INTRODUCTION TO PATELLAR TENDON REPAIR
Disruption of the extensor mechanism via patellar tendon rupture is a profoundly debilitating injury that mandates prompt surgical intervention to restore knee kinematics and ambulatory function. Historically, the gold standard for repairing avulsions of the patellar tendon from the inferior patellar pole or the tibial tubercle involved the use of transosseous bone tunnels. However, the evolution of orthopedic biomaterials and biomechanical understanding has led to the widespread adoption of suture anchor repair techniques.
Pioneered and refined by surgeons such as DeBerardino and Owens, the suture anchor technique offers several distinct biomechanical and biological advantages. It eliminates the need for large transosseous tunnels, thereby preserving bone stock—a critical factor if revision surgery is ever required. Furthermore, suture anchors allow for a more anatomic restoration of the tendon footprint, providing superior compression of the tendon against the decorticated bone bed, which optimizes the biological environment for healing. This comprehensive guide details the surgical management of acute and chronic patellar tendon ruptures, focusing on the suture anchor technique, complex reconstructions, and evidence-based postoperative protocols.
SURGICAL ANATOMY AND BIOMECHANICS
A profound understanding of the extensor mechanism's anatomy is prerequisite for anatomic repair. The patellar tendon originates from the inferior pole of the patella, spanning a crescent-shaped footprint that is wider anteriorly than posteriorly. It inserts distally onto the proximal tibial tubercle.
Biomechanically, the patellar tendon must withstand extraordinary tensile forces, often exceeding several times the patient's body weight during activities such as jumping, descending stairs, or deep flexion.
💡 Clinical Pearl: The Footprint
The proximal origin of the patellar tendon is not merely at the distal tip of the patella but extends proximally along the anterior surface of the inferior pole. Decortication and anchor placement must respect this broad, crescentic footprint to prevent elongation of the repair and subsequent patella alta.
When a rupture occurs, it typically manifests in one of three patterns:
1. Proximal Avulsion: The most common pattern, occurring at the osteotendinous junction of the inferior patellar pole.
2. Distal Avulsion: Less common, occurring at the insertion on the tibial tubercle.
3. Midsubstance Rupture: Often associated with underlying tendinopathy, systemic diseases (e.g., lupus, chronic renal failure), or prolonged corticosteroid use.
PREOPERATIVE EVALUATION AND IMAGING
Accurate preoperative planning dictates the success of the surgical intervention.
Clinical Examination
Patients typically present with a palpable infrapatellar gap, an inability to perform an active straight-leg raise, and a high-riding patella (patella alta). Hemarthrosis and significant localized edema are universally present in acute settings.
Radiographic Assessment
Standard orthogonal radiographs (AP and Lateral) are mandatory.
* Lateral Radiograph: Crucial for assessing patellar height. Indices such as the Insall-Salvati ratio or the Caton-Deschamps index should be calculated.
* Contralateral Comparison: For chronic ruptures (>6 weeks), lateral radiographs of the uninvolved extremity must be obtained with the knee flexed to exactly 45 degrees. This provides a patient-specific template for the appropriate patellar height during reconstruction.
Advanced Imaging
While the diagnosis is often clinical, Magnetic Resonance Imaging (MRI) is highly valuable for assessing the quality of the remaining tendon tissue, identifying midsubstance degeneration, and ruling out concomitant intra-articular pathology.
SURGICAL TECHNIQUE: REPAIR WITH SUTURE ANCHORS
The following technique, described by DeBerardino and Owens, provides a robust, biomechanically sound repair utilizing modern suture anchors.
Patient Positioning and Anesthesia
- Anesthesia: General or regional anesthesia is utilized based on patient comorbidities and anesthesiologist preference. Muscle relaxation is critical to allow for distal mobilization of the extensor mechanism.
- Positioning: The patient is placed supine on the operating table. A high-thigh tourniquet is applied.
- Preparation: The operative extremity is prepped and draped in a standard sterile fashion. A sterile bump may be placed under the knee to maintain slight flexion during the approach.
Surgical Approach and Dissection
- Incision: Utilize a midline longitudinal incision centered over the patellar tendon, extending from the lower third of the patella to just distal to the tibial tubercle.
- Peritenon Management: Carefully incise the peritenon longitudinally. It is imperative to dissect it away from the underlying tendon meticulously.
> ### ⚠️ Surgical Warning: Peritenon Preservation
> The peritenon carries the primary vascular supply to the healing tendon. It must be preserved and retracted gently to allow for a robust biological closure over the repair at the conclusion of the procedure. - Debridement: Thoroughly irrigate the hematoma. Débride or resect any grossly pathologic, degenerative, or necrotic tendon tissue. Decorticate the bony footprint (either the inferior patella or tibial tubercle) using a rongeur or a high-speed burr to expose a bleeding cancellous bone bed, which is essential for osteotendinous integration.
