Comprehensive Introduction and Patho-Epidemiology
The posterior cruciate ligament (PCL) serves as the primary restraint to posterior tibial translation, bearing the immense brunt of posteriorly directed sheer forces across the knee joint throughout the arc of motion. Reconstruction of the PCL remains one of the most formidable surgical challenges in orthopedic sports medicine and traumatology. Historically, surgical interventions for PCL insufficiency were plagued by unacceptable rates of graft attenuation, residual posterior laxity, and early failure. These suboptimal outcomes were largely attributed to the biomechanical flaws inherent in traditional transtibial reconstruction techniques, which forced the graft to negotiate a severely acute angle—the infamous "killer turn"—at the posterior tibial aperture.
The evolution of surgical techniques over the past three decades has led to the popularization and refinement of the tibial inlay technique. By utilizing either autogenous bone-patellar tendon-bone (BTB) or Achilles tendon-bone allografts, the inlay technique directly secures a robust bone block to the posterior tibial cortex. This anatomical restoration entirely eliminates the abrasive shear stresses on the tendinous portion of the graft that defined the transtibial approach. Consequently, the tibial inlay technique provides significantly improved long-term biomechanical stability, restoring native joint kinematics and protecting the medial and patellofemoral compartments from premature degenerative changes.
Understanding the patho-epidemiology of PCL injuries is critical for the operating surgeon. Isolated PCL injuries are relatively uncommon, often resulting from athletic trauma such as a direct blow to the anterior tibia with the knee flexed, or hyperflexion injuries with a plantarflexed foot. However, the majority of high-grade PCL ruptures occur in the setting of high-energy trauma, such as motor vehicle collisions resulting in the classic "dashboard injury." In these scenarios, the PCL is frequently injured in conjunction with the posterolateral corner (PLC), anterior cruciate ligament (ACL), or medial collateral ligament (MCL), constituting a complex multi-ligament knee injury (MLKI).
Chronic, untreated PCL deficiency inevitably alters the contact mechanics of the knee. The posterior sag of the tibia relative to the femur dramatically increases contact pressures in the medial femorotibial compartment and the patellofemoral joint. Over time, this aberrant kinematic profile leads to rapidly progressive articular cartilage degeneration and meniscal tearing. Therefore, mastering the tibial inlay reconstruction is not merely an exercise in restoring ligamentous continuity; it is a vital joint-preserving intervention designed to halt the progression of post-traumatic osteoarthritis in the young, active patient population.
Detailed Surgical Anatomy and Biomechanics
Osteology and Ligamentous Footprints
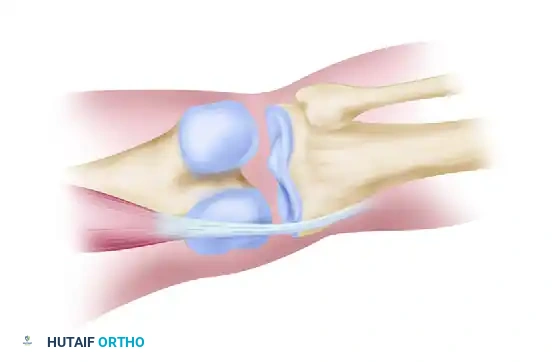
A profound mastery of the native PCL anatomy is non-negotiable for successful reconstruction. The PCL is an intra-articular, extrasynovial structure, significantly thicker and stronger than the ACL. It originates from a broad, crescent-shaped footprint on the anterolateral aspect of the medial femoral condyle. This femoral attachment is expansive, extending from the articular margin proximally and posteriorly. The tibial insertion is located in a central depression on the posterior aspect of the tibia, known as the PCL facet. This insertion site extends distally along the posterior tibial cortex, blending with the periosteum approximately 1 to 1.5 centimeters distal to the posterior articular surface.
