BACKGROUND
Resection of the proximal tibia includes the removal of one-half to two-thirds of the tibia along with a portion of all muscles that insert on it as well as the entire popliteus muscle, in combination with an extra-articular resection of the proximal tibiofibular joint. The peroneal nerve is preserved. Of all anatomic locations in which major bone resections and prosthetic reconstructions are done, the proximal tibia is considered to be the site in which surgery is the most complicated, where rates of complications are highest, and whose functional outcome is poorest. The major contributors to these complications include the lack of muscle coverage along the anteromedial aspect of the tibia, the relatively small caliber of the blood vessels around the leg, and the need to include the insertion site of the extensor mechanism with the removed surgical specimen. In the past, these difficulties made it impossible to perform limb-sparing surgery, and above-knee amputations were the only surgical option for malignant tumors at this site. The limb-sparing technique illustrated in this chapter allows a safe approach to the dissection of popliteal vessels and to the resection and replacement of the proximal one-third to two-thirds of the tibia. Preoperative evaluation of tumor extent requires a detailed understanding of the anatomy and careful evaluation by computed tomography (CT), magnetic resonance (MR) imaging, bone scintigraphy, and biplane angiography. Types of possible reconstructions include primary arthrodesis, prosthetic replacement, and allograft replacement. We prefer the prosthetic replacements because of the high rates of nonunion and infections associated with allograft reconstruction and the poor function of an arthrodesed knee. The use of a gastrocnemius rotational flap is a key factor in achieving adequate soft tissue coverage of the prosthesis and in restoring function of the extensor mechanism. ## ANATOMY
Knee Joint and Cruciate Ligaments The knee joint is seldom directly invaded by tumors of the proximal tibia. When it does occur, invasion is usually the result of a pathologic fracture, contamination of an improper biopsy technique, or tumor extension along the cruciate ligaments. The presence of hemarthrosis is suggestive of intra-articular disease. Involvement of the cruciate ligaments is often not determined until the time of surgery, although an MR imaging scan is a reliable means of determining cruciate ligament involvement preoperatively. An extra-articular resection (ie, en bloc resection of the proximal tibia, joint capsule, and femoral condyles) should be considered if nodules are identified on the cruciate ligaments. ## Extensor Mechanism The attachment site of the extensor mechanism at the tibial tuberosity is resected en bloc with the proximal tibia. Reconstruction of this mechanism is essential for a functioning extremity. ## Popliteal Trifurcation The popliteal artery divides into the anterior tibial artery, the posterior tibial artery, and the peroneal artery at the inferior border of the popliteus muscle. The popliteal trifurcation is actually composed of two bifurcations. The first is found where the anterior tibial artery arises from the popliteal artery, which then continues as the tibioperoneal trunk. The anterior tibial artery is the first branch and arises at the inferior border of the popliteus muscle. The second bifurcation is found where the peroneal artery and the posterior tibial artery arise from the tibioperoneal trunk; thus, this bifurcation is distal to the anterior tibial artery. It is almost always necessary to ligate the anterior tibial artery at the time of resection, whereas the other vessels must be identified before ligation. A unique and fortuitous anatomic feature is that the popliteus muscle covers the posterior surface of the tibia, which affords an excellent boundary between the posterior soft tissue extension from the tibia and the neurovascular bundle of the lower extremity. This is in contrast to what occurs at the distal femur in which the posterior aspect is covered solely by the popliteal fat. ## Tibiofibular Joint The proximal tibiofibular joint is located close to the posterolateral aspect of the proximal tibia. Histologic studies show that tumors involving the proximal tibia have a high incidence of extension and involvement of the periscapular tissues of the tibiofibular joint. To obtain a satisfactory surgical margin while performing a resection of the proximal tumor, it is necessary to remove this joint en bloc, that is, perform an extra-articular resection. This is routine procedure for all highgrade sarcomas of the proximal tibia. ## Subcutaneous Location of the Tibia The entire medial aspect of the tibia lies in a subcutaneous location and remains there after resection and reconstruction approaches had been carried out. This had been a major source of primary and secondary infections, which, in turn, frequently necessitated above-knee amputation.
