Masterclass: Single-Bundle Anterior Cruciate Ligament Reconstruction
Key Takeaway
This masterclass guides fellows through single-bundle ACL reconstruction. We meticulously cover surgical anatomy, patient positioning, and real-time intraoperative execution, from graft harvest to tunnel placement and fixation. Emphasis is placed on technique, rationale, and managing potential pitfalls, ensuring a comprehensive understanding of this critical procedure. Prepare to refine your skills and master ACL reconstruction.
Comprehensive Introduction and Patho-Epidemiology
Welcome, esteemed colleagues and fellows, to the operating theater. Today, we undertake a comprehensive exploration of single-bundle anterior cruciate ligament (ACL) reconstruction, an absolute cornerstone procedure in the realm of modern orthopedic sports medicine. Our fundamental surgical objective is to definitively restore both rotational and translational stability to the knee joint, thereby preventing the progressive meniscal deterioration and chondral degradation that invariably accompany chronic, untreated ACL deficiency. This intervention is far more profound than the mere mechanical replacement of a ruptured ligament; it is a meticulously orchestrated restoration of a patient's dynamic joint kinematics, designed to protect their articular health and ensure functional longevity for decades to come.
The epidemiology of ACL injuries reveals a staggering burden on the active population, with hundreds of thousands of reconstructions performed globally each year. These injuries predominantly afflict young, high-demand athletes engaged in pivoting and cutting sports such as soccer, basketball, football, and alpine skiing. The pathogenesis typically involves a non-contact deceleration mechanism, characterized by a sudden change of direction or an awkward landing that imparts a catastrophic combination of valgus stress and internal tibial rotation. This specific vector of force overwhelms the tensile limits of the native ligament, leading to macroscopic failure.
Understanding the cascade of joint degeneration following ACL rupture is critical for the operating surgeon. The ACL-deficient knee is subjected to abnormal anterior tibial translation and pathological rotatory micro-instability. Over time, this altered kinematic environment places immense, unphysiological shear stresses on the secondary stabilizers, most notably the posterior horn of the medial meniscus. The subsequent failure of the medial meniscus removes the primary wedge preventing anterior subluxation, accelerating the onset of early unicompartmental osteoarthritis. Therefore, anatomic reconstruction is not merely a functional upgrade; it is a vital joint-preserving operation.
Detailed Surgical Anatomy and Biomechanics
Ultrastructure and Vascularity
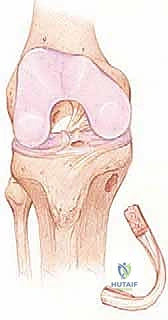
The anterior cruciate ligament is a highly complex, intra-articular, yet extra-synovial stabilizer of the knee joint. Its primary biomechanical function is to serve as the dominant restraint to anterior translation of the tibia relative to the femur, while simultaneously acting as a critical secondary restraint to varus, valgus, and internal/external rotational moments. Anatomically, the native ACL typically measures approximately 33 mm in length and 11 mm in diameter, though these dimensions exhibit natural anthropometric variation. It is a remarkably robust structure, composed predominantly of 90% type I collagen, with the remaining matrix consisting of type III collagen and elastin. This specific collagenous architecture, arranged in a distinct undulating "crimp" pattern, provides the ligament with its exceptional tensile strength and unique viscoelastic properties, allowing it to absorb and dissipate high-energy loads.
The vascular supply and innervation of the ACL are paramount to its biological function and the rationale behind surgical reconstruction. The primary blood supply originates from the middle geniculate artery, which pierces the posterior joint capsule and arborizes within the synovial fold enveloping the ligament. Crucially, the ACL is not merely a passive mechanical tether; it is a highly sophisticated sensory organ. It houses specialized mechanoreceptor nerve endings—specifically Ruffini corpuscles and Pacinian corpuscles—derived from the posterior articular branch of the tibial nerve. These mechanoreceptors are vital for proprioception, contributing significantly to knee joint position sense, dynamic reflex stabilization, and overall neuromuscular control. The loss of this proprioceptive feedback following injury is a major driver of functional instability.