The PCL is functionally divided into two distinct bundles: the larger anterolateral (AL) bundle and the smaller posteromedial (PM) bundle. These bundles exhibit a reciprocal tensioning pattern throughout the knee's range of motion. The AL bundle is tightest in knee flexion (particularly between 70 and 90 degrees), serving as the primary restraint to posterior translation in the flexed position. Conversely, the PM bundle becomes taut in full extension and hyperextension. Single-bundle reconstructions, such as the standard tibial inlay technique, primarily aim to recreate the biomechanical function of the dominant AL bundle, targeting its isometric center on the medial femoral condyle.
Intimately associated with the PCL are the meniscofemoral ligaments (MFLs) of Humphry (anterior to the PCL) and Wrisberg (posterior to the PCL). These ligaments originate from the posterior horn of the lateral meniscus and insert onto the medial femoral condyle adjacent to the PCL footprint. The MFLs are present in up to 90% of knees and contribute significantly to posterior stability, particularly when the PCL is deficient. During a posterior approach for a tibial inlay, the surgeon must carefully assess these structures; if the native PCL is avulsed but the MFLs remain intact, they should be preserved to augment the reconstructed construct.
Posterior Neurovascular Anatomy
The posterior approach to the knee requires meticulous navigation of a dense and highly unforgiving neurovascular landscape. The popliteal fossa is bounded superolaterally by the biceps femoris, superomedially by the semimembranosus and semitendinosus, and inferiorly by the medial and lateral heads of the gastrocnemius. Deep within this rhomboid space lies the popliteal neurovascular bundle. The tibial nerve is the most superficial structure within the bundle, crossing from lateral to medial as it descends. It gives off critical motor branches to the gastrocnemius, soleus, and plantaris muscles, which must be identified and protected during medial gastrocnemius retraction.
Deep and slightly medial to the tibial nerve is the popliteal vein, and deepest still, lying directly against the posterior joint capsule, is the popliteal artery. The proximity of the popliteal artery to the posterior capsule makes it highly vulnerable during blind transtibial drilling or aggressive posterior capsular dissection. The medial inferior genicular artery and vein course transversely across the superior margin of the popliteus muscle and the posterior capsule. These vessels are routinely encountered during the arthrotomy for the tibial inlay and must be meticulously ligated to prevent catastrophic postoperative hematoma and subsequent posterior compartment syndrome.
The sural nerve, a sensory branch formed by contributions from the tibial and common peroneal nerves, descends vertically between the two heads of the gastrocnemius in the subcutaneous tissue. The initial vertical incision for the posterior approach places this nerve at immediate risk. The surgeon must carefully divide the deep fascia and identify the sural nerve, retracting it laterally with the lesser saphenous vein to ensure its protection throughout the procedure. Iatrogenic injury to the sural nerve results in painful neuromas and distressing sensory deficits along the posterolateral calf and lateral foot.
Exhaustive Indications and Contraindications
Patient Selection and Clinical Decision Making
The decision to proceed with operative reconstruction of the PCL is highly nuanced, relying on a combination of clinical laxity, chronicity of the injury, concomitant ligamentous damage, and the patient's functional demands. Isolated Grade I (0-5 mm of posterior translation) and Grade II (6-10 mm of posterior translation) PCL injuries are generally managed non-operatively with a high degree of success, utilizing specialized dynamic bracing and aggressive quadriceps rehabilitation. The robust intrinsic healing capacity of the PCL often allows for functional stability in these lower-grade isolated injuries.
However, operative intervention is strictly indicated for acute isolated Grade III injuries (>10 mm of posterior translation, where the anterior tibia falls posterior to the medial femoral condyle), particularly in young, high-demand athletes. Furthermore, any PCL injury occurring in the context of a multi-ligament knee injury (e.g., PCL + ACL, or PCL + PLC) necessitates surgical reconstruction. In these complex scenarios, failure to address the PCL will inevitably lead to the failure of the reconstructed concomitant ligaments due to uncoupled rotational and translational forces. Chronic symptomatic PCL deficiency, characterized by recurrent instability, pain, and early medial compartment or patellofemoral arthrosis, is also a definitive indication for the tibial inlay procedure.
