Comprehensive Introduction and Patho-Epidemiology
Historical Context and Evolution of Techniques
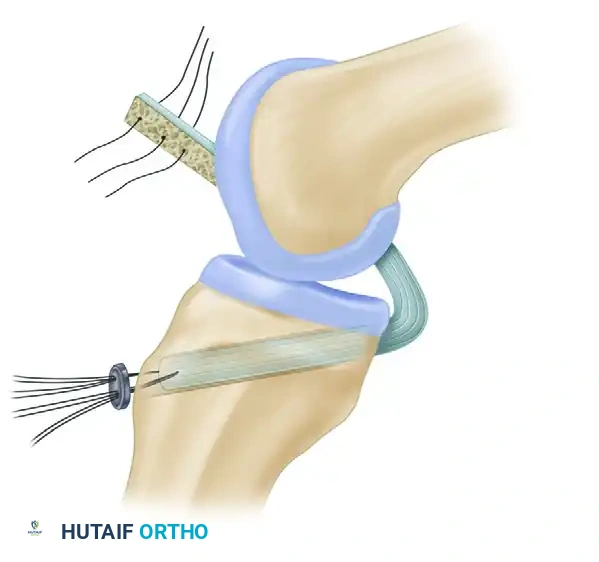
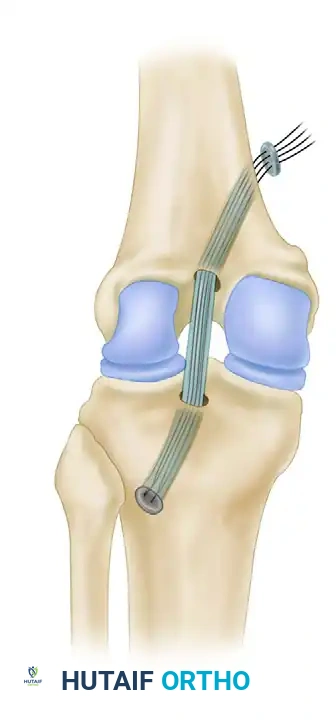
Reconstruction of the posterior cruciate ligament (PCL) represents one of the most formidable challenges in operative sports medicine and orthopedic traumatology. Historically, the PCL was often referred to as the "forgotten ligament," with early 20th-century literature suggesting that non-operative management was universally sufficient due to the inherent bony stability of the medial and lateral compartments. However, longitudinal studies eventually demonstrated that chronic PCL deficiency inexorably leads to altered knee kinematics, elevated contact pressures in the patellofemoral and medial compartments, and early-onset degenerative joint disease. The paradigm shifted dramatically in 1983 when Clancy introduced the concept of anatomical PCL reconstruction utilizing a bone-patellar tendon-bone (BTB) autograft. This technique established the foundation for modern PCL surgery by emphasizing the necessity of rigid bone-to-bone healing and precise anatomical footprint restoration.
The evolution of PCL reconstruction has been defined by a continuous quest to replicate the ligament's complex biomechanical properties while minimizing surgical morbidity. Early open procedures were fraught with extensive soft tissue dissection and a high risk of arthrofibrosis. The advent of arthroscopically assisted techniques significantly reduced surgical trauma, yet the fundamental principles established by Clancy remain highly relevant. The BTB autograft is particularly esteemed in this context because the osseous integration of the patellar and tibial bone plugs within the femoral and tibial tunnels, respectively, provides unparalleled initial fixation strength. This is critically important given the massive posterior shear forces the graft must withstand during early rehabilitation and subsequent return to weight-bearing activities.
Despite these advancements, PCL reconstruction continues to present unique intraoperative hurdles that are distinctly more complex than those encountered in anterior cruciate ligament (ACL) reconstruction. The anatomical location of the PCL's tibial insertion—situated on the posterior facet of the tibia, immediately anterior to the popliteal neurovascular bundle—demands an exacting and perilous surgical approach. Furthermore, the biomechanical phenomenon known as the "killer turn," which describes the acute angle the graft must navigate as it exits the posterior tibial aperture and courses anteriorly toward the medial femoral condyle, remains a primary cause of graft attenuation and failure. Consequently, mastering this procedure requires an exhaustive understanding of both spatial anatomy and kinematic principles.