 ---
---
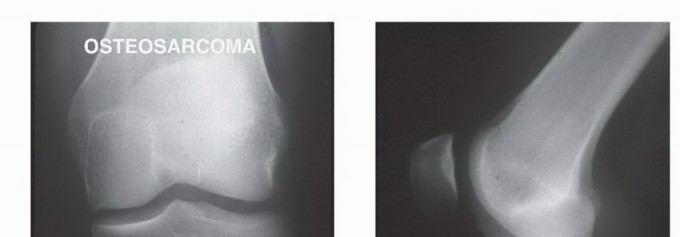
 ### FIG 1 • A. Anteroposterior and (B) lateral plain radiographs showing osteosarcoma of the proximal tibia in a 17-year-old female patient. Following treatment with neoadjuvant chemotherapy, this patient was referred to proximal tibia resection with endoprosthetic reconstruction. Today, the routine transfer of the medial gastrocnemius muscle anteriorly to cover the prosthesis is considered a reliable method of prosthetic coverage. It also provides a method of extensor mechanism reconstruction. It is a simple and reliable means of decreasing the incidence of infection, flap necrosis, and secondary amputation. 4 ## INDICATIONS AND CONTRAINDICATIONS Primary bone sarcomas of the proximal tibia(FIG 1) Benign aggressive tumors associated with extensive bone destruction(FIG 2) Metastatic tumors associated with extensive bone destruction The major contraindications to limb sparing are neurovascular involvement and compromise as well as extensive soft tissue tumor involvement that precludes adequate prosthetic coverage. ## IMAGING AND OTHER STAGING STUDIES
### FIG 1 • A. Anteroposterior and (B) lateral plain radiographs showing osteosarcoma of the proximal tibia in a 17-year-old female patient. Following treatment with neoadjuvant chemotherapy, this patient was referred to proximal tibia resection with endoprosthetic reconstruction. Today, the routine transfer of the medial gastrocnemius muscle anteriorly to cover the prosthesis is considered a reliable method of prosthetic coverage. It also provides a method of extensor mechanism reconstruction. It is a simple and reliable means of decreasing the incidence of infection, flap necrosis, and secondary amputation. 4 ## INDICATIONS AND CONTRAINDICATIONS Primary bone sarcomas of the proximal tibia(FIG 1) Benign aggressive tumors associated with extensive bone destruction(FIG 2) Metastatic tumors associated with extensive bone destruction The major contraindications to limb sparing are neurovascular involvement and compromise as well as extensive soft tissue tumor involvement that precludes adequate prosthetic coverage. ## IMAGING AND OTHER STAGING STUDIES
Computed Tomography and Magnetic Resonance Imaging CT and MR imaging are useful to determine the extent of cortical destruction and intramedullary and soft tissue extensions of the primary tumor. These data are essential for determining the level of tibial resection, which is 3 to 5 cm distal to the area of intramedullary tumor involvement. MR imaging can also reveal skip lesions, which may affect the extent of tibial resection(FIGS 3 and 4).
 ---
---
FIG 2 • A. Anteroposterior plain radiograph showing giant cell tumor of the proximal tibia in a 48-year-old female patient. This radiograph was done for persistent knee pain and this large lesion, which filled the metaepiphyseal regions, was missed by the physician who initially interpreted the film. B. Anteroposterior and lateral plain radiographs (C) were taken again 5 months later because of additional symptoms. This time, there was evidence of overwhelming extensive bone destruction. (continued)
 ---
---
 ### FIG 2 •
(continued)
D. Axial CT showing tumor filling the entire metaphysis of the proximal tibia with thinning and ballooning of the cortices. The patient was treated with proximal tibia endoprosthetic reconstruction. E. A sagittal cut through the surgical specimen shows the large tumoral mass and the cortical destruction.
### FIG 2 •
(continued)
D. Axial CT showing tumor filling the entire metaphysis of the proximal tibia with thinning and ballooning of the cortices. The patient was treated with proximal tibia endoprosthetic reconstruction. E. A sagittal cut through the surgical specimen shows the large tumoral mass and the cortical destruction.
 ---
---

 ###
FIG 3 • A,B. Anteroposterior and lateral plain radiographs, CT (C), and MR imaging (D) showing osteosarcoma of the proximal tibia. These studies demonstrate that the tumor is associated with minimal destruction of the cortices and that there is no soft tissue extension. The MR scan also accurately depicts the distal point of the intramedullary tumor extension. These findings will assist in determining the osteotomy level and the amount of surrounding soft tissue to be resected en bloc with the tumor.
