PCL Reconstruction: Treating Posterior Cruciate Ligament Avulsion
Key Takeaway
Discover the latest medical recommendations for PCL Reconstruction: Treating Posterior Cruciate Ligament Avulsion. A posterior cruciate ligament (PCL) injury can involve an avulsion, meaning a bone fragment detaches where the PCL inserts. Treatment often involves surgical reattachment via an open procedure. The posterior approach to the knee is commonly used for PCL avulsion repair, popliteal cyst removal, posterior tibial plateau fractures, and certain posterior cruciate ligament (PCL) reconstructions.
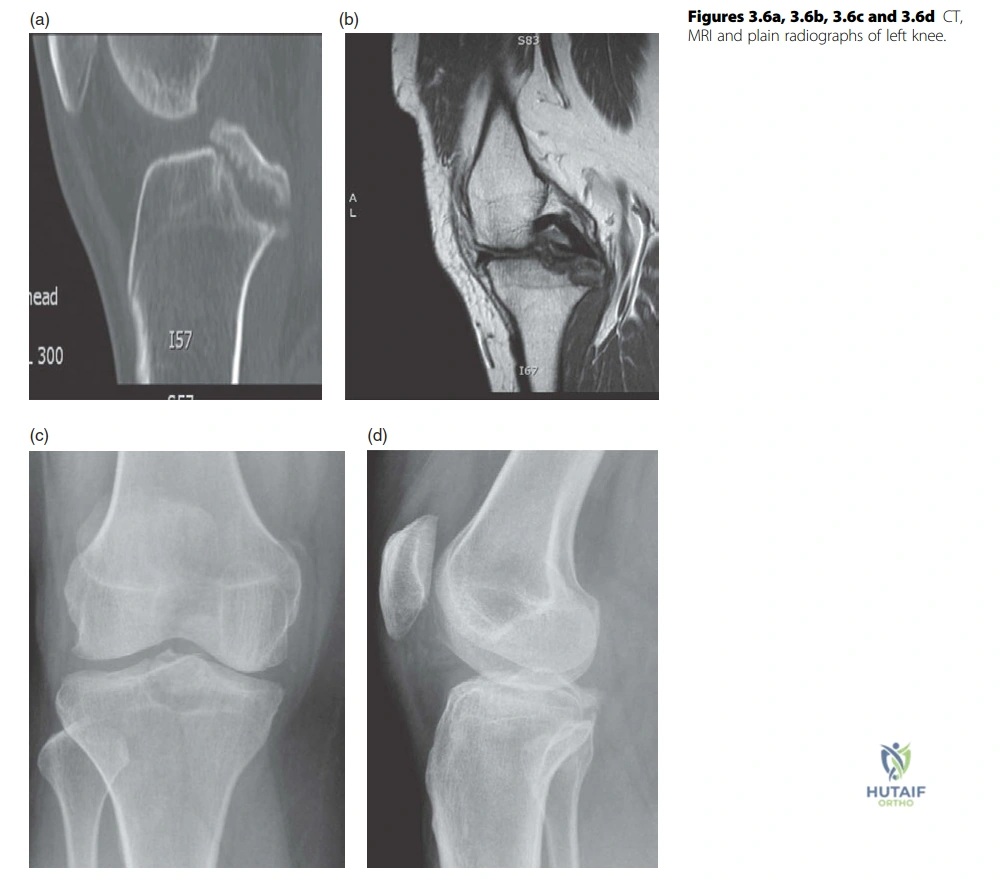
A 26-year-old rugby player presents following an awkward fall on the left knee. These are the presenting radiographs. What do you see and how would you manage this?
Candidate: I see a large bony avulsion fracture at the posterior aspect of the proximal tibia, consistent with a PCL avulsion injury. The lateral film shows the fragment is displaced into the joint. I would manage this with open reduction and internal fixation to restore the footprint, typically via a posterior approach.
Failing to identify the displacement of the fragment or jumping immediately to "reconstruct the PCL." In an avulsion, the primary goal is ORIF of the bony fragment rather than a ligament reconstruction, as the ligamentous tissue is still attached to the bone.
Systematically describe the injury: Location (posterior tibia), nature (bony avulsion of the PCL), and stability/displacement (displaced fragment within the joint). Acknowledge that the patient requires surgical fixation to prevent long-term laxity and arthritis, justifying ORIF over conservative management due to the size and displacement of the fragment.
You mentioned a posterior approach. Describe the surgical anatomy and the structures at risk during this approach.
Candidate: The posterior approach is typically done prone. Structures at risk include the popliteal artery, popliteal vein, tibial nerve, and common peroneal nerve. The gastrocnemius heads need to be mobilized to expose the posterior capsule.
Forgetting to mention the specific nerves (Sural/Tibial/Peroneal) or failing to discuss the necessity of ligating the middle geniculate vessels to safely mobilize the neurovascular bundle.
Structure the answer by layers: Skin incision (Lazy S), dissection (identifying the Sural nerve and avoiding the Common Peroneal nerve), and deep exposure (retracting the Popliteal neurovascular bundle after ligating the middle/superior medial geniculate vessels). Crucially, emphasize that the popliteal artery is the most vulnerable structure because it is deep to the vein and nerve and lies directly against the posterior capsule.
Moving to ACL reconstruction: What are the principles of tunnel placement and what happens if you place the femoral tunnel too anteriorly?
Candidate: Tunnels should be placed at the anatomic footprint. If the femoral tunnel is too anterior, it causes graft impingement in flexion, limits the range of motion, and can lead to graft elongation or failure.
Confusing anterior/posterior errors. An anterior tunnel restricts flexion, while a posterior tunnel results in a vertical graft that fails to control rotational stability (pivot shift) and can blow out the posterior wall of the femur.
Clearly distinguish between 'isometric' vs 'anatomic' placement. Define the 'Resident's Ridge' as a landmark. Explain the biomechanical consequence: Anterior placement = flexion impingement; Posterior/Vertical placement = poor rotational control and posterior wall blowout. Mention the necessity of notchplasty if the tunnel placement risks impingement.