Bundle Anatomy and Osseous Footprints
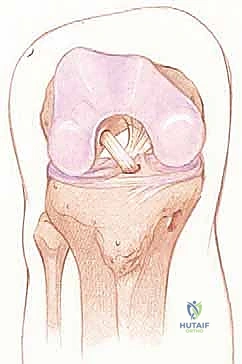
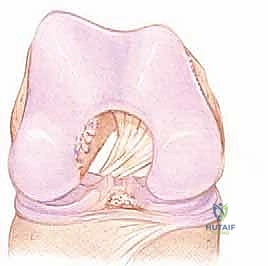
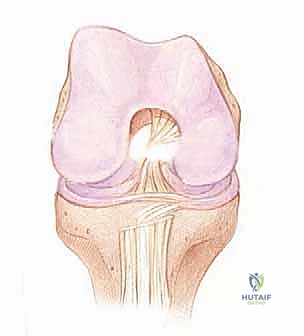
While historically conceptualized and often reconstructed as a single, homogenous ligament, the native ACL is functionally and anatomically organized into two distinct, interdependent bundles, named for their tibial insertion sites: the anteromedial (AM) bundle and the posterolateral (PL) bundle. The AM bundle is primarily tensioned during knee flexion and serves as the primary restraint against anterior tibial translation. Conversely, the PL bundle becomes maximally taut in knee extension and provides the bulk of the resistance against rotatory instability. The complex interplay and reciprocal tensioning of these two bundles throughout the arc of motion are what govern the intricate "screw-home" mechanism and coupled kinematics of the normal knee.
Precise knowledge of the osseous attachment sites is the absolute foundation of anatomic reconstruction. The tibial footprint of the ACL is a broad, irregular diamond-shaped area located immediately anterior and adjacent to the medial tibial eminence, extending anteriorly beneath the transverse intermeniscal ligament. This expansive insertion site allows for a wide distribution of mechanical forces across the plateau. On the femur, the ligament attaches to a semicircular area on the posteromedial aspect of the lateral femoral condyle. Critical osseous landmarks within the intercondylar notch include the lateral intercondylar ridge (often referred to as the resident's ridge), which marks the anterior border of the ACL footprint, and the lateral bifurcate ridge, which separates the AM and PL bundle origins. In a right knee, this footprint typically spans from the 9 o’clock to the 11 o’clock position on an arthroscopic clock face. Failure to respect these precise anatomical boundaries during tunnel preparation inevitably leads to graft impingement, kinematic mismatch, and ultimate clinical failure.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention versus non-operative management requires a nuanced, patient-specific algorithm. While non-operative management—consisting of intensive, phased physical therapy and lifestyle modification—may be appropriate for older, sedentary individuals or those who are true "copers" without subjective instability, surgical reconstruction remains the gold standard for the vast majority of active patients. The primary goal of surgery is to return the patient to their pre-injury level of activity while mitigating the risk of secondary meniscal and chondral damage.
Patient selection must account for physiologic age, baseline activity level, the presence of concomitant intra-articular pathology, and the patient's willingness to adhere to a rigorous postoperative rehabilitation protocol. An isolated ACL tear in a high-level competitive athlete is an almost absolute indication for early reconstruction. Conversely, an ACL tear in a patient with severe, bone-on-bone osteoarthritis may be a contraindication, as restoring stability will not alleviate the primary source of their pain and disability, and may even exacerbate symptoms by altering established, albeit pathological, wear patterns.
| Category | Specific Clinical Scenarios | Rationale and Considerations |
|---|---|---|
| Absolute Indications | Young, high-demand athletes (pivoting/cutting sports). | High risk of recurrent instability and secondary joint damage if left untreated. |
| Absolute Indications | Combined ligamentous injuries (e.g., ACL + PLC, ACL + Grade III MCL). | Multi-ligamentous instability rarely compensates with conservative care; leads to rapid joint destruction. |
| Absolute Indications | ACL rupture with a repairable meniscal tear (e.g., bucket-handle tear). | Meniscal repair has a significantly higher healing rate when performed concurrently with ACL reconstruction due to the hemarthrosis and bone marrow elements introduced during tunnel drilling. |
| Relative Indications | Recurrent subjective instability during activities of daily living (ADLs). | Patient is failing conservative management and experiencing functional impairment. |
| Relative Indications | Pediatric patients with open physes. | Requires specialized physeal-sparing or physeal-respecting techniques to prevent growth arrest, but delaying surgery risks irreparable meniscal damage. |
| Contraindications | Active systemic or local intra-articular infection. | Absolute contraindication; risks catastrophic septic arthritis and graft destruction. |
| Contraindications | Advanced, symptomatic unicompartmental or tricompartmental osteoarthritis. | Reconstructing the ACL will not cure arthritic pain and may alter kinematics unfavorably. High tibial osteotomy (HTO) or arthroplasty may be more appropriate. |
| Contraindications | Voluntary "copers" with low physical demands. | Patients who can dynamically stabilize their knee without functional deficits may avoid the morbidity of surgery. |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Assessment and Imaging
Before the patient ever enters the operating room, a comprehensive, meticulous preoperative workup is essential. The clinical examination must be exhaustive, ruling out concomitant injuries that could compromise the reconstruction if left unaddressed. We must evaluate for medial or lateral joint line tenderness indicative of meniscal pathology. Collateral ligament integrity is assessed with varus and valgus stress testing at 0 and 30 degrees of flexion; significant opening at full extension suggests a complex, multi-ligamentous injury. The posterior cruciate ligament (PCL) must be evaluated via the posterior drawer test and assessment of the tibial step-off to avoid misinterpreting a posterior sag as an anterior drawer (the "pseudo-Lachman"). Furthermore, the posterolateral corner (PLC) must be interrogated using the dial test at 30 and 90 degrees of flexion; unrecognized PLC deficiency is a primary cause of early ACL graft failure due to excessive varus and external rotation forces placed on the new graft.