###
FIG 3 • A,B. Anteroposterior and lateral plain radiographs, CT (C), and MR imaging (D) showing osteosarcoma of the proximal tibia. These studies demonstrate that the tumor is associated with minimal destruction of the cortices and that there is no soft tissue extension. The MR scan also accurately depicts the distal point of the intramedullary tumor extension. These findings will assist in determining the osteotomy level and the amount of surrounding soft tissue to be resected en bloc with the tumor.
 ---
---
 ### FIG 4 • Anteroposterior plain radiograph (A) and CT (B) showing osteosarcoma of the proximal tibia with cortical destruction and soft tissue extension of the tumor.
### FIG 4 • Anteroposterior plain radiograph (A) and CT (B) showing osteosarcoma of the proximal tibia with cortical destruction and soft tissue extension of the tumor.
Angiography Biplane angiography(FIG 5) is used for local arterial evaluation, especially if CT has revealed posterior soft tissue extension. The anteroposterior view is used to evaluate the popliteal bifurcation; of particular relevance is the integrity of the posterior tibial artery, which may be the sole blood supply to the leg after resection. The lateral view is essential for evaluating the interval between the tibia and the neurovascular bundle. For example, the popliteus muscle often separates a posterior tumor mass from the vessels. This is reflected as a clear interval on the lateral angiogram and serves as an indication that there is an adequate resection margin. Ligation of the anterior tibial artery is almost always required. The peroneal artery may be involved by tumors that have a large posterior compartment. Two of the major vessels may be ligated in a young patient, without jeopardizing the possibility of a viable and functional extremity. The posterior tibial artery is almost never involved by tumor. ## SURGICAL MANAGEMENT There are three major steps involved in successful resection and reconstruction of tumors of the proximal tibia: Resection of the tumor Prosthetic reconstruction of the skeletal defect and knee joint Reconstruction of the extensor mechanism and soft tissue coverage of the prosthesis with a gastrocnemius flap 1,3
 ---
---
 FIG 5 • An angiogram showing a lateral view of the popliteal artery. The space between the tumor in the proximal tibia and the popliteal bifurcation is best visualized by this study. The popliteal artery (
P
), tibioperoneal trunk (
TP
), and anterior tibia (
AT
) arteries are all identifiable. It is essential that the soft tissue posterior to the tumor mass (
curved arrow
) be free of cancer along the popliteal artery and tibioperoneal trunk. The popliteus muscle covers the bone in this interval and usually protects the vessels from tumor invasion. A tumor (
T
) blush (
small arrows
) is seen anteriorly. (From Malawer MM, McHale KA. Limb-sparing surgery for high-grade malignant tumors of the proximal tibia: surgical technique and a method of extensor mechanism reconstruction. Clin Orthop Relat Res 1989;239:231-248.)
FIG 5 • An angiogram showing a lateral view of the popliteal artery. The space between the tumor in the proximal tibia and the popliteal bifurcation is best visualized by this study. The popliteal artery (
P
), tibioperoneal trunk (
TP
), and anterior tibia (
AT
) arteries are all identifiable. It is essential that the soft tissue posterior to the tumor mass (
curved arrow
) be free of cancer along the popliteal artery and tibioperoneal trunk. The popliteus muscle covers the bone in this interval and usually protects the vessels from tumor invasion. A tumor (
T
) blush (
small arrows
) is seen anteriorly. (From Malawer MM, McHale KA. Limb-sparing surgery for high-grade malignant tumors of the proximal tibia: surgical technique and a method of extensor mechanism reconstruction. Clin Orthop Relat Res 1989;239:231-248.)
TECHNIQUES

---


 ### TECH FIG 2 •
(continued)
C. Dissection and exposure of the neurovascular bundle is often difficult because the tumor has distorted the normal anatomy. It requires splitting of the soleus muscle for most of its length. Care should be taken to identify and protect all major vascular branches prior to any ligation. The anterior tibial artery, which is the first of the popliteal artery, is located at the inferior border of the popliteus muscle. As it passes directly anterior through the interosseous membrane, it tethers the entire neurovascular bundle. (A,C: From Malawer MM, McHale KA. Limb-sparing surgery for high-grade malignant tumors of the proximal tibia: surgical technique and a method of extensor mechanism reconstruction. Clin Orthop Relat Res 1989;239:231-248.)