Pathophysiology and Injury Mechanisms
The pathophysiology of PCL injuries is intrinsically linked to the ligament's role as the primary restraint to posterior tibial translation, providing approximately 95% of the total resisting force at 90 degrees of knee flexion. The most common mechanism of injury is a direct, high-energy posterior blow to the proximal tibia with the knee in a flexed position, classically described as the "dashboard injury" in motor vehicle collisions. In athletic populations, a similar mechanism occurs during a forceful fall onto a flexed knee with the foot in plantarflexion, driving the tibial tubercle posteriorly relative to the distal femur. Alternatively, severe hyperflexion or hyperextension injuries, often accompanied by varus or valgus moments, can result in combined multiligamentous trauma involving the PCL, the posterolateral corner (PLC), or the medial collateral ligament (MCL) complex.
When the PCL ruptures, the instantaneous center of rotation of the knee shifts, profoundly altering the kinematic envelope of the joint. In a PCL-deficient knee, the tibia rests in a posteriorly subluxated position. During the initiation of knee flexion, the quadriceps mechanism must first pull the tibia anteriorly to reduce the joint before true extension can occur, a phenomenon clinically observed as the "quadriceps active test." This persistent posterior subluxation dramatically increases the sheer stress on the articular cartilage of the medial femoral condyle and the patellofemoral joint. Over time, this abnormal load distribution leads to the degradation of the chondral matrix, subchondral sclerosis, and the eventual development of severe, symptomatic osteoarthritis, particularly in the medial and patellofemoral compartments.
Understanding the chronicity of the injury is paramount for the operating surgeon. In acute settings (less than three weeks post-injury), the tissue planes are often obscured by hematoma and edema, but the native ligament remnants can frequently be identified and utilized as anatomical landmarks for tunnel placement. In chronic settings, the ligament remnants typically resorb or scar to the anterior cruciate ligament or the posterior capsule. Furthermore, chronic posterior tibial sag leads to secondary contractures of the posterior capsule and adaptive shortening of the hamstring musculature. These secondary soft-tissue changes must be meticulously addressed during surgical reconstruction to ensure that the tibia can be fully reduced to its anatomical neutral position prior to graft tensioning and fixation.
Epidemiological Considerations
Epidemiologically, PCL tears account for approximately 3% to 20% of all knee ligament injuries, a wide variance that reflects the high rate of missed diagnoses in acute clinical settings. Unlike ACL tears, which frequently present with a dramatic history of a "pop," immediate hemarthrosis, and profound instability, isolated PCL injuries can be remarkably insidious. Patients may present with vague posterior knee pain, mild effusion, and a feeling of deceleration instability rather than frank giving-way episodes. Consequently, many isolated Grade I and Grade II PCL injuries go undiagnosed and are managed conservatively, often with acceptable short-to-medium-term functional outcomes but insidious long-term joint degradation.
High-velocity trauma remains the most frequent etiology for severe Grade III isolated tears and multiligamentous knee injuries involving the PCL. In urban trauma centers, motor vehicle accidents and motorcycle collisions constitute the vast majority of these cases. In these high-energy scenarios, the incidence of concomitant injuries to the posterolateral corner, the medial collateral ligament, or the popliteal neurovascular bundle is exceptionally high. The presence of a multiligamentous injury exponentially complicates the surgical decision-making process, as failure to address peripheral instability (e.g., an unrecognized PLC injury) will subject the central PCL reconstruction to excessive varus and external rotation forces, inevitably leading to premature graft failure.
In the athletic cohort, PCL injuries are most prevalent in contact sports such as American football, rugby, and soccer, as well as in sports involving high-velocity falls like downhill skiing. While isolated PCL injuries in athletes are often managed with rigorous, quadriceps-dominant rehabilitation protocols, the failure of conservative management—manifesting as persistent pain, inability to decelerate, or progressive medial compartment symptoms—serves as a primary trigger for surgical intervention. The demographic profile of the operative patient is thus bimodal, comprising young athletes failing conservative management and victims of high-energy polytrauma requiring comprehensive knee reconstruction.
