INTRODUCTION TO SUBFASCIAL SPACE INFECTIONS
The potential spaces in the subfascial and deeper layers of the hand are infrequently infected in the modern antibiotic era; however, when they do occur, they represent true orthopedic emergencies. Because the hand is a complex, tightly compartmentalized structure, a high level of clinical suspicion must be maintained to ensure early detection and aggressive surgical treatment. Delay in diagnosis can lead to catastrophic consequences, including ischemic necrosis of intrinsic musculature, irreversible stiffness, tendon rupture, and systemic sepsis.
These deep spaces are not true anatomical voids but rather potential spaces filled with loose areolar tissue, bounded by unyielding fascial septa. When inoculated with bacteria—often via penetrating trauma, neglected calluses, or hematogenous spread—these spaces rapidly fill with purulence. The resulting increased compartmental pressure compromises local microcirculation and facilitates the proximal spread of infection along paths of least resistance, such as the lumbrical canals.
SURGICAL ANATOMY OF THE DEEP SPACES OF THE HAND
A profound understanding of the cross-sectional anatomy of the hand is the cornerstone of effective surgical management. The recognized deep spaces of the hand include the interdigital web spaces, the midpalmar space, the thenar space, a less well-defined hypothenar space, the space of Parona (in the distal forearm), and the dorsal subaponeurotic space.
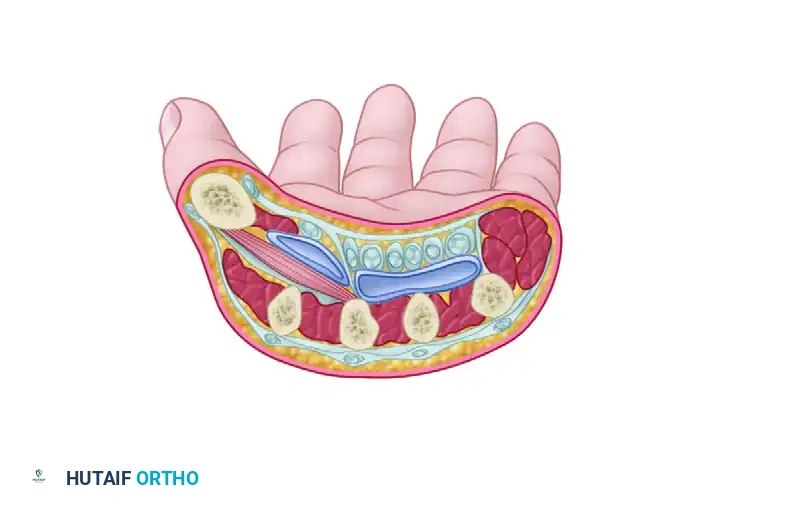
The Midpalmar Space
The midpalmar space lies deep to the flexor tendons of the middle, ring, and small fingers.
* Anterior Boundary: The flexor tendons of the ulnar three digits and the deep palmar arch.
* Posterior Boundary: The fascia covering the volar interosseous muscles and the third, fourth, and fifth metacarpals.
* Radial Boundary: The midpalmar (oblique) septum, which attaches to the third metacarpal and separates this space from the thenar space.
* Ulnar Boundary: The hypothenar septum.
The Thenar Space
The thenar space is located radial to the midpalmar septum. It is crucial to note that this space is not within the thenar muscle mass itself, but rather deep to the flexor tendons of the index finger and superficial to the adductor pollicis muscle.
* Anterior Boundary: The flexor tendons of the index finger and the first lumbrical.
* Posterior Boundary: The adductor pollicis muscle.
* Ulnar Boundary: The midpalmar (oblique) septum.
The Interdigital (Web) Spaces
There are three fat-filled interdigital web spaces located just proximal to the superficial transverse metacarpal ligament at the level of the metacarpophalangeal (MCP) joints. These spaces contain the digital neurovascular bundles and the lumbrical muscles. They serve as a critical conduit between the palmar and dorsal aspects of the hand, as well as a pathway to the deep midpalmar space via the lumbrical canals.