### TECH FIG 2 •
(continued)
C. Dissection and exposure of the neurovascular bundle is often difficult because the tumor has distorted the normal anatomy. It requires splitting of the soleus muscle for most of its length. Care should be taken to identify and protect all major vascular branches prior to any ligation. The anterior tibial artery, which is the first of the popliteal artery, is located at the inferior border of the popliteus muscle. As it passes directly anterior through the interosseous membrane, it tethers the entire neurovascular bundle. (A,C: From Malawer MM, McHale KA. Limb-sparing surgery for high-grade malignant tumors of the proximal tibia: surgical technique and a method of extensor mechanism reconstruction. Clin Orthop Relat Res 1989;239:231-248.)
2. ## Detachment of Vascular Bundle Applying posterior traction proximal to the popliteal artery permits visualization of the takeoff of the anterior tibial artery and its accompanying veins. The anterior tibial vessels are individually ligated, allowing the entire neurovascular bundle to fall away from the posterior aspect of the tibia and/or tumor(TECH FIG 3).
 ---
---
 ### TECH FIG 3 • Ligation of the anterior tibial vessels allows the entire neurovascular bundle to fall away from the posterior aspect of the tibia. (From Malawer MM, McHale KA. Limb-sparing surgery for highgrade malignant tumors of the proximal tibia: surgical technique and a method of extensor mechanism reconstruction. Clin Orthop Relat Res 1989;239:231-248.) If the mass is a large one, there is a possibility that the peroneal artery must be ligated as well, leaving the posterior tibial artery as the single blood supply to the leg. Further posterior mobilization of the popliteal vessels is achieved by ligation of the inferior geniculate vessels.
### TECH FIG 3 • Ligation of the anterior tibial vessels allows the entire neurovascular bundle to fall away from the posterior aspect of the tibia. (From Malawer MM, McHale KA. Limb-sparing surgery for highgrade malignant tumors of the proximal tibia: surgical technique and a method of extensor mechanism reconstruction. Clin Orthop Relat Res 1989;239:231-248.) If the mass is a large one, there is a possibility that the peroneal artery must be ligated as well, leaving the posterior tibial artery as the single blood supply to the leg. Further posterior mobilization of the popliteal vessels is achieved by ligation of the inferior geniculate vessels.
gastrocnemius muscle is detached at its muscle-tendon junction and interface with the lateral gastrocnemius, mobilized and rotated anteriorly to cover the prosthesis. At its upper pole, the muscle flap is sutured to the patellar tendon to reinforce the prosthesis and bone graft reconstruction.
 ---
---



 ### TECH FIG 7 • A. Illustration showing reconstruction of the extensor mechanism, which has three components: attachment of the patellar tendon to the prosthesis, reinforcement of the attachment site with bone graft, and overlying medial gastrocnemius flap. B. Intraoperative photograph showing the patellar tendon sutured to the prosthesis and underlying bone graft. C-F. Alternatively, a circumferential polyethylene terephthalate (Trevira; Implantcast Gmbh, Buxtehude, Germany) tube may be applied on the prosthesis to which the patellar tendon and surrounding muscles can be sutured. 2 ( A: From Malawer M. Proximal tibial resection with endoprosthetic reconstruction. In: Malawer MM, Sugarbaker PH, eds. Musculoskeletal Cancer Surgery: Treatment of Sarcomas and Allied Diseases. Dordrecht: Kluwer Academic Publishers, 2001:485-504.) Suction drains are positioned along the muscle envelope, and the fasciocutaneous flaps are pulled and closed, usually leaving a gap over the medial gastrocnemius flap, which necessitates coverage with a split-thickness skin graft taken from the ipsilateral thigh(TECH FIG 9).
### TECH FIG 7 • A. Illustration showing reconstruction of the extensor mechanism, which has three components: attachment of the patellar tendon to the prosthesis, reinforcement of the attachment site with bone graft, and overlying medial gastrocnemius flap. B. Intraoperative photograph showing the patellar tendon sutured to the prosthesis and underlying bone graft. C-F. Alternatively, a circumferential polyethylene terephthalate (Trevira; Implantcast Gmbh, Buxtehude, Germany) tube may be applied on the prosthesis to which the patellar tendon and surrounding muscles can be sutured. 2 ( A: From Malawer M. Proximal tibial resection with endoprosthetic reconstruction. In: Malawer MM, Sugarbaker PH, eds. Musculoskeletal Cancer Surgery: Treatment of Sarcomas and Allied Diseases. Dordrecht: Kluwer Academic Publishers, 2001:485-504.) Suction drains are positioned along the muscle envelope, and the fasciocutaneous flaps are pulled and closed, usually leaving a gap over the medial gastrocnemius flap, which necessitates coverage with a split-thickness skin graft taken from the ipsilateral thigh(TECH FIG 9).