Contraindications to the tibial inlay procedure must be strictly respected to avoid devastating complications. Active local or systemic infection is an absolute contraindication. Severe, end-stage tricompartmental osteoarthritis represents a relative contraindication, as ligamentous reconstruction will not alleviate arthritic pain; such patients are better served by arthroplasty or corrective osteotomy. Additionally, poor soft tissue envelopes, severe peripheral vascular disease, and patient non-compliance with the rigorous postoperative rehabilitation protocol are significant deterrents to surgical intervention.
Indications and Contraindications Matrix
| Category | Specific Criteria | Rationale / Clinical Context |
|---|---|---|
| Absolute Indications | Multi-Ligament Knee Injury (MLKI) | PCL deficiency guarantees failure of concomitant ACL/PLC/MCL reconstructions. |
| Absolute Indications | Bony Avulsion Fractures | Displaced tibial sided avulsions require internal fixation (equivalent to inlay). |
| Relative Indications | Acute Isolated Grade III Laxity | >10mm posterior translation in high-demand athletes prevents future arthrosis. |
| Relative Indications | Chronic Symptomatic Deficiency | Pain and instability failing conservative management; prevents medial/PF OA. |
| Absolute Contraindications | Active Joint Infection | High risk of septic arthritis and catastrophic graft failure. |
| Absolute Contraindications | End-Stage Osteoarthritis | Ligament reconstruction will not resolve bone-on-bone arthritic pain. |
| Relative Contraindications | Vascular Compromise | Popliteal approach risks further ischemic injury in compromised limbs. |
| Relative Contraindications | Patient Non-Compliance | Inability to adhere to strict bracing and rehab leads to graft attenuation. |
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging and Radiographic Sizing Protocol
Precise preoperative templating is the absolute cornerstone of a successful PCL reconstruction utilizing the tibial inlay technique. The surgeon must meticulously calculate the required graft length to prevent the bony portion of the tendon graft from recessing too proximally within the femoral tunnel. A recessed graft subjects the tendinous portion to abrasive attenuation against the tunnel aperture, recreating the very problem the inlay technique was designed to solve. Comprehensive imaging begins with weight-bearing anteroposterior, lateral, and Rosenberg views to assess joint space narrowing, alongside stress radiography (e.g., Telos device) to objectively quantify posterior translation.
High-resolution Magnetic Resonance Imaging (MRI) is mandatory to evaluate the integrity of the PCL bundles, the menisci, the chondral surfaces, and the posterolateral corner structures. However, for precise graft sizing, a strictly calibrated, true lateral radiograph of the knee flexed to exactly 30 degrees is required. The surgeon must ensure there is 3 mm or less of posterior femoral condylar overlap to guarantee a true orthogonal projection. Utilizing a high-intensity illuminator or digital templating software, the exact tibial tuberosity insertion site of the patellar tendon is identified, located just anterior to the infrapatellar fat pad density.
The native PCL trajectory is then mapped. The PCL's biomechanical strength is optimized when reconstructed from the anterior margin of the intercondylar line to a precise point 1 cm below the posterior articular surface of the tibia. The anticipated intra-articular length of the reconstructed PCL is measured. The surgeon must compare the measured PCL length to the anticipated length of the patient's autogenous patellar tendon. If the autogenous tendon exceeds the measured PCL length by more than 1.5 cm, the graft will "bottom out" or recess excessively. In such instances, the surgeon must abandon the autograft and utilize an Achilles tendon-bone allograft or a pre-measured BTB allograft of specified tendinous length.
The Berg Dual-Phase Positioning Strategy
The tibial inlay technique, as popularized by Berg, requires a highly orchestrated, dual-phase positioning strategy. This complex setup allows for a seamless transition between the anterior arthroscopic phase and the posterior open popliteal phase without compromising sterility or requiring complete, time-consuming re-draping. General anesthesia with profound muscle relaxation is mandatory to facilitate joint manipulation and posterior retraction. A high-thigh tourniquet is applied but ideally inflated only during the posterior open phase to minimize ischemic time.
