Posterior Deltoid-to-Triceps Transfer: Comprehensive Surgical Guide
Key Takeaway
The posterior deltoid-to-triceps transfer, pioneered by Moberg, is a critical reconstructive procedure designed to restore active elbow extension in patients with tetraplegia. By transferring the posterior deltoid to the triceps insertion, surgeons can re-establish the biomechanical linkage necessary for overhead reach, wheelchair transfers, and pressure relief. This guide details the surgical approach, graft interposition techniques, and rigorous postoperative protocols required for optimal functional outcomes.
Introduction and Biomechanical Rationale
The restoration of active elbow extension is arguably one of the most profoundly life-altering reconstructive procedures available to patients with cervical spinal cord injuries, specifically those with C5 or C6 tetraplegia. In these patients, the triceps brachii (innervated by C7) is paralyzed, while the deltoid (innervated by C5) remains functional. The inability to actively extend the elbow severely limits the spatial volume of reach, compromises the ability to perform independent wheelchair transfers, and prevents effective pressure relief maneuvers, thereby increasing the risk of decubitus ulcers.
The Posterior Deltoid-to-Triceps Transfer, originally popularized by Moberg and subsequently modified by various authors including Hentz and Lacey, leverages the preserved posterior third of the deltoid muscle. By rerouting this functional muscle unit to the distal triceps aponeurosis or directly to the olecranon, the surgeon re-establishes the extensor mechanism of the elbow.
Clinical Pearl: Elbow extension must be present or surgically reconstructed to stabilize the elbow against the significant flexion moment generated by other transfers. For example, if a brachioradialis transfer is planned for wrist extension, the lack of an antagonistic elbow extensor will result in the brachioradialis simply flexing the elbow rather than extending the wrist, reducing the transfer power significantly.
Preoperative Assessment and Indications
Patient Selection
The ideal candidate for a posterior deltoid-to-triceps transfer is a patient with a C5 or C6 spinal cord injury who demonstrates:
* Absent or Grade 0-1 Triceps Strength: Complete loss of active elbow extension.
* Grade 4 or 5 Posterior Deltoid Strength: The donor muscle must have near-normal power to overcome the resistance of the soft tissues and gravity.
* Supple Elbow Joint: Full passive range of motion (ROM) of the elbow is a strict prerequisite. Any flexion contractures must be addressed prior to or concurrent with the transfer.
Evaluation of Synergistic Muscles
A comprehensive manual muscle testing (MMT) examination is mandatory. Special attention must be paid to the brachioradialis.
Surgical Warning: Only when the brachioradialis muscle has Grade 4 power can it be reliably transferred to provide wrist extension. The power of the brachioradialis can be graded by palpation over the muscle mass against resisted elbow flexion with the forearm in neutral rotation.
Surgical Anatomy
A profound understanding of the posterior shoulder and arm anatomy is required to safely harvest the posterior deltoid without compromising its neurovascular pedicle.
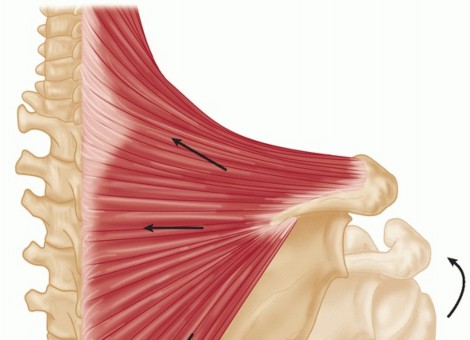
* The Deltoid Muscle: Composed of anterior, middle, and posterior fibers. The posterior fibers arise from the lower lip of the posterior border of the spine of the scapula and insert into the deltoid tuberosity of the humerus.
* Neurovascular Bundle: The axillary nerve and the posterior circumflex humeral artery enter the deltoid on its deep surface, approximately 5 to 7 cm distal to the acromion. Dissection proximal to this neurovascular hilum will result in denervation of the transfer.
Surgical Technique: Posterior Deltoid-to-Triceps Transfer (Modified Moberg)
Patient Positioning
- Place the patient in the lateral decubitus position with the operative arm facing upward.
- Ensure all bony prominences are meticulously padded to prevent pressure sores, a critical consideration in the insensate patient.
- Drape the arm free to allow full, unrestricted movement of the shoulder and elbow during the procedure. A sterile tourniquet may be applied high on the arm, though the proximal dissection often extends above the tourniquet line.
Incision and Deltoid Harvest
- Make a 10- to 13-cm longitudinal incision along the posterior border of the deltoid muscle, extending distally down to the insertion of the muscle at the deltoid tuberosity.
