Repairing Chronic Knee Medial Ligament Injuries: Your Path to Recovery

Key Takeaway
Here are the crucial details you must know about Repairing Chronic Knee Medial Ligament Injuries: Your Path to Recovery. A chronic knee medial collateral ligament (MCL) injury typically stems from valgus stress or forced external rotation on the knee. This mechanism can disrupt both superficial and deep MCL layers, frequently alongside injuries to structures like the ACL or posteromedial corner. It can be partial or complete, requiring specific repair considerations.
Introduction and Epidemiology
Injuries to the medial collateral ligament complex represent the most common ligamentous pathology of the knee joint. While the majority of acute medial-sided knee injuries resolve with nonoperative management, severe high-grade tears, multi-ligamentous knee injuries, and chronic medial instability present significant clinical challenges that necessitate surgical intervention. The medial collateral ligament is frequently injured in athletic populations due to a direct valgus stress acting upon the knee joint with the foot planted.
Forced external rotation injuries coupled with a valgus component have also been described as a primary mechanism capable of disrupting the medial collateral ligament complex. While a direct, isolated valgus force is more likely to injure the superficial medial collateral ligament, the addition of external rotation and valgus stress often causes concomitant injuries to the deep medial collateral ligament, the anterior cruciate ligament, the posteromedial corner, and the posterior oblique ligament. Epidemiological data indicates that the most common combined multi-ligamentous knee injury is an anterior cruciate ligament tear paired with a medial collateral ligament injury, followed closely by associated meniscal pathology.
Pathogenesis and Mechanism of Injury
The pathogenesis of medial knee injuries dictates the natural history and subsequent treatment algorithm. Medial collateral ligament injuries can be classified as partial or complete. A complete injury involves the disruption of both the superficial and deep medial collateral ligament layers, usually resulting in an immediate inability to ambulate and profound valgus instability.
Furthermore, the anatomical location of the tear—whether femoral-sided, mid-substance, or tibial-sided—profoundly affects the healing potential. Femoral-sided medial collateral ligament ruptures exhibit a robust healing response due to the highly vascularized surrounding soft tissue envelope. Conversely, complete tibial-sided avulsions, particularly those involving a distal retraction of the superficial medial collateral ligament over the pes anserinus tendons (often referred to as a Stener-like lesion of the knee), are significantly less likely to achieve functional competence with nonoperative management. These specific injury patterns frequently require acute surgical repair or chronic reconstruction to restore medial compartment stability.
Surgical Anatomy and Biomechanics
A profound understanding of the medial knee anatomy is an absolute prerequisite for successful surgical intervention. The medial side of the knee is classically divided into three distinct anatomical layers, as initially described by Warren and Marshall.

Layered Anatomy of the Medial Knee
Layer I consists of the deep crural fascia, which extends from the quadriceps fascia proximally and blends into the tibial periosteum distally. This layer envelopes the sartorius muscle and serves as the most superficial investing fascia of the medial knee.
Layer II contains the primary static stabilizers of the medial knee, specifically the superficial medial collateral ligament and the medial patellofemoral ligament. The superficial medial collateral ligament is a robust, flat band originating from the medial femoral epicondyle, located slightly proximal and posterior to the anatomical center of the epicondyle. It courses distally to insert approximately 4 to 6 centimeters distal to the medial joint line on the anteromedial aspect of the tibia, deep to the pes anserinus tendons. The superficial medial collateral ligament is functionally divided into an anterior and a posterior portion. The anterior portion tightens progressively in knee flexion, whereas the posterior portion achieves maximal tension in full extension.
Layer III encompasses the deep medial collateral ligament and the critical structures of the posteromedial corner. The deep medial collateral ligament is a thickening of the medial joint capsule, subdivided into the meniscotibial and meniscofemoral ligaments. This deep structure tightens during knee flexion and remains relatively lax in full knee extension.
The Posteromedial Corner and Semimembranosus Complex
The posteromedial corner provides essential rotational stability to the medial side of the knee. Injuries to the posterior oblique ligament and associated structures precipitate profound anteromedial rotatory instability. The posterior oblique ligament is a fibrous extension of the distal semimembranosus tendon that blends with the posteromedial capsule.
The semimembranosus itself is a critical dynamic stabilizer, featuring five main distinct attachments to the posterior capsule and medial tibia:
1. Pars reflexa, attaching directly to the proximal medial tibia deep to the superficial medial collateral ligament.
2. Direct arm, attaching firmly to the posteromedial tibia.
3. Insertion to the proximal medial capsule.
4. Fibrous attachment integrating into the posterior oblique ligament.
5. Attachment to the popliteus aponeurosis.
Biomechanical Properties
Biomechanically, the superficial medial collateral ligament is the primary restraint to valgus stress across all degrees of knee flexion, providing up to 78 percent of the resisting force at 25 degrees of flexion. The deep medial collateral ligament acts as a secondary restraint to valgus stress. The posterior oblique ligament and the posteromedial capsule serve as the primary restraints to internal rotation near full extension and secondary restraints to valgus stress in full extension. Disruption of these structures leads to significant valgus gapping and anteromedial rotatory subluxation of the medial tibial plateau relative to the medial femoral condyle.
Indications and Contraindications
Acute isolated medial collateral ligament injuries (Grades I and II) are overwhelmingly treated nonoperatively with protective weight-bearing and functional bracing for 2 to 6 weeks. However, specific clinical scenarios dictate operative management. Complete tibial-sided avulsions, particularly those complicated by soft tissue interposition (pes anserinus), fail to heal at their anatomic footprint and require surgical fixation.