Phase 1: Anterior and Arthroscopic Access
The patient is initially placed in the lateral decubitus position with the operative leg suspended upward. The limb is circumferentially prepared and draped from the proximal thigh to the midcalf using sterile impervious stockinettes and split drapes. The hip is abducted and externally rotated to 45 degrees, and the knee is flexed to 90 degrees. In this configuration, the anterior aspect of the knee directly faces the operating surgeon, facilitating highly ergonomic access for BTB graft harvest, diagnostic arthroscopy, and femoral tunnel preparation.

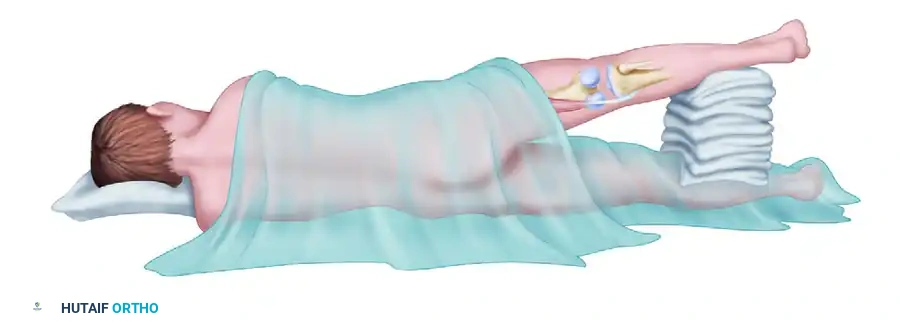
Phase 2: Posterior Popliteal Access
Following the completion of the anterior phase, the patient's position is dynamically modified by the surgical team. The knee is extended, and the operating table is tilted anteriorly toward the prone position. The thigh is abducted, and the extremity is supported with stacked sterile towels or a sterile foam ramp. This critical maneuver opens the popliteal fossa, providing the necessary direct trajectory for the posterior approach while rigorously maintaining the sterile field. The surgeon then moves to the posterior aspect of the limb to execute the inlay.
Step-by-Step Surgical Approach and Fixation Technique
1. Graft Harvest and Preparation
The procedure commences with the harvest of a 10-mm-wide central-third bone-patellar tendon-bone (BTB) autograft, assuming preoperative templating confirmed appropriate tendinous length. The graft is extracted utilizing standard trapezoidal bone blocks from the patella and tibial tubercle, typically measuring 20-25 mm in length. Meticulous care is taken not to violate the articular surface of the patella. Once harvested, the graft is taken to the back table for immediate preparation.
The tibial tubercle bone block (which will become the tibial inlay) is drilled and tapped to accept a 6.5-mm cancellous titanium screw and a spiked washer. This preparation is critical, as attempting to drill the block deep within the popliteal fossa later is technically demanding and risks fracturing the bone block. Heavy, non-absorbable traction sutures (e.g., #5 FiberWire) are passed through drill holes in the patellar bone block (which will reside in the femur) to facilitate retrograde passage through the joint. If an Achilles allograft is utilized, the calcaneal bone block is similarly shaped and pre-drilled for the inlay screw, while the tendinous portion is tubularized with a running locking stitch.
2. Diagnostic Arthroscopy and Concurrent Procedures
Standard anterolateral and anteromedial arthroscopic portals are established. Alternatively, the surgeon may utilize the incision created through the patellar tendon defect and fat pad, or a medial parapatellar arthrotomy, to thoroughly examine the intra-articular structures. A systematic diagnostic arthroscopy is performed to address any concurrent meniscal or chondral pathology before proceeding with the ligamentous reconstruction. The native PCL remnants are debrided using an aggressive shaver and radiofrequency ablation, taking care to preserve the meniscofemoral ligaments if they remain competent.
A critical clinical pearl must be observed: if a combined arthroscopic anterior cruciate ligament (ACL) and open PCL reconstruction is planned, the surgeon must always perform the ACL reconstruction first. The subsequent popliteal arthrotomy required for the PCL inlay will completely compromise the posterior joint capsule. If arthroscopy under fluid pressure is attempted after the posterior capsulotomy, it will lead to massive, uncontrollable extravasation of arthroscopic irrigation fluid into the posterior calf compartments, risking acute compartment syndrome.
