Operative Management of Sternoclavicular Joint Dislocations: A Comprehensive Guide
Key Takeaway
Anterior sternoclavicular joint dislocations rarely require surgery, with "skillful neglect" being the preferred treatment. Conversely, posterior dislocations are potentially life-threatening orthopedic emergencies requiring prompt reduction due to the proximity of mediastinal structures. When surgery is indicated for chronic instability or irreducible dislocations, resection of the medial clavicle combined with robust stabilization to the first rib using fascial grafts or synthetic tape is the gold standard.
INTRODUCTION TO STERNOCLAVICULAR JOINT PATHOLOGY
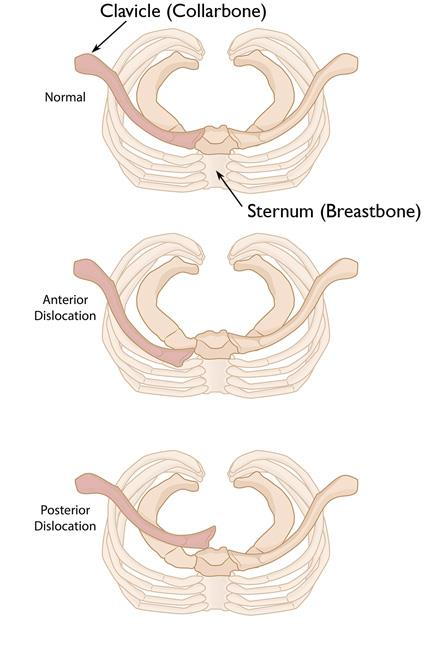
The sternoclavicular joint (SCJ) represents the sole true diarthrodial articulation between the axial skeleton and the upper extremity. Despite its critical biomechanical role in shoulder girdle kinematics, injuries to the SCJ are relatively uncommon, accounting for less than 3% of all shoulder girdle traumas. The joint is inherently unstable due to the incongruence of the articular surfaces; less than half of the medial clavicle articulates with the shallow sternal notch. Consequently, stability is almost entirely dependent on the robust surrounding ligamentous complex, primarily the posterior capsule, the intra-articular disc ligament, and the extra-articular costoclavicular (rhomboid) ligaments.
Understanding the dichotomy between anterior and posterior SCJ dislocations is paramount for the practicing orthopedic surgeon. While anterior dislocations are visually prominent and common, they are generally benign. In stark contrast, posterior dislocations are rare but represent true orthopedic emergencies due to the immediate proximity of critical mediastinal structures, including the trachea, esophagus, great vessels, and brachial plexus.
ANTERIOR STERNOCLAVICULAR DISLOCATIONS
Pathoanatomy and Clinical Presentation
Anterior dislocations typically result from an indirect force applied to the anterolateral aspect of the shoulder, driving the shoulder backward and levering the medial clavicle anteriorly out of the sternal notch. Patients present with a visible and palpable prominence over the medial chest wall.
Most authors and experienced shoulder surgeons agree that old, unreduced anterior dislocations of the SCJ usually cause minimal, if any, functional disability. Reports of surgical intervention for this condition have indicated that patients primarily complain of mild weakness, cosmetic deformity, and fatigue of the arm during heavy manual labor or overhead athletic endeavors.
The Principle of "Skillful Neglect"
Lunseth et al., who extensively reported on the surgical treatment of this condition, concluded that many patients with chronic anterior dislocations experience no significant disability. Consequently, they strongly recommended nonoperative treatment. Rarely, if ever, is surgical intervention strictly required for an isolated, uncomplicated anterior dislocation.
Rockwood famously championed the nonoperative approach of "skillful neglect." He noted that before any attempts were made to surgically stabilize the joint, patients typically had minimal discomfort, complaining only of the bony prominence and a sensation of subluxation with certain motions. Conversely, after failed surgical interventions, patients often continued to have symptoms, exacerbated by surgical scarring and iatrogenic complications.
Chronic Spontaneous Dislocation
Booth and Roper described a distinct subset of patients presenting with chronic or recurring spontaneous dislocations of the SCJ occurring without any specific history of trauma. They postulated that these patients likely possess underlying generalized "joint laxity" or collagen disorders (e.g., Ehlers-Danlos or Marfan syndrome). Surgical intervention in this specific demographic is notoriously prone to failure and should be avoided whenever possible.
Historical Surgical Procedures and Contraindications
For the rare individual who absolutely requires surgery (e.g., intractable pain, severe occupational impairment), several basic surgical procedures have been historically described:
* Fascia Lata Reconstruction: The use of fascia lata woven around the clavicle and first rib was described by Speed, as well as by Key and Conwell. Bankart and Milch utilized fascia lata routed between the clavicle and the sternum.
