Phalangeal Dislocations of the Foot: Comprehensive Surgical Management
Key Takeaway
Phalangeal dislocations of the foot, particularly at the interphalangeal joint of the hallux, frequently result from hyperextension injuries. While many are amenable to closed reduction, irreducible cases often involve incarceration of the plantar plate or sesamoid bones. This guide details the biomechanical classification, clinical evaluation, and step-by-step surgical techniques required to achieve anatomic reduction and restore forefoot stability in both simple and complex irreducible dislocations.
INTRODUCTION TO PHALANGEAL DISLOCATIONS
Phalangeal dislocations of the foot are relatively uncommon but biomechanically significant injuries that demand precise diagnostic and therapeutic algorithms. These injuries most frequently occur at the interphalangeal (IP) joint of the hallux and the metatarsophalangeal (MTP) or proximal interphalangeal (PIP) joints of the lesser toes. Because the forefoot bears immense dynamic loads during the terminal stance phase of the gait cycle, failure to achieve anatomic reduction and restore ligamentous stability can lead to chronic pain, post-traumatic arthritis, and severe functional impairment.
The primary mechanism of injury is forced hyperextension, which drives the distal phalanx dorsal to the proximal phalanx. This violent vector often results in severe soft tissue compromise, including the tearing of the plantar skin at the interphalangeal joint flexion crease, rendering the dislocation an open fracture-dislocation. While the majority of these injuries can be managed with prompt closed reduction, a critical subset remains irreducible due to the interposition of anatomic structures, most notably the plantar plate or the sesamoid bones.
This comprehensive guide delineates the pathoanatomy, classification, and step-by-step surgical management of phalangeal dislocations, providing orthopedic surgeons with the evidence-based protocols necessary to optimize patient outcomes.
ANATOMY AND BIOMECHANICS OF THE FOREFOOT JOINTS
To understand the obstacles to reduction in phalangeal dislocations, the surgeon must possess an intimate knowledge of the plantar plate and its associated capsuloligamentous structures.
The Plantar Plate
The plantar plate is a thick, fibrocartilaginous structure that forms the floor of the MTP and IP joints. It is firmly attached to the base of the distal phalanx (in the IP joint) or the proximal phalanx (in the MTP joint) and loosely attached to the metatarsal head or proximal phalangeal head via the joint capsule. Its primary biomechanical role is to resist hyperextension. During a severe hyperextension injury, the plantar plate typically avulses from its weaker proximal attachment, allowing the distal bone to translate dorsally. The plate can then become incarcerated within the joint space, acting as an impenetrable barrier to closed reduction.
Collateral Ligaments and Sesamoids
The collateral ligaments (proper and accessory) stabilize the joint against varus and valgus stress. In complete dislocations, at least one collateral ligament—usually the tibial collateral ligament—is ruptured.
In the hallux IP joint, a sesamoid bone is present within the plantar plate in approximately 10% to 15% of the population. When the plantar plate ruptures and becomes interposed in the joint, this sesamoid bone is dragged into the articular space, creating a mechanical block that is clearly visible on radiographs.
Clinical Pearl: The flexor hallucis longus (FHL) tendon can occasionally displace into the joint space during a dislocation; however, it is rarely the primary deterrent to reduction. The primary culprits of irreducibility are almost exclusively the plantar plate and the interphalangeal sesamoid.
INTERPHALANGEAL JOINT DISLOCATIONS OF THE HALLUX
Dislocations of the hallux IP joint are the most frequently encountered phalangeal dislocations in the foot. The clinical presentation is typically dramatic, with the distal phalanx resting in a fixed, hyperextended position dorsal to the proximal phalanx.
Clinical Evaluation
Thorough inspection of the plantar aspect of the hallux is mandatory. The hyperextension force frequently causes a transverse laceration of the plantar skin directly over the IP joint flexion crease. This converts the injury into an open dislocation, necessitating immediate intravenous antibiotics, tetanus prophylaxis, and formal surgical irrigation and debridement.
Neurovascular status must be documented before and after any reduction attempt. The digital nerves and arteries are stretched over the prominent condyles of the proximal phalanx and are at risk for neuropraxia or vascular compromise.
The Miki Classification of Hallux IP Dislocations
Miki et al. identified two distinct types of irreducible interphalangeal dislocations of the hallux based on the position of the plantar plate and the resulting radiographic appearance. Recognizing these types is critical for surgical planning.
Miki Type I (Minimal Deformity)
In a Type I dislocation, the plantar plate ruptures from one or both of its phalangeal attachments (usually proximally) and becomes trapped directly within the joint space.
* Clinical Appearance: The toe may appear relatively straight, and the clinical deformity is minimal, often deceiving the examiner into believing the joint is reduced.
* Radiographic Appearance: The hallmark is marked widening of the interphalangeal joint space without gross dorsal displacement.