The Dorsal Subaponeurotic Space
This space lies on the dorsum of the hand, deep to the extensor tendons and their interconnecting aponeurosis (connexus intertendineus), and superficial to the dorsal interosseous fascia and metacarpal bones. Infections here are rare but can cause profound dorsal swelling and extensor tendon dysfunction.
Clinical Pearl: The midpalmar (oblique) septum is a robust fascial layer that effectively prevents the direct lateral spread of infection between the thenar and midpalmar spaces. However, concomitant infections of both spaces can occur if the infection tracks proximally into the space of Parona, which communicates with both.
WEB SPACE INFECTION (COLLAR BUTTON ABSCESS)
Pathogenesis and Biomechanics
A web space infection, classically referred to as a "collar button abscess" or "hourglass abscess," usually localizes in one of the three fat-filled interdigital spaces. Typically, the infection begins beneath palmar calluses in manual laborers. A micro-fissure in the hypertrophied stratum corneum allows bacterial ingress (most commonly Staphylococcus aureus or Streptococcus pyogenes) into the palmar subcutaneous space.
Because the palmar skin and the underlying palmar aponeurosis are thick, unyielding, and firmly tethered by vertical fascial fibers (Cleland's and Grayson's ligaments), the accumulating purulence cannot easily decompress volarly. Instead, it follows the path of least resistance. It tracks dorsally through the fibers of the superficial transverse metacarpal ligament or along the lumbrical canal, localizing to drain on the dorsum of the hand.
This creates a characteristic "hourglass" or "collar button" configuration: a small palmar abscess connected via a narrow fascial tract to a larger dorsal abscess.
Surgical Warning: The dorsal tissue becomes obviously swollen, erythematous, and fluctuant, drawing the clinician's attention. However, the significant and more dangerous amount of the abscess remains hidden nearer the palm. Unless the palmar component is adequately drained, the infection may spread proximally through the lumbrical canal directly into the middle palmar space.
Clinical Presentation and Diagnosis
Patients typically present with severe, throbbing pain in the affected web space. Clinical signs include:
* The "V" Sign: The adjacent digits are held in an abducted position due to the mass effect of the abscess in the web space.
* Dorsal Edema: Massive swelling on the dorsum of the hand, which can mimic a primary dorsal subcutaneous abscess.
* Palmar Tenderness: Exquisite point tenderness over the volar aspect of the web space, often localized beneath a thickened callus.
* Erythema and Warmth: Extending proximally along the dorsum or volar palm.
Laboratory investigations should include a complete blood count (CBC), erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP). Plain radiographs are mandatory to rule out underlying osteomyelitis, septic arthritis of the MCP joint, or the presence of a radiopaque foreign body.
SURGICAL MANAGEMENT: OPERATIVE TECHNIQUE
Surgical incision and drainage is the definitive treatment for a collar button abscess. Antibiotic therapy alone is insufficient once a purulent collection has formed.
Preoperative Preparation
- Anesthesia: General anesthesia or a regional brachial plexus block is preferred. Local infiltration is contraindicated due to the risk of spreading the infection and the acidic environment rendering local anesthetics ineffective.
- Positioning: Supine with the arm extended on a radiolucent hand table.
- Tourniquet: A well-padded pneumatic arm tourniquet is essential for a bloodless field, allowing precise identification of neurovascular structures. Exsanguination should be performed by arm elevation rather than an Esmarch bandage to prevent proximal milking of purulence.
Step-by-Step Surgical Approach
To adequately decompress a collar button abscess, two longitudinal incisions are usually necessary: one on the dorsal surface and one on the palmar surface.
1. The Palmar Incision
- Begin the incision distal to the distal palmar crease, curving it proximally over the affected web space.