Detailed Surgical Anatomy and Biomechanics
Structural Anatomy of the Posterior Cruciate Ligament
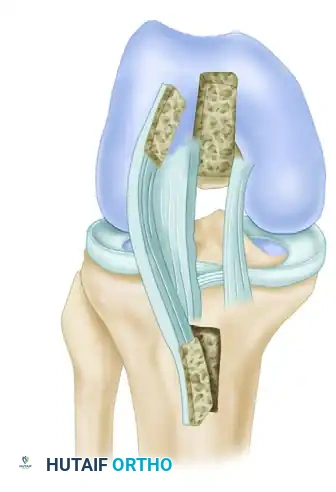
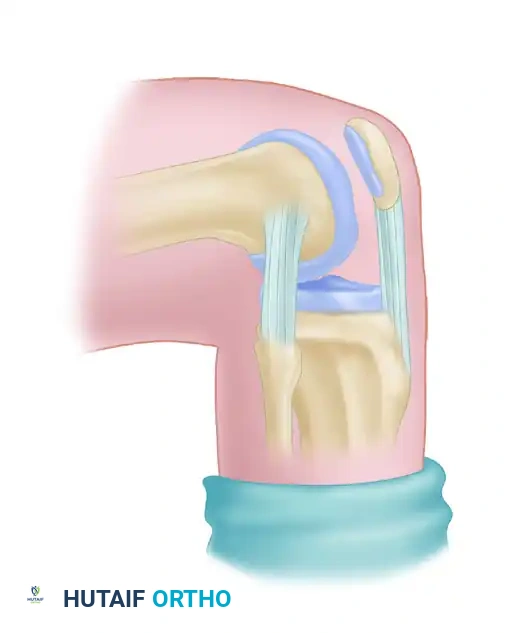
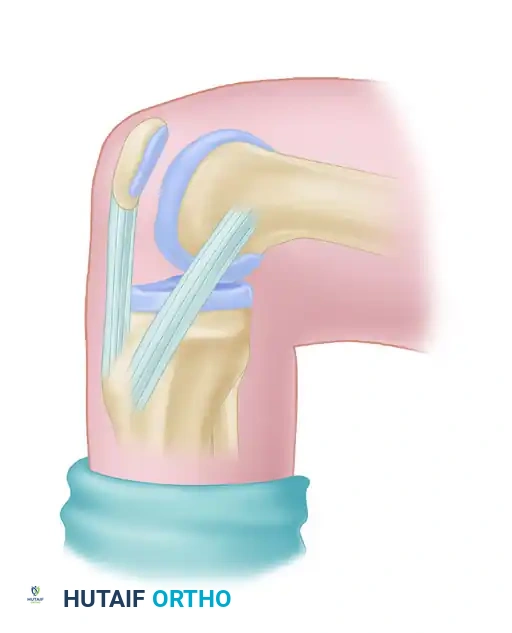
The posterior cruciate ligament is an intra-articular but extrasynovial structure, meaning it is enveloped by a fold of the synovial membrane that excludes it from the synovial cavity proper. It is the largest and strongest ligament in the human knee, possessing a tensile strength approximately twice that of the anterior cruciate ligament. The PCL originates from a broad, crescent-shaped footprint on the anterolateral aspect of the medial femoral condyle, deep within the intercondylar notch. From this femoral origin, the ligament courses posteriorly, laterally, and distally to insert onto the posterior facet of the tibia, located in a depression known as the PCL fovea. This tibial footprint extends over the posterior rim of the tibial plateau, blending with the posterior capsule and the periosteum of the posterior tibia.
Anatomically and biomechanically, the PCL is divided into two distinct functional bundles: the larger anterolateral (AL) bundle and the smaller posteromedial (PM) bundle. The AL bundle constitutes approximately 85% of the ligament's cross-sectional area and substance. Its femoral origin is positioned shallow and high in the intercondylar notch, while its tibial insertion is located more anteriorly and laterally within the PCL fovea. Conversely, the PM bundle originates deeper and lower on the medial femoral condyle and inserts more posteriorly and medially on the tibia. This dual-bundle architecture is not merely an anatomical curiosity but is fundamental to the ligament's complex tensioning pattern throughout the knee's arc of motion.