3. Femoral Tunnel Preparation
The femoral origin of the PCL is broad, but the isometric center of the anterolateral bundle is the primary target for a single-bundle reconstruction. A femoral aiming jig is introduced through the anteromedial portal. The guide pin is positioned in the anterosuperior femoral origin of the PCL, precisely 4 to 5 mm from the anterior articular margin of the medial femoral condyle, at the 1 o'clock (left knee) or 11 o'clock (right knee) position.
An outside-in or inside-out technique may be utilized. For the outside-in approach, a 5-cm longitudinal incision is made proximal to the medial femoral epicondyle. The medial patellar retinaculum is divided, and the medial femoral condyle is exposed subperiosteally. The guide pin is over-drilled using a cannulated reamer matched to the exact diameter of the patellar bone block (typically 10 or 11 mm) to create the interosseous tunnel. The intra-articular margins of this femoral tunnel must be meticulously chamfered with a rasp to prevent a guillotine-effect abrasion on the graft during repetitive flexion. Finally, an 18-gauge wire loop or specialized suture passing device is passed through the femoral tunnel into the posterior joint space for later graft shuttling.
4. The Posterior Approach to the Popliteal Fossa
The patient is transitioned to the modified prone position (Phase 2). A vertical incision is made in line with the palpable semitendinosus tendon. As the incision reaches the popliteal crease, it is veered laterally and extended distally over the posterior calf, creating a gentle "S" shape to prevent scar contracture. The deep fascia overlying the gastrocnemius muscle is exposed and incised vertically. The sural nerve is immediately identified, mobilized, and gently retracted laterally.
The surgeon bluntly develops the interval between the medial head of the gastrocnemius and the semimembranosus tendon. Slightly flexing the knee at this stage significantly improves deep exposure and relieves dangerous tension on the popliteal vessels. The medial head of the gastrocnemius is incised near its tendinous insertion and retracted laterally, strictly protecting its motor branch from the tibial nerve. The inferior medial geniculate artery and vein are identified overlying the posterior capsule, ligated, and divided. A vertical incision is then made through the oblique popliteal ligament and the posterior joint capsule to enter the joint. The posterior tibial plateau is exposed subperiosteally, preparing the bony bed for the inlay.
5. Graft Passage, Tibial Inlay, and Fixation
The 18-gauge wire loop previously placed through the femoral tunnel is retrieved through the posterior arthrotomy. The traction sutures of the patellar bone block are passed through the loop, and the graft is advanced retrograde into the medial femoral condyle tunnel. The graft is secured within the femoral tunnel using a 7-mm or 9-mm diameter cannulated titanium or biocomposite interference screw. The bony portion of the graft must lie flush at the tunnel margin interface, avoiding deep recession.
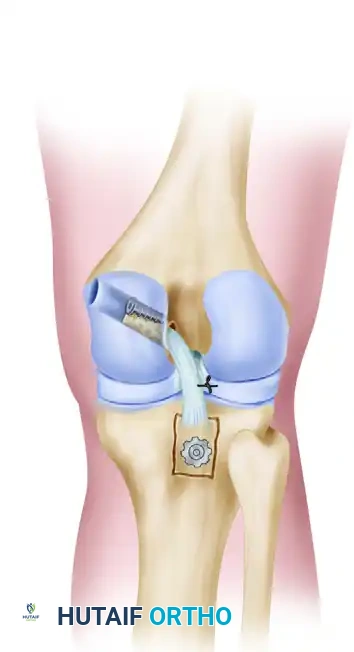
The knee is then positioned in full extension. This utilizes the geometric congruity of the femoral condyles and the tibial plateau to automatically reduce posterior tibial subluxation. Slight manual tension is applied to the tendinous portion of the graft to determine the exact site for posterior tibial fixation. Using a sharp osteotome or a high-speed burr, a precise unicortical window is created in the posterior tibia, 1 cm distal to the articular surface. The dimensions of this window must perfectly match the size of the tibial bone block.