 ---
---

 ###
TECH FIG 8 • Illustrations (A-C) and intraoperative photographs
(continued)
###
TECH FIG 8 • Illustrations (A-C) and intraoperative photographs
(continued)
 ---
---

 TECH FIG 8 •
(continued)
(D-F) showing soft tissue coverage around the prosthesis. The soleus muscle is pulled anteriorly to cover the middle segment of the prosthesis, and the medial gastrocnemius is transposed to cover its proximal segment. The medial sural artery to the medial gastrocnemius muscle is carefully preserved. The medial gastrocnemius muscle is detached at its muscle-tendon junction and interfaced with the lateral gastrocnemius, mobilized and rotated anteriorly to cover the prosthesis. It is sutured to the border of the anterior muscles and the patellar tendon, forming a complete soft tissue envelope around the prosthesis. (A,B: From Malawer MM, McHale KA. Limb-sparing surgery for highgrade malignant tumors of the proximal tibia: surgical technique and a method of extensor mechanism reconstruction. Clin Orthop Relat Res 1989;239:231-248; C: From Malawer M. Proximal tibial resection with endoprosthetic reconstruction. In: Malawer MM, Sugarbaker PH, eds. Musculoskeletal Cancer Surgery: Treatment of Sarcomas and Allied Diseases. Dordrecht: Kluwer Academic Publishers, 2001:485-504.)
TECH FIG 8 •
(continued)
(D-F) showing soft tissue coverage around the prosthesis. The soleus muscle is pulled anteriorly to cover the middle segment of the prosthesis, and the medial gastrocnemius is transposed to cover its proximal segment. The medial sural artery to the medial gastrocnemius muscle is carefully preserved. The medial gastrocnemius muscle is detached at its muscle-tendon junction and interfaced with the lateral gastrocnemius, mobilized and rotated anteriorly to cover the prosthesis. It is sutured to the border of the anterior muscles and the patellar tendon, forming a complete soft tissue envelope around the prosthesis. (A,B: From Malawer MM, McHale KA. Limb-sparing surgery for highgrade malignant tumors of the proximal tibia: surgical technique and a method of extensor mechanism reconstruction. Clin Orthop Relat Res 1989;239:231-248; C: From Malawer M. Proximal tibial resection with endoprosthetic reconstruction. In: Malawer MM, Sugarbaker PH, eds. Musculoskeletal Cancer Surgery: Treatment of Sarcomas and Allied Diseases. Dordrecht: Kluwer Academic Publishers, 2001:485-504.)
 ---
---


 ###
TECH FIG 9 • A-E. Suction drains are positioned along the muscle envelope, and the fasciocutaneous flaps are pulled and closed, usually leaving a gap over the medial gastrocnemius flap, which necessitates coverage with a split-thickness skin graft, taken from the ipsilateral thigh.
(continued)
###
TECH FIG 9 • A-E. Suction drains are positioned along the muscle envelope, and the fasciocutaneous flaps are pulled and closed, usually leaving a gap over the medial gastrocnemius flap, which necessitates coverage with a split-thickness skin graft, taken from the ipsilateral thigh.
(continued)
 ---
---
 TECH FIG 9 •
(continued)
Anteroposterior (F) and lateral plain radiographs (G) showing a proximal tibia endoprosthetic reconstruction.
## PEARLS AND PITFALLS
Surgical ▪ Long anteromedial incision considerations ▪ Ligation of the anterior tibial artery allows retraction of the vascular bundle away from the proximal tibia and enables safe resection. Reconstruction ▪ Reconstruction of the proximal tibial defect with uncemented prostheses for primary bone sarcomas in young adults and cemented prostheses for metastatic lesions
1.
Reconstruction of the extensor mechanism composed of three components: attachment of the patellar tendon stump to the prosthesis, reinforcement with a bone graft, and overlaying of a medial gastrocnemius flap.
2.
Viable soft tissue coverage of the entire length of the prosthesis: the soleus muscle for its middle third and medial gastrocnemius or its proximal third Rehabilitation ▪ Prolonged immobilization of the operated extremity in full extension followed by gradual range-of-motion exercises are essential for restoring function of the extensor mechanism.
