs active flexion exercises against the resistance of dynamic splinting components (e.g., rubber bands), which helps glide the flexor tendons and prevent adhesions.
- Passive flexion is strictly avoided to prevent stretching the newly remodeled central slip.
- Between exercise sessions, the finger is splinted in full extension.
-
Modified Protocol (FDS Lengthened at the Chiasma):
- If the FDS was fractionally lengthened and repaired, the tendon repair site is highly vulnerable to rupture.
- Active-resisted flexion must be delayed for an additional 8 weeks (until 12 weeks postoperatively).
- During this time, the patient is permitted gentle, active, non-resisted motion within a protected arc, but heavy resistance is contraindicated.
Phase 3: Maturation and Weaning (Week 6 and Beyond)
- At 6 weeks postoperatively, daytime splinting is discontinued, and the patient is encouraged to use the hand for light activities of daily living.
- Night Splinting: A static PIP extension splint must be worn every night. Because scar tissue continues to contract for up to 6 to 12 months postoperatively, night splinting is typically maintained for a minimum of 6 months to prevent recurrence of the flexion contracture.
Complications and Pitfalls
- Recurrence of Deformity: The most common complication, almost exclusively due to patient non-compliance with the prolonged postoperative night splinting regimen.
- Persistent Extensor Lag: Occurs if the PIP joint is not held in strict extension for the first 4 weeks, preventing the central slip from remodeling.
- FDS Rupture: Can occur if active-resisted flexion is initiated too early in patients who underwent FDS lengthening.
- Neurovascular Injury: The digital nerves are highly susceptible to injury during the release of Grayson's ligaments and anomalous lumbrical insertions. Meticulous dissection is mandatory.
- Joint Stiffness: Over-aggressive capsular release or failure to achieve hemostasis can lead to severe arthrofibrosis. The surgeon must balance the need for complete release with the preservation of gliding tissues.
Conclusion
The Smith Tendon Release remains a cornerstone in the operative management of severe camptodactyly. By systematically addressing the skin, digital fascia, intrinsic apparatus, and flexor tendons, the surgeon can effectively dismantle the multifactorial tethers causing the PIP flexion contracture. Success relies heavily on the surgeon's restraint in avoiding central slip exploration and bony recontouring, coupled with an uncompromising adherence to a prolonged, extension-biased postoperative rehabilitation protocol.
You Might Also Like