The bone block is inlaid into the prepared tibial window and secured rigidly to the underlying cancellous bone using the pre-selected 6.5-mm titanium cancellous screw and spiked washer. If the graft is marginally too long, the tibial insertion site is advanced further distally along the posterior tibial cortex before creating the window. Following fixation, the posterior compartment is thoroughly irrigated. The medial head of the gastrocnemius is repaired to its insertion site, and the wound is closed in a routine, layered fashion.
Complications, Incidence Rates, and Salvage Management
Intraoperative and Postoperative Risks
While the tibial inlay technique provides superior biomechanical outcomes, it is a technically demanding procedure associated with severe potential complications. Neurovascular injury is the most feared complication. The popliteal artery is at risk during posterior capsular dissection and retractor placement. Incidence of major vascular injury is rare (<1%), but requires immediate vascular surgery consultation, intraoperative angiogram, and potential bypass grafting. Tibial nerve neuropraxia can occur from aggressive lateral retraction of the medial gastrocnemius; this is typically transient, resolving over 3-6 months, but requires careful postoperative neurological monitoring.
Arthrofibrosis and loss of flexion are common postoperative complications, occurring in up to 10-15% of patients. This is often driven by prolonged immobilization or excessive initial tensioning of the graft. Management involves aggressive physical therapy, dynamic splinting, and, if refractory, arthroscopic lysis of adhesions and manipulation under anesthesia (MUA) at the 3-to-6-month mark. Residual posterior laxity or graft failure can occur due to unrecognized posterolateral corner (PLC) injuries, poor graft incorporation, or premature return to high-impact activities.
Posterior compartment syndrome of the calf is a rare but catastrophic complication unique to procedures involving posterior capsulotomies combined with arthroscopy. If fluid extravasates into the posterior compartments, tissue pressures can rapidly exceed capillary perfusion pressure, leading to muscle necrosis. Immediate recognition—characterized by a tense, non-compressible calf and out-of-proportion pain—mandates emergent four-compartment fasciotomy.
Complications and Salvage Strategies Matrix
| Complication | Estimated Incidence | Mechanism/Etiology | Salvage / Management Strategy |
|---|---|---|---|
| Popliteal Artery Injury | < 1% | Aggressive posterior retraction; aberrant vessel anatomy. | Emergent vascular consult; primary repair or saphenous vein bypass. |
| Arthrofibrosis | 10 - 15% | Prolonged immobilization; capsular scarring; over-tensioning. | Aggressive PT; dynamic bracing; Arthroscopic lysis of adhesions + MUA. |
| Graft Attenuation / Failure | 5 - 10% | Unrecognized PLC injury; premature weight-bearing; biological failure. | Revision reconstruction (often requiring allograft); concurrent PLC repair. |
| Sural Nerve Neuroma | 2 - 5% | Iatrogenic transection or entrapment during posterior approach. | Gabapentinoids; local corticosteroid injections; surgical neuroma excision. |
| Posterior Compartment Syndrome | < 1% | Massive fluid extravasation during concurrent arthroscopy. | Emergent four-compartment lower extremity fasciotomy. |
Phased Post-Operative Rehabilitation Protocols
Phase I: Maximum Protection (Weeks 0–2)
Rehabilitation following a tibial inlay PCL reconstruction is inherently conservative, designed to rigidly protect the healing graft from posterior shear forces while safely initiating the restoration of functional range of motion. During the first two weeks, the knee is locked in a hinged knee brace in full extension (0 degrees) at all times, including during sleep. This extended position utilizes the bony congruity of the joint to prevent posterior tibial sag, entirely offloading the newly reconstructed PCL.