Scenario A: Midsubstance Ruptures
For ruptures occurring in the midsubstance of the tendon:
1. Expose the full length of the tendon.
2. Place two locking Krackow stitches in each tendon stump (proximal and distal). Utilize heavy, No. 2 or No. 5 nonabsorbable braided sutures.
3. With the knee held in full extension, tie the four proximal core sutures directly to the corresponding distal sutures, ensuring symmetric tension.
4. Repair the medial and lateral retinaculum meticulously with heavy absorbable sutures (e.g., No. 1 Vicryl) to offload the central tendon repair.
Scenario B: Proximal Avulsion from the Patella
For avulsions from the inferior patellar pole, the suture anchor technique is highly effective.
- Footprint Preparation: Expose the inferior patellar pole and decorticate the anatomic footprint.
- Anchor Placement: Place three double-loaded or triple-loaded suture anchors equidistant along the anatomic tendon footprint of the inferior patella. Ensure the anchors are seated flush with the cortical bone to prevent prominence.
- Suture Configuration: Pull the suture through the anchor eyelet to produce long and short suture arms.
- Tendon Grasping: Pass the long suture arm down and back up through the substance of the proximal tendon stump in a locking Krackow fashion.
- Reduction and Fixation: Use the short arm of the suture to act as a pulley, reducing the tendon directly to the decorticated patellar footprint.
- Knot Tying: Tie each suture repair securely while an assistant holds the patella reduced distally with a towel clip or tenaculum, and the knee is in full extension.
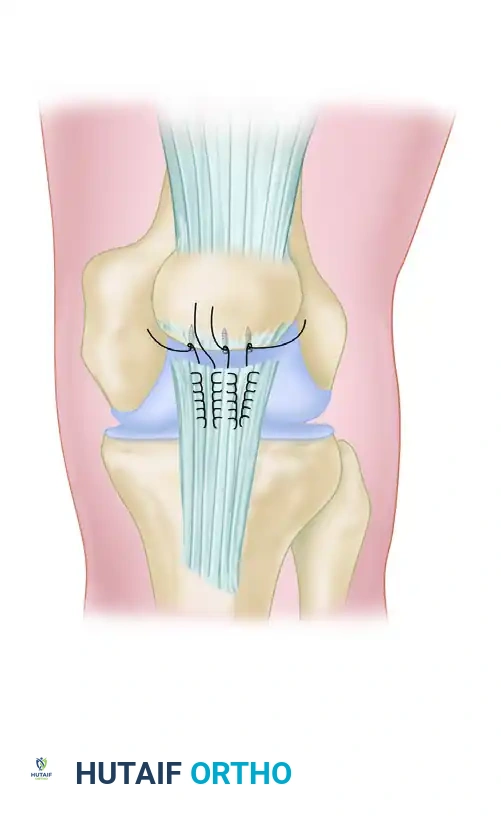
FIGURE 48-34A: Repair of patellar tendon avulsion with suture anchors. For proximal avulsions, three suture anchors are placed in the anatomic tendon footprint of the inferior patella. The sutures are passed in a locking fashion to secure the tendon to the bone.
Scenario C: Distal Avulsion from the Tibial Tubercle
For distal avulsions, the biomechanical principles remain identical, but the fixation is reversed.
- Footprint Preparation: Decorticate the anatomic footprint on the proximal tibial tubercle.
- Anchor Placement: Place the suture anchors directly into the solid bone of the tibial tubercle.
- Tendon Grasping and Reduction: Utilize the same long-arm Krackow technique described above, passing the sutures proximally into the distal tendon stump. Reduce the tendon distally to the tubercle and tie securely.
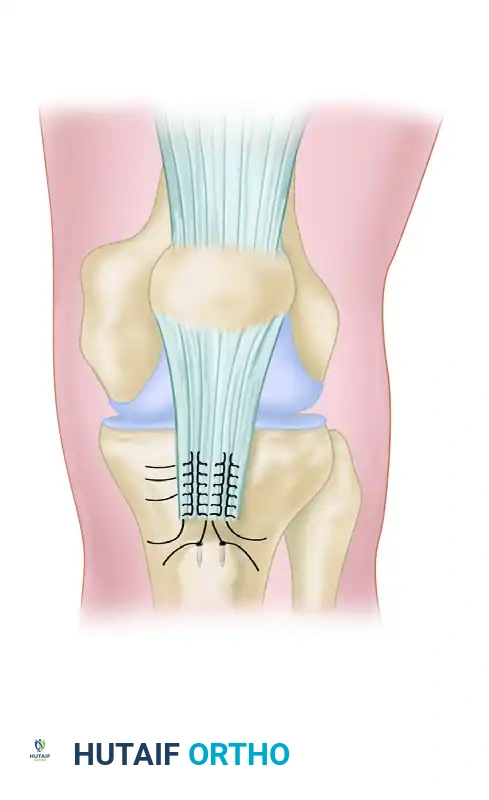
FIGURE 48-34B: Repair of patellar tendon avulsion with suture anchors. For distal avulsions, suture anchors are placed directly into the tibial tubercle, and the tendon is repaired down to the anatomic footprint.
