Acute Anterior Glenohumeral Dislocations
The glenohumeral joint, owing to its shallow glenoid fossa and reliance on soft-tissue restraints, is the most frequently dislocated major joint in the human body. While uncomplicated dislocations of the shoulder rarely require open reduction, the management paradigm for first-time dislocators has evolved significantly. The decision-making process must account for patient age, activity level, pathoanatomy, and the presence of concurrent injuries.
Irreducible and Complex Dislocations
Although closed reduction is successful in the vast majority of acute anterior dislocations, a subset of these injuries proves irreducible.
Clinical Pearl: A shoulder dislocation that cannot be reduced under adequate conscious sedation or general anesthesia should immediately raise the suspicion of soft-tissue interposition or an obstructing osteochondral fragment. Repeated, forceful attempts at closed reduction in these scenarios are contraindicated and may result in iatrogenic neurovascular injury or iatrogenic fractures.
Seradge and Orme, as well as Kuhnen and Groves, have classically described acute anterior dislocations of the shoulder that were irreducible due to the interposition of the long head of the biceps tendon. In these cases, the biceps tendon slips posteriorly to the humeral head, creating a mechanical block to reduction. Furthermore, acute dislocations may be complicated by fracture fragments from the greater tuberosity or the anterior glenoid rim that become incarcerated within the joint space, preventing the humeral head from returning to its concentric position. These complex fracture-dislocations necessitate open reduction and internal fixation (ORIF) to restore articular congruity and stability.
Concurrent Rotator Cuff Tears in the Older Patient
The demographic profile of the patient is a critical determinant of associated pathology. While young patients typically sustain capsulolabral avulsions (Bankart lesions), patients over the age of 40 are at a significantly higher risk for concurrent rotator cuff tears.
Neviaser et al. reported on a cohort of 31 patients, the majority of whom were older than 40 years, who sustained rotator cuff tears in addition to acute shoulder dislocations.
Surgical Warning: Rotator cuff tears must be highly suspected when profound weakness in abduction or external rotation persists after successful shoulder reduction. Do not attribute this weakness solely to axillary nerve neurapraxia without thorough investigation.
In the Neviaser cohort, the diagnosis of a massive rotator cuff tear was confirmed via arthrography (though modern practice favors MRI). Without intervention, eight of these patients developed chronic instability. Ultimately, all 31 patients required surgical rotator cuff repair to restore function and stability. The loss of the compressive forces provided by the rotator cuff severely destabilizes the glenohumeral joint, making early diagnosis and repair paramount in the older demographic.
Pathoanatomy and Biomechanics of Instability
Understanding the specific intraarticular lesions generated during a first-time dislocation is essential for predicting recurrence and planning surgical intervention. In a landmark effort to determine which shoulders are prone to recurrent dislocation, Baker et al. identified and classified intraarticular lesions in 45 patients with first-time anterior glenohumeral dislocations.
Based on examination under anesthesia (EUA) and diagnostic arthroscopy, Baker et al. classified these shoulders into three distinct pathoanatomic groups:
- Group 1 (6 patients): Characterized by isolated capsular tears with no labral lesions. On EUA, these shoulders were stable. Arthroscopically, hemorrhage was present in the inferior capsule between the middle and inferior glenohumeral ligaments (IGHL). No Hill-Sachs lesions were identified. These represent capsular sprains with a low risk of recurrence.
- Group 2 (11 patients): Characterized by subluxable shoulders on EUA. Arthroscopy revealed partial detachment of the labrum from the glenoid rim and the IGHL attachment to the biceps insertion. Hill-Sachs lesions were identified in this group, indicating a more significant translation of the humeral head over the glenoid rim.
- Group 3 (28 shoulders): Characterized by gross instability on EUA. Arthroscopy demonstrated complete disruption of the IGHL insertion anteriorly (a classic Bankart lesion). Deep, engaging Hill-Sachs lesions were also universally seen in this group.
This classification underscores that the severity of the initial capsulolabral injury directly correlates with the degree of clinical instability and the likelihood of recurrent dislocation.
Management Strategies: Nonoperative vs. Operative
The traditional approach of immobilizing all first-time dislocators has been challenged by prospective data demonstrating unacceptably high recurrence rates in young, active populations. We currently favor initial nonoperative management for first-time dislocations in older or sedentary patients, but consider arthroscopic stabilization procedures an appropriate, and often superior, alternative in selected young athletes.
Evidence for Early Arthroscopic Stabilization
Multiple high-level studies have demonstrated the efficacy of early surgical intervention in preventing recurrent instability:
- Arciero et al.: Prospectively divided acute anterior shoulder dislocations into surgical (21 patients) and nonsurgical (15 patients) groups. Of the nonsurgical group, a staggering 80% developed recurrent instability at an average of 10 months post-injury, with many ultimately requiring open repair. Conversely, the surgical group (treated with transglenoid arthroscopic suturing) achieved an 80% success rate at a mean follow-up of 32 months. Only one patient required an open Bankart repair after a repeat dislocation.