Anteroposterior radiograph demonstrating a Miki Type I dislocation with marked widening of the interphalangeal joint space due to an incarcerated plantar plate.

Lateral view of the same Miki Type I injury. Note the wide joint space; the distal phalanx is not grossly hyperextended, which can mask the severity of the incarceration.
Miki Type II (Obvious Deformity)
In a Type II dislocation, the distal phalanx lies completely dorsal to the proximal phalanx, locking the joint in severe hyperextension.
* Clinical Appearance: The deformity is obvious and rigid. The plantar skin is stretched taut or torn.
* Radiographic Appearance: The base of the distal phalanx overlaps the head of the proximal phalanx. If an IP sesamoid is present, it is often visible within the joint space, preventing reduction.
Surgical Warning: A Miki Type I dislocation is a classic "trap" for the unwary surgeon. Because the toe looks clinically aligned, the widened joint space on the radiograph might be dismissed as poor technique or joint effusion. Failure to recognize the incarcerated plantar plate will lead to chronic instability, pain, and early osteoarthritis.
MANAGEMENT STRATEGIES: CLOSED VS. OPEN REDUCTION
Principles of Closed Reduction
Most simple phalangeal dislocations can be reduced closed in the emergency department.
- Anesthesia: A comprehensive digital block using 1% lidocaine or 0.5% bupivacaine (without epinephrine) is administered to ensure complete anesthesia and muscle relaxation.
- Maneuver: The key to successful reduction is avoiding premature flexion, which will only tighten the incarcerated structures.
- First, apply sustained longitudinal axial traction in the line of the deformity (hyperextension) to distract the joint surfaces.
- Second, apply direct dorsal-to-plantar pressure on the base of the distal phalanx.
- Finally, once the base of the distal phalanx clears the condyles of the proximal phalanx, smoothly flex the toe to achieve reduction.
- Post-Reduction Assessment: The joint should be assessed for stability. If the joint is stable and congruent, buddy taping to the adjacent toe for 3 to 4 weeks is sufficient.
Indications for Open Reduction
Open reduction is strictly indicated under the following circumstances:
* Failure of closed reduction after one or two well-executed attempts.
* Open dislocations requiring formal irrigation and debridement.
* Radiographic evidence of joint space widening after a seemingly successful closed reduction (indicating persistent plantar plate or sesamoid interposition).

Post-reduction radiograph showing the interphalangeal joint space remains wider than normal. This is an absolute indication for open reduction.