- Raise thick fasciocutaneous flaps over the fascia of the deltoid to expose the muscle belly and identify its humeral insertion.
- Using a periosteal elevator and sharp dissection, elevate the posterior third to half of the deltoid tendon. It is imperative to harvest a robust strip of the periosteal insertion to provide strong tissue for the subsequent weave.
Figure 1: The posterior border of the deltoid muscle belly is isolated. The surgeon must preserve as much of the tendinous and periosteal insertion as possible to facilitate secure distal fixation.
- Place this mobilized portion of the deltoid under slight tension. Gently split the muscle fibers in a distal-to-proximal direction.
- Critical Step: As you split the fibers proximally, continuously palpate and visually inspect the deep surface of the muscle for the axillary nerve and posterior circumflex humeral vessels. End the proximal dissection immediately when this neurovascular hilum is identified to prevent iatrogenic denervation.
- The underlying triceps generally is atrophied in these patients, making the posterior deltoid edge easily palpable and distinct.
Triceps and Olecranon Exposure
- Through a separate curved longitudinal incision over the posterior elbow, expose the distal triceps aponeurosis and its insertion onto the olecranon. The incision should be placed slightly medial or lateral to the midline to prevent a scar directly over the bony prominence of the olecranon.
- Identify the musculotendinous junction of the triceps.
Graft Interposition and Tendon Weave
The method of connecting the posterior deltoid to the triceps depends entirely on the available length and the degree of overlap.
Scenario A: Adequate Overlap (Direct Transfer)
If there is adequate overlap of the tendinous portions of the deltoid insertion and the proximal portion of the triceps aponeurosis, the transfer can be accomplished without an interposition graft, as described by Hentz et al.
Scenario B: Inadequate Overlap (Grafting Required)
If the overlap does not provide adequate length for a secure weave fixation, a free tendon graft is necessary. Several graft sources have been validated in the literature:
* Great Toe Extensors: Originally utilized by Moberg.
* Anterior Tibial Tendon: Advocated by Lacey et al. for its robust cross-sectional area.
* Fascia Lata: Utilized by Hentz et al., providing a broad sheet for a secure, multi-point weave.
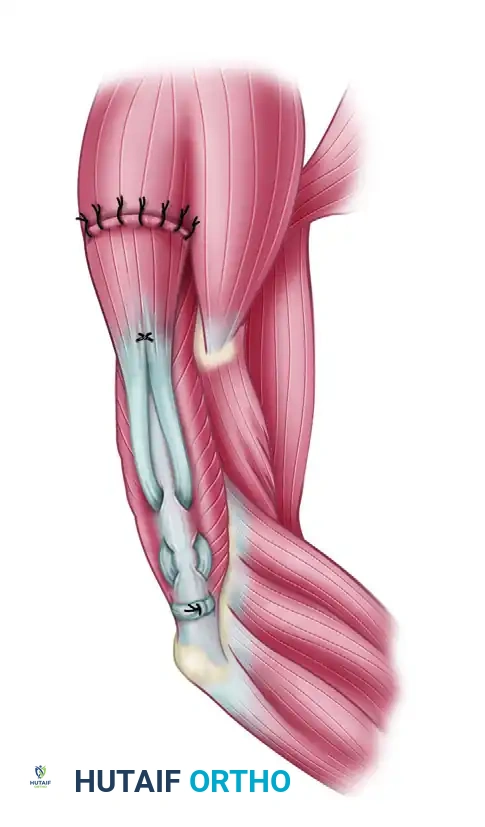
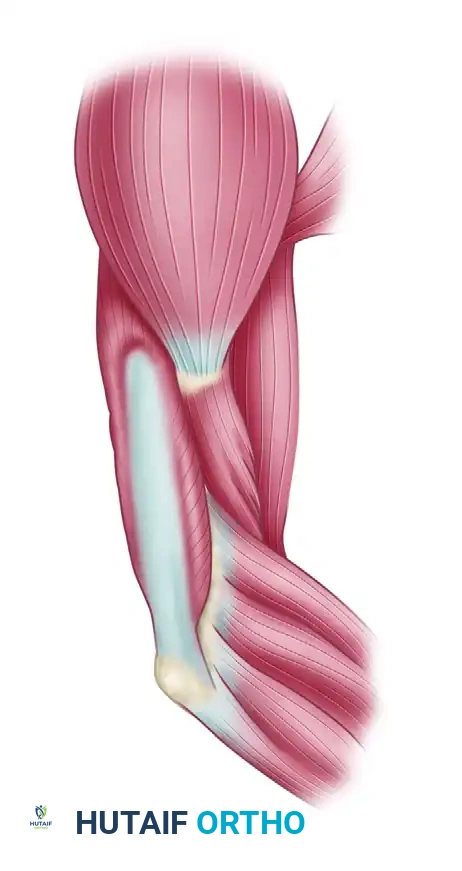
Figure 2: Tendon grafts are laced into the distal end of the posterior deltoid muscle belly proximally and woven into the triceps aponeurosis distally using a Pulvertaft weave technique.