- Bottoni and Arciero et al.: In a similar prospective study, found an 11.1% recurrence rate after acute arthroscopic stabilization in 10 patients at a mean follow-up of 36 months, compared to a 75% recurrence rate in 14 patients treated nonoperatively.
- DeBerardino et al.: Reported on the arthroscopic stabilization of 49 acute anterior shoulder dislocations in young, high-demand athletes. They noted only six failures (12%) at a mean follow-up of 37 months (range 30 to 100 months).
- Salmon and Bell: Treated 17 patients with acute primary anterior shoulder dislocations using an arthroscopic transglenoid suture technique. They reported only one recurrent dislocation at the latest follow-up. Crucially, 9 of the 16 patients without recurrence were able to return to the same or a higher level of athletic activity.
Based on these data, arthroscopic intervention is highly recommended in active, young patients (typically under 25 years of age) with no prior history of subluxation or impingement, as they possess the highest statistical probability of recurrent dislocations.
Acromioclavicular (AC) Joint Separations
While glenohumeral dislocations involve the articulation between the humeral head and the glenoid, injuries to the superior shoulder girdle frequently involve the acromioclavicular (AC) joint. AC joint separations are typically the result of a direct blow to the superior aspect of the acromion with the arm adducted, driving the acromion inferiorly while the clavicle remains stabilized by the sternocleidomastoid muscle.
Biomechanics of the AC Joint
Stability of the AC joint is provided by two distinct ligamentous complexes:
1. Acromioclavicular (AC) Ligaments: Provide horizontal (anterior-posterior) stability. The superior AC ligament is the most robust.
2. Coracoclavicular (CC) Ligaments: Consisting of the conoid (medial) and trapezoid (lateral) ligaments, these provide vertical (superior-inferior) stability.
Disruptions are classified by the Rockwood system (Types I-VI). Types I and II are managed nonoperatively. Type III is controversial, often managed nonoperatively in the general population but surgically in overhead athletes or manual laborers. Types IV, V, and VI require surgical reconstruction due to severe displacement and fascial disruption.
The Stewart Technique for Acute AC Dislocation
Historically, acute AC joint dislocations were managed with direct transarticular fixation to hold the joint reduced while the ligaments healed. The Stewart technique is a classic example of this approach, utilizing rigid pin fixation across the acromioclavicular articulation.
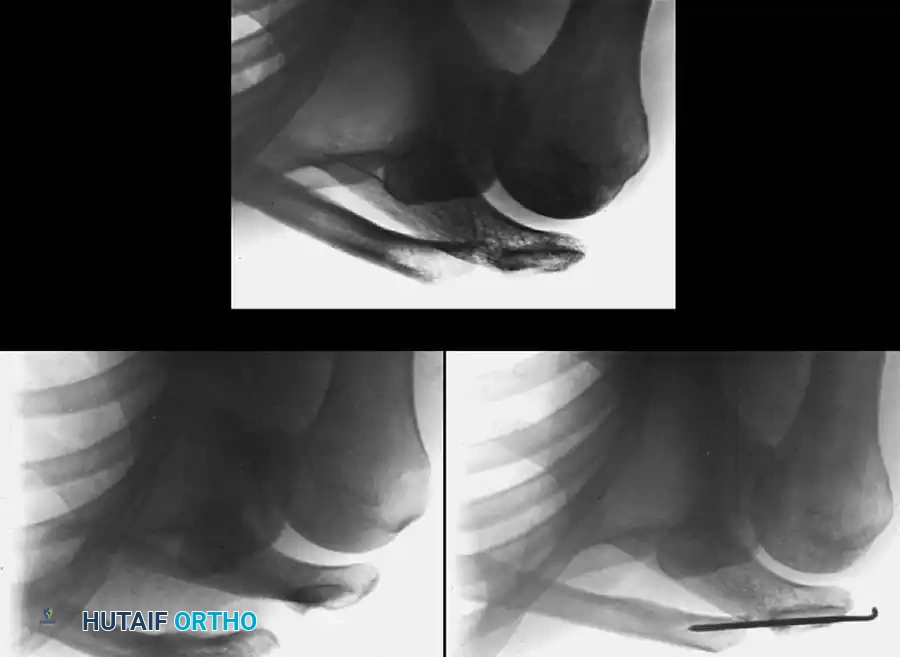
Fig. 57-19 Stewart technique for acute dislocation of acromioclavicular joint. A, Soon after injury. B, Six weeks after surgery. C, Three months after surgery.
Surgical Steps for Transarticular Pinning:
1. Positioning: The patient is placed in the beach chair position.
2. Incision: A superior approach is made over the distal clavicle and AC joint.
3. Reduction: The AC joint is debrided of any interposed meniscus or frayed ligamentous tissue. The clavicle is reduced anatomically in both the horizontal and vertical planes.
4. Fixation: Heavy Kirschner wires or Steinmann pins are driven from the lateral aspect of the acromion, across the AC joint, and into the medullary canal of the distal clavicle.
5. Postoperative Care: The pins are typically removed at 6 weeks (as seen in Fig. 57-19 B) to prevent hardware breakage, allowing for fibrous healing of the joint (Fig. 57-19 C).