* Tendon Transfers: Burrows recommended the use of the subclavius tendon to tether the medial clavicle.
* Subperiosteal Dissection: Booth and Roper recommended a subperiosteal dissection of the sternal origin of the sternocleidomastoid (SCM) muscle, extending inferiorly with a strip of periosteum. This tendoperiosteal strip is threaded subperiosteally under the medial end of the first rib, passed behind the rib, and routed through a drill hole in the clavicle from superior to inferior, before being sutured back onto itself.
🚨 SURGICAL WARNING: The Danger of Metallic Fixation
Lunseth et al. previously modified SCJ procedures by adding a threaded Steinmann pin across the joint. This practice is now universally condemned. Numerous authors have documented the catastrophic migration of metallic fixation (K-wires, Steinmann pins) from the SCJ into the mediastinum, resulting in fatal cardiac tamponade, aortic puncture, and pulmonary injury. Metallic pins must never be used to stabilize the sternoclavicular joint.
The Evolution of Resection Arthroplasty
Resection of the medial end of the clavicle was historically recommended by Salvatore, DePalma, Rockwood, Bateman, and Milch. However, it is critical to emphasize that if the medial end of the clavicle is removed, the surgeon must meticulously preserve the costoclavicular (rhomboid) ligament.
Eskola et al. studied patients who underwent stabilization with fascial loops, tendon grafts, or isolated resection of the sternal end of the clavicle. They found that all patients treated by isolated resection of the medial end of the clavicle (without stabilization) yielded poor results, characterized by intractable pain and profound weakness in the upper extremity.
Therefore, Rockwood refined the approach: if surgery is unavoidable, he recommended resecting 1 inch (2.5 cm) of the medial clavicle, debriding the intra-articular disc ligament, and—crucially—stabilizing the remaining clavicle to the first rib using a 3-mm cotton Dacron tape or a robust strip of autogenous fascia. He also advocated for the detachment of the clavicular head of the sternocleidomastoid to temporarily neutralize the superior deforming force exerted by this muscle on the clavicle.
POSTERIOR STERNOCLAVICULAR DISLOCATIONS
Pathoanatomy and Mediastinal Risk
Posterior dislocation of the SCJ is an uncommon but potentially life-threatening injury. It typically occurs via a direct blow to the anteromedial clavicle or an indirect force applied to the posterolateral shoulder, driving the shoulder anteriorly and levering the medial clavicle posteriorly into the mediastinum.
In a chronic or acute unreduced state, posterior dislocation can be severely disabling. Worman and Leagus reviewed the literature on chronic retrosternal dislocations; alarmingly, 16 of 60 patients suffered severe complications involving the trachea, esophagus, or great vessels. Diagnosis was delayed in one-third of the patients, and intrathoracic injury occurred in 25% of cases.
Clinical Complications
- Dysphagia: The most common complication, resulting from direct mechanical pressure on the esophagus.
- Respiratory Compromise: Cough, stridor, and dyspnea due to tracheal compression.
- Neurovascular Injury: Compression or laceration of the subclavian vessels, brachiocephalic vein, or brachial plexus.
- Thoracic Outlet Syndrome: Gangahar and Flogataites, as well as Jain et al., described thoracic outlet syndrome caused by posterior SCJ dislocation. Jain successfully treated this via transaxillary resection of the first rib.
- Other: Rupture of the thoracic duct, pneumothorax, and subcutaneous emphysema.
Preoperative Evaluation and Multidisciplinary Approach
Given the high morbidity and potential mortality, open reduction of a posterior dislocation is almost always indicated if closed reduction fails or if the injury is chronic.
1. Imaging: A preoperative CT scan (preferably a CT angiogram) is mandatory to evaluate the exact position of the medial clavicle relative to the mediastinal structures.
2. Consultation: A thoracic or vascular surgeon must be consulted and ideally available on standby during the procedure, as catastrophic hemorrhage can occur upon dislodging the clavicle from the great vessels.
If the reduction is highly unstable or cannot be safely achieved due to chronic soft-tissue contractures, Gangahar and Flogataites recommended resecting the medial half of the clavicle. Aside from a cosmetic defect, they noted no significant functional disability from this extensive resection, provided the scapulothoracic mechanics remained intact.
SURGICAL TECHNIQUE: RESECTION OF THE MEDIAL END OF THE CLAVICLE AND STABILIZATION
When operative intervention is definitively indicated (e.g., chronic symptomatic anterior instability failing conservative care, or irreducible posterior dislocations), resection arthroplasty combined with first-rib stabilization is the procedure of choice.
Preoperative Positioning
- Anesthesia: General endotracheal anesthesia is required.
- Positioning: The patient is placed in the beach-chair position or supine with a bump between the scapulae to allow the shoulders to fall posteriorly, opening the anterior chest wall.