## POSTOPERATIVE CARE
The extremity is kept elevated and in full extension to avoid tension on the reconstructed patellar tendon for 5 days. Continuous suction is required for 3 to 5 days, and perioperative intravenous antibiotics are continued until the drainage tubes are removed. If there is no evidence of significant swelling by the end of the fifth day, the patient is allowed to walk with weight bearing as tolerated for 10 to 15 minutes at a time. If the extremity remains free of swelling, a gradual increment in exercise is allowed. The knee is kept fully extended in a knee immobilizer for 6 weeks, by the end of which gradual passive and active flexion of the knee joint are allowed.
## OUTCOMES
Proximal tibia resections are associated with considerably higher rates of flap ischemia, deep infection, and prosthetic loosening than limb-sparing resections at other sites, such as the proximal humerus and the proximal and distal aspects of the femur.
TECH FIG 9 •
(continued)
Anteroposterior (F) and lateral plain radiographs (G) showing a proximal tibia endoprosthetic reconstruction.
## PEARLS AND PITFALLS
Surgical ▪ Long anteromedial incision considerations ▪ Ligation of the anterior tibial artery allows retraction of the vascular bundle away from the proximal tibia and enables safe resection. Reconstruction ▪ Reconstruction of the proximal tibial defect with uncemented prostheses for primary bone sarcomas in young adults and cemented prostheses for metastatic lesions
1.
Reconstruction of the extensor mechanism composed of three components: attachment of the patellar tendon stump to the prosthesis, reinforcement with a bone graft, and overlaying of a medial gastrocnemius flap.
2.
Viable soft tissue coverage of the entire length of the prosthesis: the soleus muscle for its middle third and medial gastrocnemius or its proximal third Rehabilitation ▪ Prolonged immobilization of the operated extremity in full extension followed by gradual range-of-motion exercises are essential for restoring function of the extensor mechanism.
## POSTOPERATIVE CARE
The extremity is kept elevated and in full extension to avoid tension on the reconstructed patellar tendon for 5 days. Continuous suction is required for 3 to 5 days, and perioperative intravenous antibiotics are continued until the drainage tubes are removed. If there is no evidence of significant swelling by the end of the fifth day, the patient is allowed to walk with weight bearing as tolerated for 10 to 15 minutes at a time. If the extremity remains free of swelling, a gradual increment in exercise is allowed. The knee is kept fully extended in a knee immobilizer for 6 weeks, by the end of which gradual passive and active flexion of the knee joint are allowed.
## OUTCOMES
Proximal tibia resections are associated with considerably higher rates of flap ischemia, deep infection, and prosthetic loosening than limb-sparing resections at other sites, such as the proximal humerus and the proximal and distal aspects of the femur.
The lower survival data for prosthetic replacements at the lower tibia (80% at 10 years compared with 95% for the others) are most likely attributable to the complexity of the surgical procedure and the soft tissue reconstruction, breakage of the polyethylene component, and mechanical failure. In addition, impairment of the extensor mechanism is still the most prominent functional compromise after this resection. The incidence of infection has been dramatically decreased by the use of a gastrocnemius muscle flap. Strict adherence to postoperative management guidelines has also decreased the incidence of limb edema, wound problems, and magnitude of extensor mechanism dysfunction.
## COMPLICATIONS
Limb edema Flap ischemia to full-thickness necrosis Deep periprosthetic infection Dysfunctional extensor mechanism and extension lag Prosthetic loosening ## REFERENCES
1. Bickels J, Wittig JC, Kollender Y, et al. Reconstruction of the extensor mechanism after proximal tibia endoprosthetic replacement. J Arthroplasty 2001;16:856-862.
2.
Gosheger G, Hillmann A, Lindner N, et al. Soft-tissue reconstruction of megaprostheses using a trevira tube. Clin Orthop Relat Res 2001;393:264-271.
3.
Malawer MM, McHale KA. Limb-sparing surgery for high-grade malignant tumors of the proximal tibia: surgical technique and a method of extensor mechanism reconstruction. Clin Orthop Relat Res 1989;231:231-248.
4.
Malawer MM, Price WM. Gastrocnemius transposition flap in conjunction with limb-sparing surgery for primary bone sarcomas around the knee. Plast Reconstr Surg 1984;73:741-750.