The meniscofemoral ligaments (MFLs) are critical accessory structures intimately associated with the PCL. These ligaments arise from the posterior horn of the lateral meniscus and course superiorly and medially to insert on the medial femoral condyle, closely flanking the PCL. The anterior meniscofemoral ligament (Ligament of Humphry) passes anterior to the PCL, while the posterior meniscofemoral ligament (Ligament of Wrisberg) passes posterior to it. At least one of these ligaments is present in over 90% of human knees, and both are present in approximately 30%. They serve as secondary restraints to posterior tibial translation and play a vital role in controlling the kinematics of the lateral meniscus during deep flexion. During surgery, these structures must be carefully identified, as an intact Ligament of Humphry can easily be mistaken for an intact AL bundle of the PCL, leading to a false-negative diagnosis of a PCL rupture.
Kinematics and the Concept of Isometry
The biomechanical behavior of the PCL is dictated by the reciprocal tensioning of its two constituent bundles. As the knee moves from extension into flexion, the femoral attachment of the AL bundle rotates anteriorly and superiorly, causing the AL fibers to tighten. Consequently, the AL bundle is the primary restraint to posterior tibial translation at 90 degrees of knee flexion, which is the position of maximum posterior instability in a PCL-deficient knee. Conversely, the PM bundle is relatively lax in flexion but becomes taut as the knee approaches terminal extension. This codominant relationship ensures that the PCL provides continuous kinematic control across the entire range of motion, preventing posterior subluxation and controlling internal rotation of the tibia.
Achieving isometry—or near-isometry—is the absolute cornerstone of a successful PCL reconstruction. Isometry refers to the surgical selection of femoral and tibial attachment sites that maintain a constant distance from one another throughout the knee's range of motion. If a graft is placed in a non-isometric position, it will undergo excessive length changes during flexion and extension. A graft that stretches excessively will eventually undergo plastic deformation and fail (laxity), whereas a graft that shortens excessively will restrict the joint's range of motion and potentially cause articular cartilage damage or graft rupture (capture). Because true absolute isometry does not exist for the entire broad footprint of the PCL, surgeons aim for "favorable isometry," prioritizing the kinematics of the dominant AL bundle.
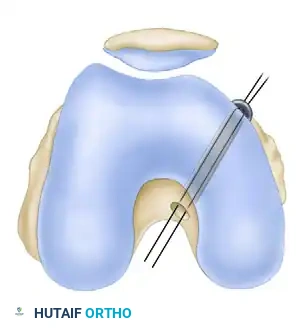
The femoral attachment site is the most critical variable in determining PCL isometry. Errors in femoral tunnel placement profoundly affect graft tension, with deviations in the anteroposterior plane being far more detrimental than those in the proximal-distal plane. If the femoral tunnel is placed too anteriorly (shallow in the notch), the graft will be excessively tight in flexion and loose in extension. If placed too posteriorly (deep in the notch), the graft will be tight in extension and lax in flexion. The most isometric region is located toward the roof of the intercondylar notch, averaging 11 mm from the junction of the notch and the trochlear groove.

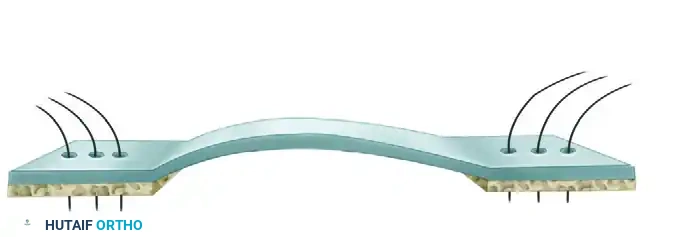
Clinical Pearl: Isometry Testing
A strong suture or wire should be passed through holes drilled in the selected tibial and femoral condyles and attached to an isometer device. A length change of 2 mm or less is acceptable. If the length increases with flexion, the selected site is too distal; if it decreases with flexion, the site is too proximal.
Morgan et al. defined the anatomical origins of the PCL bundles to reproducibly position femoral tunnels:
* Anterolateral Band: 13 mm ± 0.5 mm posterior to the medial articular cartilage–intercondylar wall interface, and 13 mm ± 0.5 mm inferior to the articular cartilage–intercondylar roof interface.