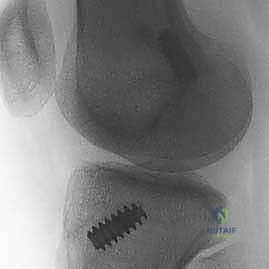
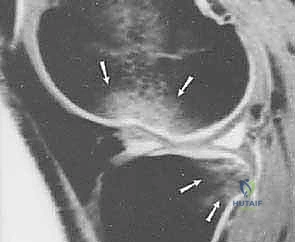
Imaging studies are paramount for preoperative templating and confirming the clinical diagnosis. High-quality, weight-bearing plain radiographs (anteroposterior, lateral, and Merchant/skyline views) are mandatory to rule out bony avulsion fractures (such as the pathognomonic Segond fracture, an avulsion of the anterolateral ligament complex), loose bodies, or pre-existing hardware. In cases of suspected coronal malalignment, long-leg hip-to-ankle radiographs are crucial to assess the mechanical axis. Magnetic Resonance Imaging (MRI) is the gold standard for soft tissue evaluation, offering unparalleled sensitivity and specificity for diagnosing ACL tears, identifying the exact location of the rupture (proximal, mid-substance, or distal), and characterizing associated meniscal tears, chondral lesions, and characteristic bone bruising patterns (typically involving the mid-lateral femoral condyle and posterior lateral tibial plateau).
Examination Under Anesthesia and Patient Positioning
The surgical intervention officially begins with the Examination Under Anesthesia (EUA). This is a non-negotiable, critical step. With the patient fully relaxed and devoid of muscular guarding, we perform a definitive ligamentous examination. The Lachman test is performed to assess anterior tibial translation and endpoint quality. The pivot shift test—the most specific clinical test for rotatory instability—is executed to confirm the functional loss of the ACL. A positive pivot shift, characterized by the subluxation of the lateral tibial plateau in extension and its sudden, clunking reduction in flexion, dictates the necessity of the reconstruction and provides a baseline to which the post-reconstruction stability will be compared.
Patient positioning is meticulously orchestrated to provide optimal, unimpeded access to the knee joint while ensuring patient safety. We position the patient supine on the operating table. A crucial maneuver is dropping the foot of the bed, which allows the operative knee to be flexed freely past 90 degrees and easily brought into full extension. A commercially available, well-padded lateral post or a dedicated knee holder is applied to the proximal thigh of the operative leg. This provides a stable fulcrum against which valgus stress can be applied to open the medial compartment during arthroscopy, while still allowing free manipulation of the limb. The contralateral leg is placed in a well-padded gynecological-style holder or carefully secured to the table and kept entirely out of the operative field to prevent inadvertent neurological injury and maintain strict sterility. A tourniquet is placed high on the operative thigh, though its inflation is strictly at the surgeon's discretion and often reserved only for cases of intractable bleeding to minimize ischemic muscle damage.



Step-by-Step Surgical Approach and Fixation Technique
Graft Selection and Autograft Harvest
The choice of graft material—autograft versus allograft—and the specific autograft type (Bone-Patellar Tendon-Bone [BPTB], Hamstring [semitendinosus/gracilis], or Quadriceps tendon) is a highly individualized decision based on patient age, activity level, occupation, and surgeon expertise. For the young, high-demand athlete, BPTB and Hamstring autografts remain the undisputed gold standards due to their superior biological incorporation and lower failure rates compared to allografts. BPTB is often favored for its rigid bone-to-bone healing and exceptional initial fixation strength, making it ideal for contact athletes. However, it carries a higher risk of anterior knee pain and patellar fracture. Hamstring autografts offer excellent tensile strength with less extensor mechanism morbidity, making them preferable for jumping athletes or those whose occupations require prolonged kneeling.