Chronic medial knee instability, defined as persistent symptomatic valgus laxity or anteromedial rotatory instability failing a minimum of 3 to 6 months of conservative management, is a primary indication for ligamentous reconstruction. Furthermore, high-grade medial collateral ligament injuries occurring in the setting of multi-ligamentous knee trauma (e.g., combined anterior cruciate ligament and complete medial collateral ligament tears with posterior oblique ligament extension) often warrant concurrent surgical management to prevent graft failure of the reconstructed cruciate ligaments.
| Clinical Scenario | Operative Indication | Non-Operative Indication |
|---|---|---|
| Grade I / II Isolated MCL Tear | Rarely indicated | Primary treatment (Bracing, early ROM) |
| Grade III Isolated Femoral Avulsion | Failure of conservative therapy, persistent laxity | Primary treatment (Hinged knee brace 4-6 weeks) |
| Grade III Isolated Tibial Avulsion | Retraction superficial to pes anserinus (Stener-like lesion) | Non-displaced, anatomic alignment maintained |
| Combined ACL / Grade III MCL | Persistent valgus laxity > 3 weeks, high-demand athlete | MCL heals conservatively, delayed ACL reconstruction |
| Chronic Valgus Instability | Symptomatic instability affecting activities of daily living | Low-demand patient, medically unfit for surgery |
| Multi-ligamentous Knee Injury (KD III/IV) | Acute repair/reconstruction of all injured structures | Extreme polytrauma precluding prolonged surgery |
Contraindications to surgical intervention include active local or systemic infection, severe uncorrected mechanical axis malalignment (e.g., severe genu valgum requiring osteotomy prior to or concurrent with ligamentous reconstruction), advanced medial compartment osteoarthritis, and complex regional pain syndrome.
Pre Operative Planning and Patient Positioning
Clinical Evaluation and Imaging
A meticulous patient history regarding the mechanism of injury must be elicited. The physical examination must include a comprehensive assessment of the medial structures. The valgus stress test is performed at both 0 degrees and 30 degrees of knee flexion. Laxity at 30 degrees isolates the superficial medial collateral ligament, while laxity at 0 degrees indicates a combined injury involving the superficial medial collateral ligament, the posterior oblique ligament, and potentially the cruciate ligaments. The dial test should be performed to assess for concurrent posterolateral corner injury, and the anterior drawer test in external rotation can help quantify anteromedial rotatory instability.

Standard radiographic evaluation includes weight-bearing anteroposterior, lateral, and Merchant views to assess for avulsion fractures (e.g., Pellegrini-Stieda lesion in chronic cases), joint space narrowing, and overall limb alignment. Valgus stress radiographs can objectively quantify medial compartment gapping compared to the contralateral uninjured knee; a side-to-side difference greater than 3.2 millimeters is highly indicative of a complete medial collateral ligament tear. Magnetic Resonance Imaging (MRI) is the gold standard for evaluating the precise anatomic location of the tear, the integrity of the posterior oblique ligament, and associated intra-articular pathology.
Operating Room Setup and Positioning
The patient is placed supine on the operating table. A thorough examination under anesthesia is performed to confirm the physical examination findings without muscle guarding. A proximal thigh tourniquet is applied.