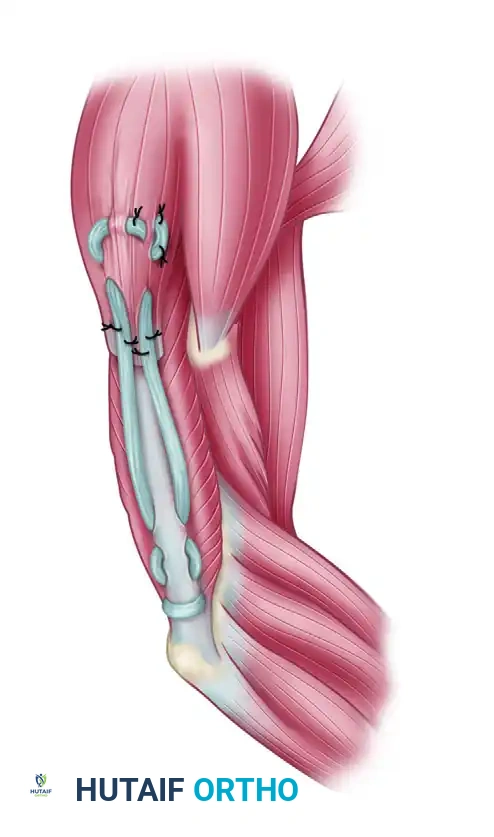
Figure 3: Fascia lata can be used instead of tubular tendon grafts. The broad fascial sheet allows for excellent distribution of tension across the atrophied triceps aponeurosis.
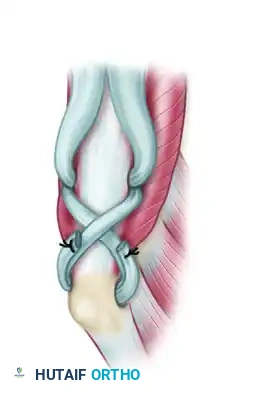
Figure 4: Direct insertion into the olecranon through a transosseous bone tunnel can also be performed with either type of graft, providing rigid bone-to-tendon healing.
Tensioning and Fixation
- The tension of the transfer is paramount. Adjust the tension of the attachment so that full elbow flexion can still be passively obtained on the operating table, but with palpable elastic resistance. Over-tensioning will result in a flexion contracture, while under-tensioning will result in an extensor lag.
- Secure the weave using multiple non-absorbable sutures (e.g., 0 or 2-0 braided polyester).
- Radiographic Markers: Place small stainless steel sutures or surgical clips on either side of the transfer site. This allows the surgeon to radiographically follow the integrity of the attachment postoperatively. If the markers separate on follow-up X-rays, a rupture of the transfer should be suspected.
Adjunctive Procedures: Management of Fixed Supination Deformity
In patients with tetraplegia, the preservation of the biceps (C5) without the opposition of the pronator teres (C6, C7) frequently leads to a fixed supination deformity of the forearm. This severely limits the patient's ability to interact with flat surfaces, use keyboards, or perform feeding activities.
When a fixed supination deformity is present, it must be addressed to maximize the functional utility of the upper extremity. The Zancolli procedure involves the rerouting of the distal end of the biceps and the release of the interosseous membrane.
Biceps Rerouting Technique (Zancolli)
By rerouting the biceps tendon around the radial neck, its biomechanical function is converted from a primary supinator to a pronator, while preserving its function as an elbow flexor.
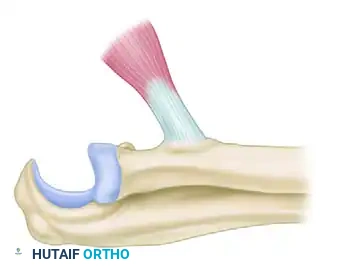
Figure 5: Exposure of the distal biceps tendon at its insertion on the radial tuberosity. The tendon is prepared for detachment.
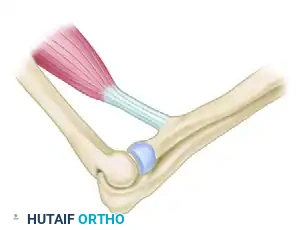
Figure 6: The biceps tendon is detached from the radial tuberosity. Care must be taken to protect the posterior interosseous nerve during deep dissection.