* Posteromedial Band: 8 mm ± 0.5 mm posterior to the medial articular cartilage–intercondylar wall interface, and 20 mm ± 0.5 mm inferior to the articular cartilage–intercondylar roof interface.
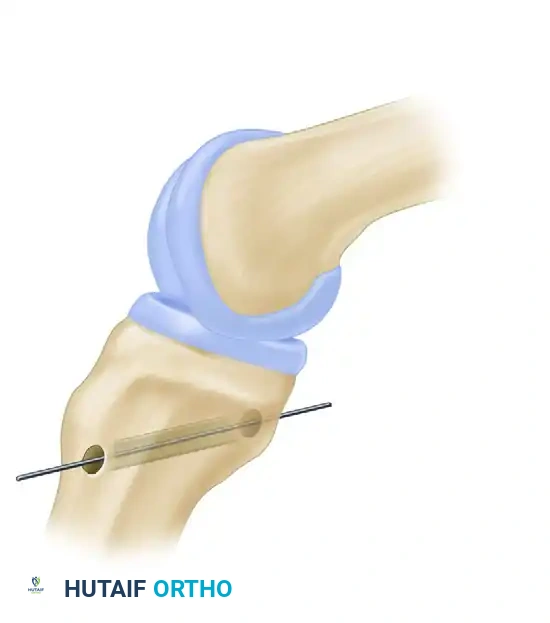
Unlike the highly sensitive femoral site, the tibial attachment is relatively insensitive to proximal-distal or medial-lateral variations regarding length patterns. The anatomical center is located in the PCL fovea, just inferior to the articular margin of the posterior tibia and slightly lateral to the midline. However, the tibial tunnel placement is critical for a different biomechanical reason: mitigating the "killer turn." If the tibial tunnel is drilled too vertically or too centrally, the angle at which the graft exits the posterior tibia and turns toward the femur becomes extremely acute. This sharp angle acts as a fulcrum, causing severe abrasion, mechanical fatigue, and eventual failure of the graft material.
The Meniscofemoral Ligaments and Posterolateral Corner
The interplay between the PCL and the posterolateral corner (PLC) of the knee is a critical concept in orthopedic biomechanics. The PLC, comprising the fibular collateral ligament (FCL), the popliteus tendon, and the popliteofibular ligament, acts as the primary restraint to varus opening and external tibial rotation. Biomechanical studies have unequivocally demonstrated that the PCL and the PLC function synergistically. When the PCL is ruptured, the PLC structures experience significantly increased loads during posterior translation and external rotation. Conversely, if the PLC is deficient, the PCL is subjected to massive varus and rotational forces.
This synergistic relationship dictates that isolated reconstruction of the PCL in the presence of an unrecognized PLC injury is doomed to fail. The reconstructed PCL graft, regardless of its initial fixation strength, cannot withstand the repetitive varus and external rotation moments imparted by a deficient PLC. Over time, the graft will undergo plastic deformation, elongate, and ultimately fail, returning the patient to a state of chronic posterior and rotational instability. Therefore, meticulous evaluation of the posterolateral structures, both clinically and radiographically, is an absolute prerequisite before undertaking PCL reconstruction.
During diagnostic arthroscopy or arthrotomy, the surgeon must also carefully evaluate the meniscofemoral ligaments (Humphry and Wrisberg). As previously noted, these structures often remain intact even in the presence of a complete mid-substance PCL rupture. Their preservation is highly desirable, as they provide residual posterior stability and protect the lateral meniscus. However, their presence can severely confound the intraoperative assessment of PCL integrity.
Surgical Warning: Misdiagnosis of Posterolateral Corner Injury
If either the ligament of Humphry or Wrisberg is intact, the tibia will move only slightly backward during a posterior drawer test with the tibia in marked internal rotation. This can mask a complete PCL tear and lead to a mistaken diagnosis of pure posterolateral rotary instability.