Depending on surgeon preference and concurrent procedures (e.g., anterior cruciate ligament reconstruction), the leg may be placed in a standard leg holder or positioned freely with a lateral post to allow for dynamic assessment of valgus laxity and range of motion throughout the procedure. The contralateral limb is secured in sequential compression devices. Standard orthopedic preparation and draping are performed to allow exposure from the proximal thigh to the ankle.
Detailed Surgical Approach and Technique
Surgical Incision and Dissection
A longitudinal incision is made along the medial aspect of the knee, typically extending from the medial epicondyle to approximately 6 centimeters distal to the joint line, centered over the course of the superficial medial collateral ligament. Alternatively, a hockey-stick incision can be utilized for broader exposure of the posteromedial corner.
Dissection proceeds through the subcutaneous tissue to identify the deep crural fascia (Layer I). Meticulous hemostasis is maintained. The infrapatellar branch of the saphenous nerve and the main trunk of the saphenous nerve must be identified and carefully protected during the distal exposure. The fascia is incised longitudinally to expose the sartorius fascia.
While there is no true internervous plane on the medial side of the knee, surgical dissection often utilizes the interval between the sartorius (innervated by the femoral nerve) and the gracilis (innervated by the obturator nerve) to access the distal insertion of the superficial medial collateral ligament. The pes anserinus tendons are retracted distally and posteriorly to expose the full tibial footprint.
Acute Repair Techniques
For acute injuries requiring surgical intervention, direct repair is typically performed within the first 3 weeks post-injury before significant tissue retraction and scarring occur.

Femoral Avulsions: If the superficial medial collateral ligament is avulsed from the medial epicondyle, the footprint is decorticated to bleeding bone. Suture anchors (typically 4.5 mm to 5.5 mm) are placed at the anatomic origin. Krackow or locking whipstitches are placed through the proximal ligament stump, and the ligament is reduced to its anatomic footprint and tied with the knee held in 20 to 30 degrees of flexion and neutral rotation under slight varus stress.
Tibial Avulsions: Distal avulsions, particularly those retracted superficial to the pes anserinus, are managed similarly. The distal footprint (4 to 6 cm distal to the joint line) is prepared. Suture anchors or a cortical button technique can be utilized to secure the distal stump.
Posterior Oblique Ligament Repair: If the posterior oblique ligament is torn, it must be repaired to restore rotatory stability. Suture anchors are placed at the posteromedial aspect of the medial femoral condyle or the posteromedial tibia depending on the location of the avulsion. The posterior oblique ligament is tensioned and tied with the knee in full extension to eliminate anteromedial rotatory subluxation.

Chronic Reconstruction Techniques
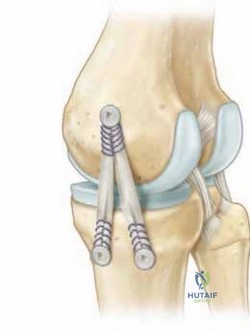
In cases of chronic medial instability or severe acute tissue maceration precluding primary repair, anatomic reconstruction is the gold standard. The anatomic medial knee reconstruction technique, as popularized by LaPrade, utilizes two distinct grafts (often a split Achilles allograft, semitendinosus autograft, or tibialis anterior allograft) to reconstruct both the superficial medial collateral ligament and the posterior oblique ligament.
Femoral Tunnel Preparation: The anatomic origins of the superficial medial collateral ligament and the posterior oblique ligament are identified. The superficial medial collateral ligament origin is slightly proximal and posterior to the medial epicondyle. The posterior oblique ligament origin is located approximately 7.7 millimeters distal and 2.9 millimeters anterior to the gastrocnemius tubercle. Two femoral tunnels are drilled, taking care to angle the pins to avoid intersection with each other or with concurrent cruciate ligament tunnels.
Tibial Tunnel Preparation: Two tibial tunnels are created. The superficial medial collateral ligament tibial tunnel is placed at its anatomic distal insertion, approximately 6 centimeters distal to the joint line. The posterior oblique ligament tibial tunnel is placed at the posteromedial aspect of the tibia, targeting the direct arm attachment of the semimembranosus.

Graft Passage and Fixation: The grafts are secured in the femoral tunnels using interference screws. The superficial medial collateral ligament graft is routed distally, deep to the crural fascia and superficial to the pes anserinus. The posterior oblique ligament graft is routed to the posteromedial tibial tunnel.
Tensioning Protocol: Sequential tensioning is critical for restoring normal knee kinematics. The superficial medial collateral ligament graft is tensioned and fixed in the tibial tunnel with an interference screw or staple while the knee is held in 20 to 30 degrees of flexion under a gentle varus reduction force. Subsequently, the posterior oblique ligament graft is tensioned and fixed with the knee in full extension to restore the posteromedial restraint.

Complications and Management
Surgical intervention on the medial aspect of the knee carries specific risks. The most frequent and debilitating complication following medial collateral ligament repair or reconstruction is postoperative arthrofibrosis. The medial tissues are highly vascular and prone to robust fibrotic responses. This risk is exponentially increased if surgery is performed during the acute inflammatory phase of a combined anterior cruciate ligament and medial collateral ligament injury.