Pitfall: Transarticular AC joint pinning carries a known risk of pin migration, which can be catastrophic if pins migrate medially into the thoracic cavity or neurovascular structures. Modern techniques often favor CC ligament reconstruction over transarticular AC pinning to avoid this complication.
The Weaver-Dunn Procedure for AC Joint Reconstruction
For chronic AC joint separations, or severe acute separations (Types IV-VI), primary repair of the CC ligaments is often insufficient due to poor tissue quality. The Weaver-Dunn procedure, originally described in 1972, remains a foundational technique for reconstructing the CC ligament complex by transferring the coracoacromial (CA) ligament.
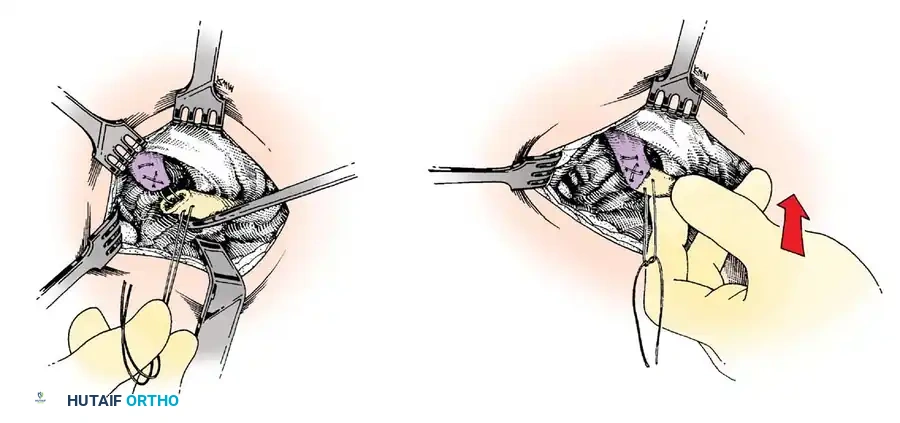
Fig. 57-20 Technique of Weaver and Dunn for acromioclavicular separations (see text). (Redrawn from Weaver JK, Dunn HK: Treatment of acromioclavicular injuries, especially complete acromioclavicular separation, J Bone Joint Surg 54A:1187, 1972.)
Step-by-Step Surgical Technique:
- Patient Positioning and Approach:
- The patient is placed in the beach chair position.
- A saber incision is made starting at the posterior edge of the clavicle, extending anteriorly over the coracoid process.
- Distal Clavicle Excision:
- The distal 1 to 1.5 cm of the clavicle is excised. This prevents future AC joint arthrosis and creates space for the reduction. Care is taken to preserve the superior deltotrapezial fascia for later meticulous repair.
- Harvesting the CA Ligament:
- The coracoacromial (CA) ligament is identified. It is detached from its insertion on the undersurface of the acromion, often taking a small fleck of bone to enhance healing.
- The ligament is mobilized, leaving its origin on the coracoid process intact. Heavy non-absorbable sutures (e.g., #2 FiberWire) are woven into the free end of the CA ligament using a Krackow or whipstitch technique.
- Ligament Transfer and Fixation:
- The distal end of the clavicle is prepared by drilling a medullary hole or creating bone tunnels.
- The clavicle is reduced inferiorly to its anatomic position relative to the coracoid.
- The free end of the CA ligament is transferred into the medullary canal of the distal clavicle and secured via the pre-placed sutures through superior drill holes (as depicted in Fig. 57-20).
- Augmentation (Modern Modification):
- Because the native CA ligament is only about 25% as strong as the native CC ligaments, the classic Weaver-Dunn procedure is almost universally augmented in modern practice. This is achieved using heavy suture cerclage, cortical buttons, or suture anchors passed around or through the coracoid and clavicle to protect the CA ligament transfer while it heals.
- Closure:
- The deltotrapezial fascia is meticulously imbricated and repaired over the distal clavicle. This fascial repair is critical for dynamic stability of the shoulder girdle.
Postoperative Rehabilitation Protocol
Whether undergoing arthroscopic Bankart repair for glenohumeral instability or a Weaver-Dunn reconstruction for AC separation, strict adherence to a phased rehabilitation protocol is mandatory.
- Phase I (0-4 Weeks): Absolute immobilization in a sling. For AC joint reconstructions, a sling that supports the elbow to push the humerus and scapula upward (relieving tension on the CC repair) is utilized. Pendulum exercises are permitted, but active elevation and cross-body adduction are strictly prohibited.
- Phase II (4-8 Weeks): Sling is discontinued. Passive range of motion (PROM) and active-assisted range of motion (AAROM) are initiated. For anterior stabilization, external rotation is limited to 30 degrees to protect the anterior capsulolabral repair.
- Phase III (8-12 Weeks): Active range of motion (AROM) is progressed. Isotonic strengthening of the rotator cuff and periscapular stabilizers begins.
- Phase IV (3-6 Months): Advanced strengthening, plyometrics, and sport-specific training. Return to contact sports is generally delayed until 6 months postoperatively, contingent upon the restoration of symmetric strength and dynamic stability.