Exhaustive Indications and Contraindications
Clinical Evaluation and Diagnostic Imaging
The clinical evaluation of a suspected PCL injury requires a high index of suspicion and a meticulous physical examination. The hallmark of a PCL-deficient knee is the posterior sag sign, observed when the patient lies supine with the hips and knees flexed to 90 degrees. In a normal knee, the medial tibial plateau extends approximately 1 cm anterior to the medial femoral condyle. In a PCL-deficient knee, this normal step-off is lost, and the tibia sags posteriorly due to gravity. The posterior drawer test, performed at 90 degrees of flexion, quantifies the degree of posterior translation. It is strictly graded: Grade I (0-5 mm translation, tibia remains anterior to condyles), Grade II (6-10 mm translation, tibia is flush with condyles), and Grade III (>10 mm translation, tibia drops posterior to the condyles).
Advanced diagnostic imaging is essential for preoperative planning. Magnetic Resonance Imaging (MRI) is the gold standard for evaluating the structural integrity of the PCL, the menisci, the chondral surfaces, and the collateral ligaments. Acute PCL tears appear as discontinuous, hyperintense, and thickened structures on T2-weighted sagittal images. However, in chronic settings, the PCL may heal in an elongated, non-functional state, appearing deceptively intact on MRI. In such cases, stress radiography becomes invaluable. Bilateral kneeling stress radiographs or Telos device stress views objectively quantify the degree of posterior tibial translation. A side-to-side difference of greater than 8 mm is generally considered indicative of a complete, functionally significant PCL rupture.
Furthermore, the clinical evaluation must exhaustively rule out concomitant injuries. The Dial test, performed at 30 and 90 degrees of knee flexion, is critical for assessing posterolateral corner integrity. Increased external rotation of more than 10 degrees compared to the contralateral limb at 30 degrees suggests an isolated PLC injury, while increased rotation at both 30 and 90 degrees indicates a combined PCL and PLC injury. Varus and valgus stress testing at 0 and 30 degrees must also be meticulously documented. Any failure to identify and concurrently address these peripheral instabilities represents a profound error in surgical judgment.
Indications for Surgical Intervention
The decision to proceed with operative reconstruction of the PCL is highly individualized, balancing the severity of the injury, the chronicity of the symptoms, and the patient's functional demands. Historically, non-operative management was favored for isolated injuries; however, contemporary evidence supporting early surgical intervention to prevent long-term joint degradation has broadened the indications. The absolute and relative indications for PCL reconstruction using a patellar tendon graft are clearly delineated in modern orthopedic practice.
The primary indication for acute surgical intervention is a multiligamentous knee injury. Any combination of a PCL tear with an ACL, PLC, or severe MCL complex injury mandates comprehensive surgical reconstruction to restore joint kinematics and prevent catastrophic functional failure. In these complex scenarios, the PCL reconstruction serves as the central stabilizing pillar around which the peripheral reconstructions are tensioned. Additionally, acute bony avulsion fractures of the PCL from the tibial insertion, if displaced more than 2-3 mm or associated with clinical instability, are absolute indications for surgical repair or reconstruction, as they possess excellent healing potential when anatomically reduced and rigidly fixed.
For isolated PCL injuries, the indications are more nuanced. Acute isolated Grade III tears (>10 mm posterior translation) in young, high-demand athletes are increasingly treated with early reconstruction to expedite return to sport and mitigate the risk of secondary meniscal and chondral damage. In the chronic setting, the primary indication is symptomatic instability that has failed a rigorous, minimum 3-to-6-month trial of conservative management emphasizing quadriceps strengthening. Patients who present with chronic, progressive medial compartment or patellofemoral pain, recurrent effusions, and a demonstrable posterior sag are excellent candidates for reconstruction, provided severe osteoarthritis has not yet developed.
Absolute and Relative Contraindications
The selection of appropriate surgical candidates is as critical as the execution of the technique itself. Proceeding with a PCL reconstruction in the presence of specific contraindications can lead to devastating outcomes, including catastrophic graft failure, intractable infection, or severe exacerbation of underlying joint pathology.