Injury to the saphenous nerve or its infrapatellar branch is another common complication due to the proximity of the surgical approach. This can result in localized neuroma formation, hyperesthesia, or numbness over the anteromedial proximal tibia. Careful blunt dissection and retraction are required to minimize iatrogenic nerve injury.
| Complication | Estimated Incidence | Prevention and Salvage Strategies |
|---|---|---|
| Arthrofibrosis / Loss of Motion | 10% - 15% | Delay concurrent ACL surgery until full ROM is achieved. Early aggressive physical therapy. Salvage: Manipulation under anesthesia, arthroscopic lysis of adhesions. |
| Saphenous Nerve Neuroma | 5% - 10% | Avoid transverse incisions. Careful dissection of Layer I. Salvage: Gabapentinoids, local corticosteroid injections, surgical excision of neuroma. |
| Recurrent Valgus Instability | 3% - 8% | Meticulous anatomic graft placement. Address concurrent cruciate pathology. Evaluate and correct coronal malalignment (HTO). Salvage: Revision reconstruction. |
| Hardware Prominence | 5% - 12% | Countersink interference screws. Use low-profile staples or cortical buttons on the tibia. Salvage: Hardware removal after graft incorporation (>9 months). |
| Deep Vein Thrombosis (DVT) | 1% - 3% | Sequential compression devices, early mobilization, chemical prophylaxis in high-risk patients. Salvage: Therapeutic anticoagulation. |
Hardware prominence over the medial tibial condyle is frequently reported, particularly in asthenic patients, due to the lack of robust soft tissue coverage over the proximal medial tibia. The use of low-profile fixation devices and countersinking interference screws can mitigate this risk.
Post Operative Rehabilitation Protocols
Rehabilitation following medial collateral ligament repair or reconstruction must balance the protection of the healing tissues with the prevention of arthrofibrosis. The protocol is generally divided into distinct phases.

Phase 1: Protection and Early Range of Motion (Weeks 0 to 4)
Postoperatively, the patient is placed in a hinged knee brace locked in extension for weight-bearing. Weight-bearing status typically begins as toe-touch or partial weight-bearing to protect the fixation. Range of motion exercises are initiated immediately to prevent stiffness. The brace is unlocked for passive and active-assisted range of motion from 0 to 90 degrees. Valgus stress must be strictly avoided. Quadriceps activation exercises (isometric sets) and straight leg raises are emphasized.
Phase 2: Progressive Loading and Strengthening (Weeks 4 to 8)
Weight-bearing is progressively advanced to full weight-bearing as tolerated with the brace unlocked. Range of motion is advanced to full, symmetric flexion and extension. Closed kinetic chain exercises (e.g., mini-squats, leg presses) are initiated. Proprioceptive training and stationary cycling begin once 100 degrees of flexion is achieved.
Phase 3: Advanced Strengthening (Weeks 8 to 16)
The hinged knee brace is gradually weaned for activities of daily living. Advanced strengthening focuses on functional movements, eccentric quadriceps and hamstring loading, and core stability. Straight-line jogging and agility drills can be introduced towards the end of this phase, provided the patient demonstrates symmetric lower extremity strength and no valgus laxity on clinical examination.
Phase 4: Return to Sport (Months 4 to 6+)
Return to competitive athletics is contingent upon achieving full, painless range of motion, a stable knee on clinical examination (negative valgus stress test at 0 and 30 degrees), and isokinetic strength testing demonstrating at least 90% symmetry compared to the contralateral uninjured limb. Functional testing, including single-leg hop tests and sport-specific cutting maneuvers, must be passed prior to clearance. A prophylactic functional medial unloader or hinged brace may be utilized during the first season back to play, depending on surgeon preference and sport requirements.
Summary of Key Literature and Guidelines
The evolution of medial knee surgery has been heavily influenced by foundational anatomical and biomechanical studies. The seminal work by Warren and Marshall established the three-layer anatomical model, which remains the fundamental framework for surgical dissection of the medial knee. Hughston's detailed descriptions of the posteromedial corner and the posterior oblique ligament highlighted the necessity of addressing the posterior capsular structures to prevent chronic anteromedial rotatory instability.
More recently, the comprehensive biomechanical and anatomical studies by LaPrade and colleagues have redefined the quantitative anatomy of the medial collateral ligament complex. Their work mapped the precise isometric points for femoral tunnel placement and demonstrated that an anatomic reconstruction utilizing two separate grafts (reconstructing both the superficial medial collateral ligament and the posterior oblique ligament) biomechanically outperforms single-bundle non-anatomic reconstructions in restoring native knee kinematics under valgus and rotatory loads. Current consensus guidelines strongly favor nonoperative management for isolated acute injuries, while advocating for anatomic reconstruction in the setting of chronic instability or severe multi-ligamentous knee trauma.
Clinical & Radiographic Imaging