Further imaging confirming persistent widening and incongruity of the joint space despite closed reduction attempts, necessitating surgical intervention.
SURGICAL TECHNIQUE: OPEN REDUCTION OF THE HALLUX IP JOINT
When the plantar plate or sesamoid is incarcerated, a formal open reduction is required. The dorsal approach is preferred as it provides excellent visualization of the joint space and avoids the weight-bearing plantar surface, minimizing the risk of painful scar formation.
Step 1: Positioning and Preparation
The patient is placed supine on the operating table. A calf or ankle tourniquet is applied to ensure a bloodless surgical field. Intravenous antibiotics are administered, particularly if the injury is open.
Step 2: The Dorsal Approach
- Make a dorsal midline or lazy-S incision centered over the hallux interphalangeal joint.
- Carefully dissect through the subcutaneous tissues, taking care to identify and retract the dorsal cutaneous nerve branches.
- Identify the extensor hallucis longus (EHL) tendon. The EHL can be retracted laterally or medially. In cases of severe swelling or difficult exposure, the EHL tendon can be split longitudinally or Z-lengthened, though simple retraction is usually sufficient.
- Perform a dorsal capsulotomy to expose the joint space.
Step 3: Extricating the Incarcerated Structures
- Inspect the joint. You will typically find the fibrocartilaginous plantar plate (and potentially the sesamoid) draped over the condyles of the proximal phalanx, blocking the reduction of the distal phalanx.
- Use a Freer elevator or a small bone hook to gently tease the plantar plate distally and plantarly, slipping it over the condyles of the proximal phalanx.
- Simultaneously apply longitudinal traction to the distal phalanx.
- Once the plantar plate is extricated from the joint space, the distal phalanx will easily reduce into its anatomic position.
Step 4: Stabilization and Closure
- Assess the stability of the joint. If the collateral ligaments are completely incompetent and the joint is grossly unstable, temporary stabilization with a smooth 0.045-inch or 0.062-inch Kirschner wire (K-wire) driven antegrade across the IP joint is recommended.
- Repair the dorsal capsule with absorbable sutures (e.g., 3-0 Vicryl).
- If the EHL was split or lengthened, repair it meticulously.
- Close the skin with non-absorbable sutures (e.g., 4-0 Nylon).
- If there is a plantar skin tear (open injury), it should be thoroughly irrigated and loosely approximated or left open to heal by secondary intention, depending on the degree of contamination.
LESSER TOE DISLOCATIONS (MTP AND IP JOINTS)
While hallux dislocations command significant attention, lesser toe dislocations present their own unique challenges.
Interphalangeal Joints of the Lesser Toes
Historically, it has been the experience of many surgeons that IP joint dislocations of the lesser toes are easily reducible by closed methods and do well with simple buddy taping for 3 weeks. However, recent literature suggests a more nuanced reality. Some studies report that nearly all dislocated lesser toe IP joints in their cohorts required open reduction due to soft tissue interposition.
When successfully reduced, lesser toe IP joints are virtually asymptomatic at long-term follow-up. Therefore, if closed reduction fails, open reduction via a dorsal approach is highly successful and yields excellent functional results.
Metatarsophalangeal (MTP) Joints of the Lesser Toes
Dislocations of the lesser MTP joints are notoriously difficult to manage. Approximately 30% of dislocated lesser toe MTP joints require open reduction because they are irreducible by closed means.
The primary obstacle is, again, the plantar plate. During a dorsal MTP dislocation, the plantar plate avulses from the metatarsal neck and becomes incarcerated dorsal to the metatarsal head.
* Clinical Consequence: Unlike IP joints, residual subluxations or dislocations at the MTP joints are persistently painful and lead to severe metatarsalgia and crossover toe deformities.
* Surgical Management: Open reduction is mandatory for irreducible MTP dislocations. A dorsal approach is utilized, the deep transverse metatarsal ligament may need to be released, and the plantar plate must be extricated using a Freer elevator. Temporary K-wire fixation across the MTP joint for 3 to 4 weeks is standard practice to maintain alignment while the capsuloligamentous structures heal.
COMPLEX FOREFOOT TRAUMA: ASSOCIATED METATARSAL INJURIES
Phalangeal dislocations rarely occur in isolation during high-energy trauma. Crush injuries to the forefoot frequently result in a combination of phalangeal dislocations and severe metatarsal fractures. The management of the phalangeal dislocation must be integrated into the overall reconstruction of the forefoot cascade.
When faced with a displaced first metatarsal fracture combined with fractures of the lesser metatarsals and associated joint subluxations/dislocations, the surgical priority is to restore the medial column (the first ray) first.

Preoperative anteroposterior radiograph demonstrating a high-energy crush injury with a displaced first metatarsal fracture and comminuted fractures of the second to fourth metatarsals, disrupting the entire forefoot cascade.