- Crucial Technique: The incision must be curvilinear or zigzag (e.g., a Bruner-type incision). Crossing the palmar creases at right angles must be strictly avoided to prevent the development of postoperative flexion contractures.
- Carefully dissect through the subcutaneous tissue. If a callus is present, the necrotic center may be excised, but preserve as much viable palmar skin as possible.
- Identify and protect the digital neurovascular bundles, which lie in close proximity to the lumbrical muscles.
2. The Dorsal Incision
- Make a longitudinal incision on the dorsal surface of the web space, centered between the metacarpal heads.
- Dissect bluntly through the dorsal subcutaneous tissue to enter the dorsal component of the abscess cavity.
- Protect the dorsal sensory branches of the radial or ulnar nerves and the extensor hood apparatus.
3. Connecting the Spaces and Debridement
- Using a blunt hemostat, gently probe from the dorsal incision toward the palmar incision to identify the communicating tract (the "neck" of the collar button).
- Strict Prohibition: The web itself (the free edge of the interdigital skin) should not be incised. Incising the web margin invariably leads to a severe, functionally limiting adduction contracture of the digits.
- Once the tract is identified, gently dilate it to ensure free communication between the dorsal and palmar compartments.
- Obtain deep tissue cultures (aerobic, anaerobic, and fungal) before initiating irrigation.
- Perform a meticulous debridement of all necrotic fat, fascia, and devitalized tissue.
- Copiously irrigate the connected spaces with several liters of sterile normal saline.
4. Drainage and Closure
- The wounds are generally left open to heal by secondary intention or delayed primary closure.
- A small corrugated drain, Penrose drain, or a loose wick of iodoform gauze may be passed through the tract from dorsal to palmar to maintain patency and prevent premature skin closure.
- Apply a bulky, non-adherent, absorbent dressing.
POSTOPERATIVE PROTOCOL AND REHABILITATION
Immediate Postoperative Care
- Immobilization: The hand should be immobilized in a volar resting splint in the "safe position" (intrinsic-plus position): wrist extended 20-30 degrees, MCP joints flexed 70-90 degrees, and interphalangeal (IP) joints fully extended. This prevents collateral ligament contracture.
- Elevation: Strict elevation of the hand above the level of the heart is critical to reduce edema, which is a primary driver of postoperative stiffness.
- Antibiotics: Intravenous antibiotics should be initiated empirically (covering MRSA and Streptococcus, e.g., Vancomycin and Ceftriaxone) and subsequently tailored based on intraoperative culture and sensitivity results.
Wound Management and Therapy
- The dressing and drains are typically removed or advanced at 48 to 72 hours postoperatively.
- If the infection is severe or necrotic tissue remains, a planned second-look debridement in the operating room may be necessary.
- Once the acute signs of infection (erythema, severe pain, purulent drainage) have subsided, aggressive hand therapy must commence.
- Rehabilitation: Active and active-assisted range of motion (ROM) exercises for the digits, wrist, and forearm are instituted to prevent tendon adhesions and joint stiffness. Edema control techniques (e.g., Coban wrapping, retrograde massage) are utilized as the wound heals.
COMPLICATIONS AND PITFALLS
Failure to recognize the dual-compartment nature of a collar button abscess or inadequate surgical execution can lead to severe complications:
- Proximal Propagation: Inadequate palmar drainage forces the infection proximally through the lumbrical canal into the midpalmar space, transforming a localized web space infection into a deep, limb-threatening space infection.
- Web Space Contracture: Incising the free edge of the web space skin will result in a hypertrophic scar and a syndactyly-like contracture, severely limiting finger abduction.
- Neurovascular Injury: Blind or aggressive sharp dissection in the web space can easily transect the common digital artery or proper digital nerves.
- Stiffness: Prolonged immobilization or failure to control postoperative edema will result in profound stiffness of the MCP and IP joints, often requiring subsequent tenolysis or capsulotomy.