Assessment and Closure
- Gap Formation Check: Once the repair is tied and the retinaculum is closed, gently flex the knee to 45–90 degrees (depending on the tension of the repair) to check for gap formation and assess the safe range of motion for postoperative rehabilitation.
- Peritenon Closure: Close the preserved peritenon over the repaired tendon using fine absorbable sutures. This step is vital for restoring the vascular envelope and preventing subcutaneous adhesions.
- Skin Closure: Close the subcutaneous tissues and skin in a standard layered fashion.
TREATMENT OF CHRONIC PATELLAR TENDON RUPTURES
The management of a patellar tendon rupture that is more than 6 weeks old presents a formidable surgical challenge. In chronic settings, the extensor mechanism undergoes severe contracture, and the patella retracts proximally, becoming encased in dense scar tissue.
Surgical Mobilization
Extensive surgical release is mandatory to draw the patella distally to the appropriate anatomic level.
* Historical Techniques: Previously, preoperative traction through a Kirschner wire placed transversely in the patella was recommended to stretch the quadriceps over several weeks.
* Current Paradigm: Modern orthopedic consensus favors intraoperative proximal release of scar tissue. If the patella cannot be mobilized distally, a modified Thompson quadricepsplasty is indicated. This involves releasing the vastus lateralis and medialis from the rectus femoris, and occasionally releasing the rectus femoris from the anterior joint capsule.
Establishing Patellar Height
Intraoperative fluoroscopy is essential. The patellar height must be compared to the preoperative lateral radiographs of the uninvolved extremity (taken at 45 degrees of flexion) to ensure anatomic restoration and prevent iatrogenic patella infera or alta.
Augmentation and Reconstruction
Primary repair is rarely sufficient in chronic cases due to tissue retraction and degeneration.
1. Autograft Augmentation: If sufficient native patellar tendon remains, the repair must be augmented. The ipsilateral semitendinosus or gracilis tendon can be harvested, left attached distally at the pes anserinus, and routed through a transverse drill hole in the patella to frame and protect the primary repair.
2. Allograft Reconstruction: If the rupture is several months old and the native tissue is unsalvageable, an allograft reconstruction is required. An Achilles tendon allograft with a calcaneal bone block is the graft of choice. The bone block is press-fit into a trough created in the tibial tubercle, and the tendinous portion is woven through and sutured over the patella and quadriceps tendon.
POSTOPERATIVE CARE AND REHABILITATION
The postoperative protocol must balance the protection of the healing osteotendinous junction with the prevention of arthrofibrosis. The stability of the intraoperative tendon repair directly dictates the aggressiveness of the rehabilitation.
Phase I: Maximum Protection (Weeks 0 to 6)
- Weight Bearing: Weight bearing as tolerated (WBAT) is allowed immediately, provided the knee is locked in a hinged knee brace in full extension.
- Range of Motion (ROM): Early flexion is allowed via active-assisted range of motion (AAROM) and passive range of motion (PROM), strictly guided by the intraoperative safe zone.
- ROM Goals: The goal is to achieve 90 degrees of flexion by 4 to 6 weeks.
- Muscle Activation: Isometric quadriceps contractions (quad sets) can be initiated immediately after surgery to prevent severe atrophy.
Phase II: Moderate Protection (Weeks 6 to 12)
- Brace Weaning: The hinged brace is gradually unlocked to allow functional ROM during ambulation, eventually weaning off the brace as quadriceps control improves.
- Strengthening: Straight-leg raises (SLR) without an extension lag should be achievable by 6 weeks. Closed kinetic chain exercises (e.g., mini-squats, leg presses) are initiated.
- ROM Goals: Progression to full, symmetric range of motion is expected by 10 to 12 weeks.
Phase III: Return to Function (Months 3 to 6+)
- Advanced Strengthening: Progression to unilateral strengthening, proprioception, and sport-specific drills.
- Return to Play: Full return to high-impact activities or sports is strictly prohibited for a minimum of 6 months, and is contingent upon achieving >90% strength symmetry on isokinetic testing and the absence of an extensor lag.
COMPLICATIONS AND PITFALLS
Surgeons must be vigilant regarding potential complications associated with patellar tendon repair:
* Re-rupture: The most devastating complication, often resulting from patient non-compliance, aggressive early flexion, or inadequate initial fixation. Suture anchor techniques significantly reduce this risk compared to traditional methods.
* Arthrofibrosis and Stiffness: Prolonged immobilization leads to severe stiffness. The modern approach of early, protected ROM is critical to mitigating this risk.
* Patella Infera/Alta: Over-tensioning the repair leads to patella infera, causing anterior knee pain and altered patellofemoral contact pressures. Under-tensioning leads to patella alta and an extensor lag. Meticulous intraoperative assessment of the contralateral knee template is the best preventative measure.
* Infection: Given the subcutaneous nature of the anterior knee, meticulous soft tissue handling and peritenon closure are vital to prevent wound dehiscence and deep infection.