Weight-bearing protocols vary slightly among surgeons, but partial weight-bearing (typically 25-50%) with bilateral axillary crutches is generally permitted immediately. This controlled axial loading stimulates joint proprioception and promotes the flow of synovial fluid for cartilage nutrition without overloading the ligamentous construct. Therapeutic exercises in this phase are strictly limited to elevation, cryotherapy, and active ankle pumps to mitigate edema and prevent deep vein thrombosis. Passive patellar mobilization is initiated to prevent infrapatellar contracture.
Phase II: Controlled Mobilization (Weeks 2–6)
At the two-week mark, provided the wound is healing well and the patient demonstrates adequate quadriceps control (ability to perform a straight leg raise without an extensor lag), progression to full weight-bearing in the locked brace is allowed. The brace is sequentially unlocked during supervised physical therapy sessions to permit a protected, passive arc of motion from 0 to 90 degrees. Flexion beyond 90 degrees is strictly prohibited during this phase, as the anterolateral bundle of the PCL experiences maximum tension in deep flexion.
Strengthening begins with a relentless focus on the quadriceps mechanism. Isometric quadriceps exercises (quad sets, straight leg raises) are initiated. Crucially, active knee extension exercises should be performed with the knee positioned between 70 and 90 degrees of flexion; this specific arc minimizes posterior tibial translation forces, as the patellar tendon angle draws the tibia anteriorly. Active hamstring contraction is strictly and absolutely avoided. The hamstrings act as direct antagonists to the PCL, drawing the tibia posteriorly; premature hamstring activation is a primary driver of graft attenuation.
Phase III and IV: Advanced Strengthening and Return to Play (Weeks 6+)
By week six, the patient is typically weaned off crutches, and the brace is transitioned to a dynamic PCL brace (e.g., Jack PCL brace) which applies an anteriorly directed force to the posterior calf. Progression to a full, unrestricted arc of motion is encouraged. Prone quadriceps exercises are advanced, and closed-kinetic-chain exercises such as mini-squats and leg presses (limited to 0-70 degrees) are introduced.
Light, closed-kinetic-chain hamstring exercises may be cautiously introduced around week 12, progressing to full arc hamstring strengthening only as graft incorporation solidifies (typically visible on MRI by 6 months). Return to cutting, pivoting, and contact sports is a prolonged process, generally delayed until 9 to 12 months postoperatively. Clearance for return to play is strictly contingent upon the restoration of at least 90% contralateral quadriceps and hamstring strength on isokinetic testing, complete resolution of effusions, and the absolute absence of posterior instability on clinical examination (negative posterior drawer and dial tests).
Summary of Landmark Literature and Clinical Guidelines
The paradigm shift from transtibial to tibial inlay PCL reconstruction is strongly supported by decades of rigorous biomechanical and clinical research. The foundational work by Berg (1995) originally detailed the dual-positioning inlay technique, demonstrating that direct posterior fixation eliminated the "killer turn" and provided superior graft isometry. Biomechanical cadaveric studies by Markolf et al. provided the definitive quantitative evidence for this shift. Markolf demonstrated that transtibial grafts experienced significantly higher cyclic elongation and ultimate failure rates due to the acute angle at the posterior tibial aperture, whereas the inlay technique restored posterior laxity to within 1-2 mm of the intact native state.
Clinical outcomes literature further corroborates these biomechanical findings. Long-term cohort studies comparing BTB autografts to Achilles allografts in the inlay position have shown equivalent stability, but Achilles allografts are frequently preferred in complex reconstructions or smaller patients to avoid the morbidity of a massive autograft harvest and the risk of graft-tunnel mismatch ("bottoming out"). Furthermore, literature emphasizes that addressing concomitant posterolateral corner (PLC) injuries is paramount; failure to reconstruct an incompetent PLC results in a 30-40% increase in forces seen by the PCL graft, guaranteeing eventual failure.
Current clinical guidelines from the American Academy of Orthopaedic Surgeons (AAOS) and the American Orthopaedic Society for Sports Medicine (AOSSM) advocate for the tibial inlay technique in high-demand patients with Grade III acute injuries, chronic symptomatic laxity, and multi-ligament knee injuries, provided the surgeon possesses the requisite anatomical expertise to safely navigate the popliteal fossa.