| Category | Specific Contraindication | Rationale and Clinical Implication |
|---|---|---|
| Absolute | Active Joint Infection | Introduction of hardware and avascular graft material into an infected field guarantees persistent sepsis, graft necrosis, and potential joint destruction. |
| Absolute | Severe Osteoarthritis (Kellgren-Lawrence Grade III/IV) | Reconstructing a ligament in a severely degenerated joint will not alleviate arthritic pain and may exacerbate stiffness. Arthroplasty is indicated. |
| Absolute | Uncorrected Malalignment (e.g., Varus Thrust) | Chronic PCL/PLC deficiency often leads to a varus morphotype. Reconstructing the PCL without first performing a High Tibial Osteotomy (HTO) will result in rapid graft stretching and failure due to excessive mechanical overload. |
| Absolute | Inability to Comply with Rehabilitation | PCL rehab is arduous and requires strict adherence to bracing and weight-bearing restrictions. Non-compliance guarantees graft elongation. |
| Relative | Advanced Age with Low Functional Demand | The surgical morbidity and prolonged recovery may outweigh the benefits in sedentary patients who tolerate mild instability well. |
| Relative | Prior Patellar Tendon Harvest (Ipsilateral) | Harvesting a previously utilized or compromised patellar tendon risks patellar fracture, extensor mechanism rupture, or inadequate graft strength. Alternative grafts (quadriceps, allograft) should be considered. |
| Relative | Severe Patellofemoral Chondromalacia | Harvesting a BTB graft may exacerbate anterior knee pain and patellofemoral symptoms in patients with pre-existing severe chondral wear. |
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging and Pre-Operative Templating
Pre-operative planning is a rigorous process that begins long before the patient enters the operating theater. The surgeon must meticulously review all imaging modalities to formulate a precise surgical blueprint. High-resolution MRI is scrutinized not only to confirm the PCL rupture but to evaluate the exact dimensions of the native footprints, the morphology of the intercondylar notch, and the integrity of the extensor mechanism from which the graft will be harvested. The length of the patellar tendon is a critical variable; a tendon that is unusually short may yield a graft that is insufficient to span the long intra-articular distance from the posterior tibia to the medial femoral condyle, necessitating an alternative graft choice or highly modified fixation techniques.
Radiographic templating involves assessing the mechanical axis of the lower extremity using full-length, standing anteroposterior radiographs. As previously emphasized, any significant varus or valgus malalignment must be identified. In chronic cases with a dynamic varus thrust, a staged approach is often mandatory: a proximal tibial osteotomy is performed first to correct the mechanical axis, followed by the soft-tissue ligamentous reconstruction in a subsequent procedure. Failure to template and correct coronal plane malalignment subjects the reconstructed PCL to eccentric loading forces that rapidly exceed the ultimate tensile strength of the graft, leading to inevitable failure.
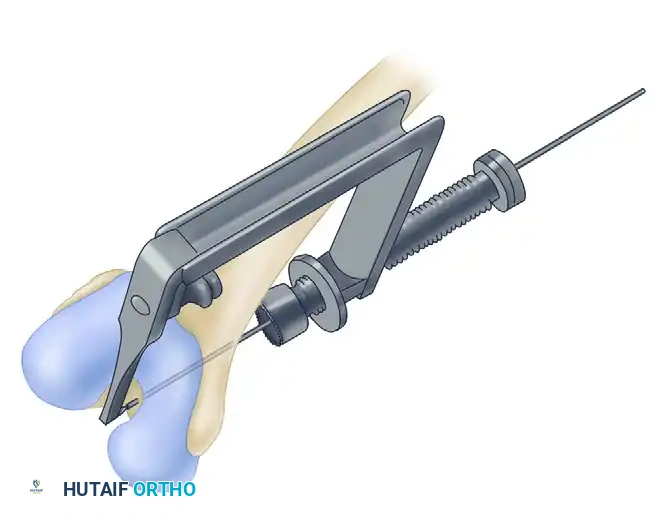
Furthermore, the surgeon must plan the exact trajectory of the tibial and femoral tunnels. The tibial tunnel, in particular, requires careful spatial conceptualization. Because the tunnel must originate on the anteromedial tibia and exit precisely at the PCL fovea on the posterior cortex, the trajectory is long and critically close to the popliteal artery. Pre-operative assessment of the tibial depth and the optimal starting point (often more distal and anterolateral than traditionally taught) is essential to minimize the "killer turn" angle and ensure the safety of the posterior neurovascular structures during reaming.