- Preparation: The entire forequarter, neck, and anterior chest must be prepped and draped to allow for extensile exposure and potential median sternotomy if vascular complications arise.
Step-by-Step Surgical Approach (Technique 58-6)
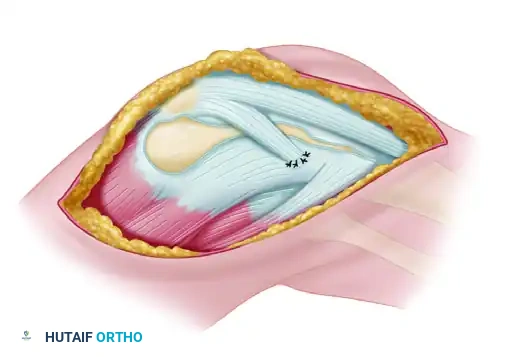
1. Exposure and Dissection
* Expose the medial end of the clavicle subperiosteally through a transverse incision approximately 6 cm long, running parallel to the superior border of the bone.
* Divide the platysma in line with the incision. Identify and protect the supraclavicular nerves where possible.
* Incise the periosteum longitudinally and elevate it meticulously.
2. Mobilization of the Medial Clavicle
* Free the medial end of the bone. Grasp it securely with a towel clip or robust bone forceps.
* Lift the clavicle anteriorly and superiorly. Carefully clear it of soft-tissue attachments posteriorly using a periosteal elevator.
* Surgical Pearl: Always keep the elevator directly on the bone to avoid plunging into the mediastinum or injuring the subclavian vein, which lies immediately posteroinferior to the subclavius muscle.
3. Assessment of the Costoclavicular Ligament
* Evaluate the integrity of the costoclavicular (rhomboid) ligaments. In chronic dislocations, these are usually torn or severely attenuated.
* If the ligaments are attached but stretched, resect only that part of the clavicle medial to these ligaments to preserve their stabilizing function.
* If the ligaments are completely torn or incompetent, plan to resect approximately 2 to 2.5 cm of the medial bone.
4. Osteotomy and Resection
* Protect the posterior structures by passing a malleable retractor or a blunt Darrach retractor behind the clavicle.
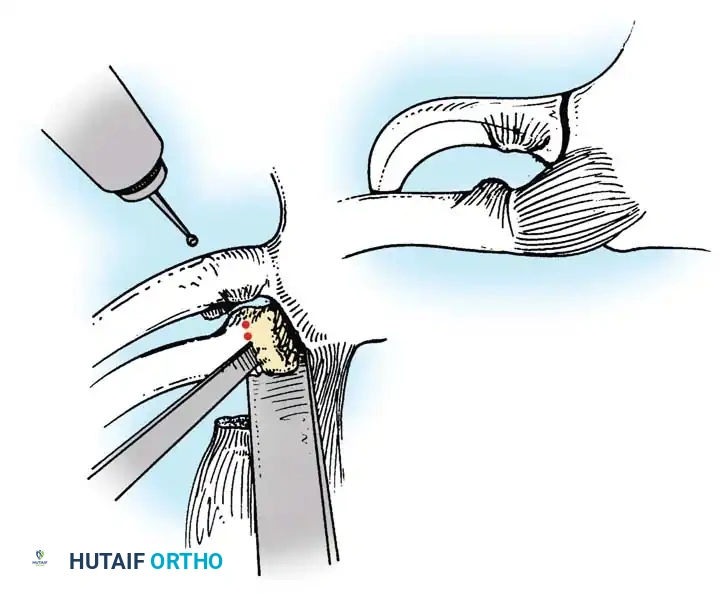
* Outline the site of the osteotomy with a drill to prevent splintering, and then resect 2.5 cm of bone using a sharp osteotome or an oscillating saw.
Fig. 58-4 Technique for resecting medial end of clavicle. A, Site of osteotomy is outlined with drill, and 2.5 cm of bone is then resected with osteotome. B, Periosteum is plicated and closed around remaining medial end of clavicle.
- Bevel the anterosuperior corner of the remaining lateral clavicular stump using a rongeur or rasp. This is a critical cosmetic step that prevents the sharp edge of the osteotomy from tenting the skin.
5. Stabilization to the First Rib
* Because isolated resection leads to poor outcomes (as shown by Eskola et al.), stabilization is mandatory if instability is present.
* Stabilize the remaining clavicle to the first rib using a 3-mm cotton Dacron tape, a robust semitendinosus allograft, or a strip of autogenous fascia lata.
* Carefully dissect subperiosteally around the first rib. Pass a right-angle clamp or a specialized ligature carrier under the first rib from anterior to posterior, staying strictly subperiosteal to avoid the underlying pleura and subclavian vessels.