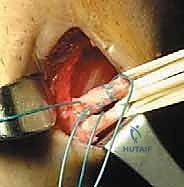
For a BPTB harvest, a 5 to 7-cm paramedian or midline longitudinal incision is made over the patellar tendon. Meticulous dissection is required to identify and protect the infrapatellar branches of the saphenous nerve to prevent postoperative dysesthesia. The paratenon is carefully incised and reflected to be preserved for later closure. Using a double-bladed scalpel, the central third of the patellar tendon (typically 9-10 mm in width) is isolated. Bone plugs, approximately 20-25 mm in length, are harvested from the distal pole of the patella and the tibial tubercle using an oscillating saw and curved osteotomes. The graft is then taken to the back table, where it is meticulously trimmed to pass smoothly through the sizing sizing tubes, and passing sutures are placed through drill holes in the bone plugs.



Diagnostic Arthroscopy and Intercondylar Notch Preparation
Following graft harvest, standard anterolateral (AL) and anteromedial (AM) arthroscopic portals are established. A systematic, comprehensive diagnostic arthroscopy is performed, evaluating the patellofemoral joint, medial and lateral gutters, medial and lateral compartments, and the intercondylar notch. Any concomitant meniscal pathology is addressed at this stage; meniscal repair is always prioritized over resection, especially in the setting of an ACL reconstruction, as the restored stability and the biological milieu of the bleeding bony tunnels significantly enhance meniscal healing rates.
Attention is then directed to the intercondylar notch. The remnants of the ruptured ACL are carefully debrided using a motorized shaver and radiofrequency ablation wand. It is crucial to preserve the tibial stump if it does not impede visualization, as it contains valuable mechanoreceptors and may aid in graft revascularization. A notchplasty—the removal of osteophytes from the lateral wall and roof of the intercondylar notch—may be performed if the notch is inherently narrow (a "stenotic notch") to prevent graft impingement in full extension. However, this must be done conservatively to avoid altering the anatomical landmarks of the femoral footprint, specifically the lateral intercondylar ridge (resident's ridge), which serves as the critical anterior boundary for femoral tunnel placement.




Anatomic Femoral and Tibial Tunnel Preparation
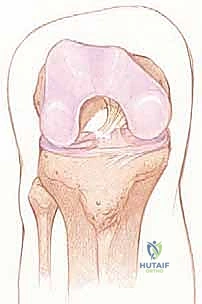
The creation of anatomic osseous tunnels is the most critical technical aspect of the procedure. For the femoral tunnel, independent drilling through an accessory anteromedial (AAM) portal has largely superseded the traditional transtibial technique, as it allows for unconstrained, truly anatomic placement within the native footprint. The knee is hyperflexed (typically >110 degrees) to prevent posterior wall blowout. A specialized femoral offset guide is introduced through the AAM portal and hooked over the over-the-top position. A Beath pin is drilled through the lateral femoral condyle, exiting the anterolateral thigh. The femoral tunnel is then reamed over the pin to the appropriate depth and diameter based on the graft measurements. The tunnel must be positioned posterior to the resident's ridge, typically at the 10 o'clock or 10:30 position for a right knee (or 2 o'clock/1:30 for a left knee), ensuring it captures the center of the native footprint to restore both AM and PL bundle function.




Preparation of the tibial tunnel follows. A tibial drill guide is set to approximately 50-55 degrees to ensure a sufficiently long intraosseous tunnel and to match the native sagittal inclination of the ACL. The intra-articular aiming point is placed at the center of the native tibial footprint, using landmarks such as the posterior border of the anterior horn of the lateral meniscus, the medial tibial spine, and the PCL. The starting point on the anteromedial tibia is typically midway between the tibial tubercle and the posteromedial border of the tibia. A guide pin is advanced, and after arthroscopic confirmation of ideal placement—ensuring no impingement against the PCL or the roof of the notch in full extension—the tunnel is reamed.



Graft Passage, Tensioning, and Fixation
With both tunnels meticulously prepared and cleared of debris, the graft is ready for passage. A passing suture (or a specialized passing loop) is shuttled from the tibial tunnel, through the joint space, and out the femoral tunnel. The graft is then smoothly pulled into position. For a BPTB graft, the bone plugs must dock securely within the osseous tunnels. The orientation of the graft is critical; the collagenous portion should be rotated to mimic the native twist of the ACL bundles.




Robust, rigid fixation is the final, crucial step to allow for early aggressive rehabilitation. For BPTB autografts, aperture fixation using metallic or bioabsor
Clinical & Radiographic Imaging Archive