Operating Room Setup and Anesthesia Considerations
The operating room setup for a PCL reconstruction must be highly organized, accommodating the need for extensive equipment, fluoroscopy, and potentially multiple surgical assistants. The procedure is typically performed under general anesthesia to ensure complete muscle relaxation, which is vital for accurately assessing joint laxity and manipulating the heavy lower extremity during tunnel preparation and graft tensioning. Regional anesthesia, such as an adductor canal block or a femoral nerve block, is frequently utilized as an adjunct to provide robust postoperative analgesia, thereby facilitating early rehabilitation and minimizing opioid consumption.
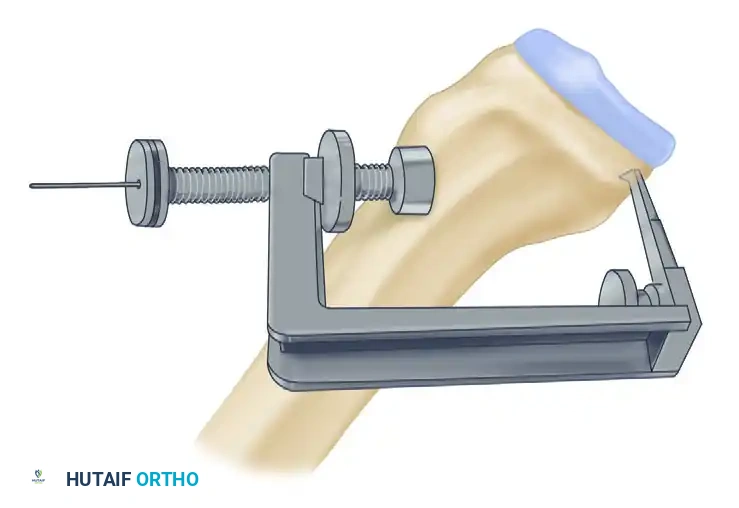
A well-padded thigh tourniquet is applied as proximally as possible to maximize the surgical field. Intravenous prophylactic antibiotics (typically a first-generation cephalosporin) are administered within one hour prior to tourniquet inflation. The use of a specialized leg holder or a lateral post is a matter of surgeon preference, but it must allow for unrestricted hyperflexion of the knee past 110 degrees, which is often necessary for adequate visualization of the femoral footprint deep within the intercondylar notch. Additionally, the setup must allow seamless integration of a C-arm fluoroscopy unit, which is frequently brought in horizontally to confirm the precise location of the tibial guide pin before over-reaming.
The surgical instrumentation must be meticulously verified prior to the incision. Standard ACL reconstruction sets are insufficient. The surgical team must have access to specific PCL instrumentation, including specialized posterior tibial drill guides, curved curettes, posterior capsule retractors (such as a smooth spoon or a specialized PCL retractor), and a variety of fixation devices including interference screws, suspensory cortical buttons, and AO malleolar screws with spiked washers. The availability of a high-quality arthroscopic pump system is also critical to maintain joint distension and clear visualization in the face of inevitable venous bleeding from the posterior capsule and osseous tunnels.
Patient Positioning and Examination Under Anesthesia
Patient positioning is the foundational step of the surgical procedure. The patient is placed supine on the operating table. The non-operative leg is carefully padded and placed in a well-leg holder or secured flat on the table, ensuring that it does not obstruct the surgeon's mobility or the positioning of the fluoroscopy unit. The operative leg is prepped and draped in a standard sterile fashion, allowing access from the proximal thigh to the toes. A sterile tourniquet is often used to maintain a bloodless field during the open portions of the procedure, particularly during graft harvest and the posteromedial arthrotomy.
Once the patient is anesthetized and positioned, a comprehensive Examination Under Anesthesia (EUA) is mandatory. The EUA provides the most accurate assessment of joint laxity, free from patient guarding or muscle spasm. The surgeon systematically evaluates the anterior drawer, posterior drawer, Lachman test, pivot shift, varus/valgus stress at 0 and 30 degrees, and the Dial test at 30 and 90 degrees. This final clinical assessment confirms the preoperative diagnosis and ensures that no subtle peripheral instabilities have been missed.
During the EUA, the surgeon must specifically note the resting position of the tibia relative to the femur. In a chronic PCL-deficient knee, the tibia will be posteriorly subluxated. The surgeon must confirm that the tibia can be easily and fully reduced to its anatomical neutral position
Clinical & Radiographic Imaging Archive