By maintaining a high index of suspicion, understanding the complex fascial anatomy, and executing a precise, dual-incision surgical approach, the orthopedic surgeon can effectively eradicate subfascial space infections and restore full function to the hand.
📚 Medical References
- subfascial space infections, Hand Clin 14:557, 1998.
- Jebson PJ: Infections of the fi ngertip: paronychias and felons, Hand Clin 14:547, 1998.
- Jebson PJ, Louis DS: Hand infections, Hand Clin 14:511, 1998.
- Jeong GK, Lester B: Mycobacterium tuberculosis infection of the wrist, Am J Orthop 30:411, 2001.
- Jones MW, Wahid IA, Matthews JP: Septic arthritis of the hand due to Mycobacterium marinum, J Hand Surg 13B:333, 1988.
- Kakinoki R, Ikeguchi R, Nakamura T: Second dorsal metacarpal artery muscle fl ap: an adjunct in the treatment of chronic phalangeal osteomyelitis, J Hand Surg 29A:49, 2004.
- Kanavel AB: Infections of the hand: a guide to the surgical treatment of acute and chronic suppurative processes in the fi ngers, hand, and forearm, 6th ed, Philadelphia, 1933, Lea & Febiger. Kann SE, Jacquemin J, Stern PJ: Simulators of hand infections, Instr Course Lect 46:69, 1997.
- Kaplan JE, Zoschke D, Kisch AL: Withdrawal of immunosuppressive agents in the treatment of disseminated coccidioidomycosis, Am J Med 68:624, 1980.
- Karanas YL, Bogdan MA, Chang J: Community acquired methicillin-resistant Staphylococcus aureus hand infections: case reports and clinical implications, J Hand Surg 25A:760, 2000.
- Kargi E, Akduman D, Gungor E, et al: Primary extremity actinomycosis causing osteomyelitis of the hand, Plast Reconstr Surg 112:1495, 2003.
- Katzman BM, Bozentka DJ: Salmonella osteomyelitis of the hand in an infant with sickle cell disease, Orthopedics 23:727, 2000.
- Keyser JJ, Eaton RG: Surgical cure of chronic paronychia by eponychial marsupialization, Plast Reconstr Surg 58:66, 1976.
- Kilgore ES: Hand infections: II, J Hand Surg 5A:723, 1983.
- Klein MB, Chang J: Management of hand and upper-extremity infections in heart transplant recipients, Plast Reconstr Surg 106:598, 2000.
- Kono M, Stern PJ: The history of hand infections, Hand Clin 14:511, 1998.
- Kour AK, Looi KP, Phone MH, et al: Hand infections in patients with diabetes, Clin Orthop Relat Res 331:238, 1996.
- Kriegs-Au G, Ganger R, Petje G: The sequelae of late diagnosis in tuberculous fl exor tenosynovitis of the hand—a report of 2 cases, Acta Orthop Scand 74:221, 2003.
- Kroesen S, Widmer AF, Tyndall A, et al: Serious bacterial infections in patients with rheumatoid arthritis under anti-TNFα therapy, Rheumatology 42:617, 2003.
- Lee EY, Rubin DA, Brown DM: Recurrent Mycobacterium marinum tenosynovitis of the wrist mimicking extraarticular synovial chondromatosis on MR images, Skeletal Radiol 33:405, 2004.
- Lille S, Hayakawa T, Neumeister NW, et al: Continuous postoperative catheter irrigation is not necessary for the treatment of suppurative fl exor tenosynovitis, J Hand Surg 25B:304, 2000.
- Linscheid RL, Dobyns JH: Common and uncommon infections of the hand, Orthop Clin North Am 6:1063, 1975.
- Liseki EJ, Curl WW, Markey KL: Hand and forearm infections caused by Aeromonas hydrophila, J Hand Surg 5A:605, 1980.
- Loncarich D, Shin A: Suppurative