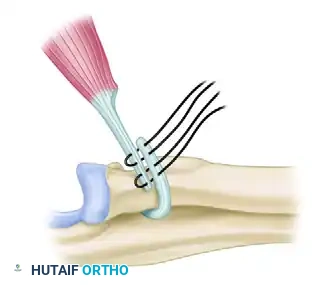
Figure 7: The tendon is rerouted around the radial neck. This alters the vector of pull, converting the muscle into a pronator of the forearm.
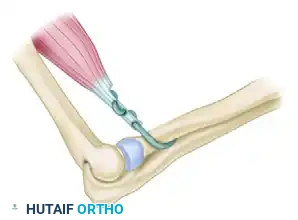
Figure 8: The rerouted biceps tendon is reattached to the radius. Release of the interosseous membrane may be required if severe, chronic contracture prevents passive pronation.
Postoperative Care and Rehabilitation Protocol
The postoperative rehabilitation following a posterior deltoid-to-triceps transfer is rigorous, prolonged, and requires absolute patient compliance. The transferred muscle must heal securely before it can withstand the massive forces required for wheelchair transfers.
Phase I: Immobilization (Weeks 0 to 4)
- Immediately postoperatively, the arm is immobilized in a well-padded long-arm splint or cast.
- The elbow is positioned in 0 to 30 degrees of elbow flexion.
- The shoulder is maintained with the arm adducted to minimize tension on the proximal deltoid dissection.
Phase II: Gradual Mobilization (Weeks 4 to 6)
- At 4 to 6 weeks, the rigid immobilization is removed and replaced with an adjustable hinged elbow brace.
- The elbow is gradually flexed at a strictly controlled rate of 10 to 15 degrees per week.
- This slow progression prevents sudden stretching or rupture of the healing tendon weave.
Phase III: Active Range of Motion (Weeks 6 to 12)
- Once the gradual flexion protocol is complete, active and active-assisted range-of-motion exercises are initiated.
- The patient works on progressive range of motion, focusing on recruiting the posterior deltoid to extend the elbow against gravity.
- Night Splinting: The elbow is maintained in an elbow extension splint at night for a minimum of 3 months to prevent the development of a flexion contracture.
Phase IV: Strengthening and Functional Integration (Months 3 and Beyond)
- Strict Restriction: The patient must absolutely refrain from wheelchair push-ups, independent transfers, and heavy weight-bearing through the operated arm for a minimum of 3 months postoperatively.
- After 3 months, progressive resistance exercises are introduced.
- Functional training with occupational therapy focuses on integrating the new active elbow extension into activities of daily living, reaching, and eventually, safe transfer techniques.
Complications and Pitfalls
- Transfer Rupture: The most devastating complication. Usually occurs due to premature weight-bearing (e.g., an accidental early wheelchair transfer) or overly aggressive passive flexion during rehabilitation. Radiographic markers placed during surgery can confirm rupture.
- Extensor Lag: Caused by under-tensioning the transfer at the time of surgery or stretching of the graft during the healing phase.
- Flexion Contracture: Caused by over-tensioning the transfer or failure to comply with the postoperative night extension splinting protocol.
- Axillary Nerve Injury: Iatrogenic injury during the proximal splitting of the posterior deltoid fibers. This results in catastrophic failure of the transfer and further weakens the shoulder. Strict adherence to identifying the neurovascular hilum is mandatory.
📚 Medical References
- deltoid-to-triceps transfer in quadriplegia, Clin Orthop Relat Res 187:163, 1984.
- Samii K: Transplantation of the clavicular head of the pectoralis major for paralysis of the elbow fl exors, Am Dig Foreign Orthop Lit 61, 1970.
- Seddon HJ: Transplantation of pectoralis major for paralysis of the fl exors of the elbow, Proc R Soc Med 42:837, 1949.
- Segal A, Seddon HJ, Brooks DM: Treatment of paralysis of the fl exors of the elbow, J Bone Joint Surg 41B:44, 1959.
- Spira E: Replacement of biceps brachii by pectoralis minor transplant: report of a case, J Bone Joint Surg 39B:126, 1957.
- Steindler A: Muscle and tendon transplantation at the elbow, Instr Course Lect 2:276, 1944.
- Zancolli EA: Paralytic supination contracture of the forearm, J Bone Joint Surg 49A:1275, 1967.
- Zancolli E, Mitre H:
You Might Also Like