* Pass the graft or tape under the first rib and through drill holes made in the remaining medial clavicle (or in a figure-of-eight fashion around it).
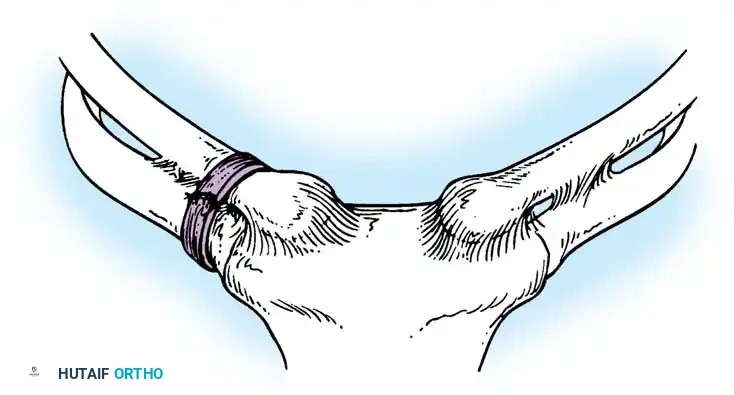
Fig. 58-5 Stabilization of clavicle to first rib with fascial loops. The graft is passed securely around the first rib and the clavicular stump to recreate the costoclavicular tether.
6. Soft Tissue Closure and SCM Detachment
* Detach the clavicular head of the sternocleidomastoid muscle from its insertion. This eliminates the superior deforming force that threatens to pull the clavicle upward and stress the newly reconstructed ligaments.
* Plicate the remaining periosteal sleeve and capsule tightly over the resected end of the clavicle.
* Close the platysma and skin in layers.
Postoperative Aftertreatment and Rehabilitation
Meticulous postoperative care is essential to protect the soft-tissue reconstruction while it heals.
- Phase I (0 to 3 Weeks): The shoulder girdle is strictly immobilized in a Velpeau-type dressing or a well-fitted shoulder immobilizer. The patient is instructed to avoid any active elevation or abduction of the shoulder. Elbow, wrist, and hand range of motion (ROM) are encouraged.
- Phase II (3 to 6 Weeks): The immobilizer is discontinued. A progressive, supervised active-assisted range-of-motion exercise program is initiated. Forward elevation is typically limited to 90 degrees during this phase to prevent excessive rotational stress on the SCJ reconstruction.
- Phase III (6 to 12 Weeks): Full active ROM is gradually restored. Isometric strengthening of the periscapular stabilizers (trapezius, rhomboids, serratus anterior) is emphasized to ensure optimal scapulothoracic rhythm, which unloads the sternoclavicular joint.
- Return to Play: Heavy manual labor and contact sports are generally restricted for a minimum of 4 to 6 months postoperatively, pending clinical stability and radiographic healing.
Pitfall: Failure to adequately immobilize the patient for the first 3 weeks is the leading cause of graft stretching and recurrent instability. Patient compliance must be strictly enforced.
CONCLUSION
The sternoclavicular joint presents unique challenges to the orthopedic surgeon. While anterior dislocations are best managed with reassurance and nonoperative "skillful neglect," posterior dislocations demand high clinical suspicion, advanced imaging, and prompt surgical reduction due to the peril they pose to mediastinal structures. When surgical reconstruction is undertaken, the absolute avoidance of transarticular pins, the judicious resection of the medial clavicle, and the meticulous ligamentous reconstruction to the first rib form the triad of a successful, evidence-based surgical outcome.
📚 Medical References
- Sternoclavicular joint dislocation, Clin Orthop Relat Res 58:51, 1968.
- Stankler L: Posterior dislocation of the clavicle: a report of two cases, Br J Surg 50:164, 1962.
- Weaver JK, Dunn HK: Treatment of acromioclavicular injuries, especially complete acromioclavicular separation, J Bone Joint Surg 54A:1187, 1972.
- Worman LW, Leagus C: Intrathoracic injury following retrosternal dislocation of the clavicle, J Trauma 7:416, 1967.
- Shoulder Chaudhuri GK, Sengupta A, Saha AK: Rotation osteotomy of the humerus for recurrent dislocation of the shoulder: anterior and posterior, Acta Orthop Scand 45:193, 1974.
- Connolly JF: Humeral head defects associated with shoulder dislocations: their diagnostic and surgical signifi cance, Instr Course Lect 21:42, 1972.
- Delcogliano A, Caporaso A, Chiossi, S, et al: Surgical management of chronic, unreduced posterior dislocation of the shoulder, Knee Surg Sports Traumatol Arthrosc 13:151, 2005.
- DePalma AF: Surgery of the shoulder, Philadelphia, 1950, JB Lippincott. Goga IE:
You Might Also Like