Preoperative lateral radiograph of the same injury, highlighting the severe dorsal displacement and instability of the metatarsal segments.
Surgical Reconstruction of the Metatarsal Cascade
- First Ray Stabilization: The first metatarsal is the primary weight-bearing axis of the forefoot. It must be anatomically reduced and rigidly fixed. Open reduction and internal fixation (ORIF) using a low-profile titanium plate and screws is the gold standard.
- Lesser Ray Stabilization: Once the first ray is restored to its anatomic length and rotation, the lesser metatarsals are addressed. Because of the comminution and the need to minimize soft tissue stripping in crush injuries, closed reduction and percutaneous pinning (CRPP) with stout Steinmann pins or K-wires is often preferred over formal plating for the lesser rays.
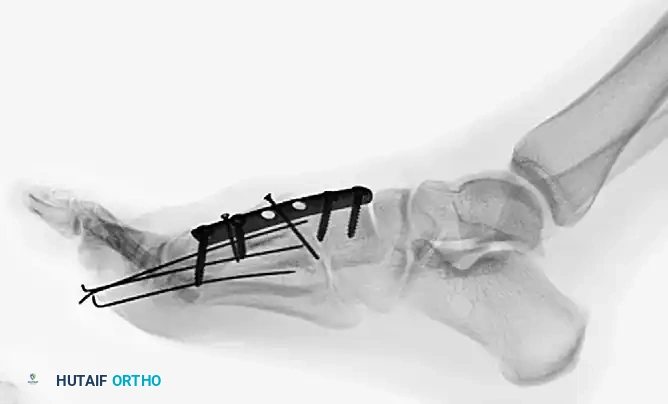
Postoperative anteroposterior radiograph showing anatomic restoration of the forefoot. The first metatarsal has been rigidly stabilized with plate and screw fixation, while the lesser metatarsals have been aligned using percutaneous Steinmann pins.

Postoperative lateral radiograph confirming the restoration of the sagittal alignment of the metatarsals and the reduction of the associated joint spaces.
By restoring the metatarsal parabola, the surgeon re-establishes the tension on the plantar fascia and the intrinsic musculature, which is essential for the subsequent stability of any reduced phalangeal dislocations.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The postoperative management of phalangeal dislocations depends on the stability achieved during surgery and the presence of associated injuries.
- Immobilization: If the joint is stable after open reduction without K-wires, the toe is buddy-taped, and the patient is placed in a rigid-soled postoperative shoe. If K-wires were utilized, the pins are left protruding through the skin and capped.
- Weight-Bearing: Heel-weight-bearing only is permitted for the first 3 to 4 weeks to protect the repair of the plantar plate and collateral ligaments.
- Pin Removal: K-wires are typically removed in the clinic at 3 to 4 weeks postoperatively.
- Physical Therapy: Once pins are removed, aggressive active and passive range-of-motion exercises of the IP and MTP joints are initiated to prevent arthrofibrosis. The plantar plate takes approximately 6 to 8 weeks to heal sufficiently for normal push-off activities.
COMPLICATIONS AND PITFALLS
- Missed Incarceration: The most common pitfall is accepting a "near-anatomic" closed reduction. If the joint space remains widened (Miki Type I), the plantar plate is trapped. Leaving this unaddressed guarantees chronic pain, stiffness, and early degenerative joint disease.
- Arthrofibrosis: The IP and MTP joints are highly prone to stiffness following trauma and surgery. Prolonged immobilization beyond 4 weeks should be strictly avoided unless dictated by concomitant fractures.
- Avascular Necrosis (AVN): While rare, aggressive soft tissue stripping during open reduction can compromise the blood supply to the phalangeal head, leading to AVN. Meticulous, tissue-preserving surgical technique is paramount.
- Infection: Open dislocations with plantar skin tears carry a high risk of deep space infection. Aggressive initial debridement and appropriate antibiotic coverage are non-negotiable.
By adhering to strict radiographic evaluation criteria and maintaining a low threshold for open reduction, the orthopedic surgeon can reliably navigate the complexities of phalangeal dislocations, restoring both the anatomy and the dynamic function of the forefoot.
📚 Medical References
- phalangeal dislocations of the index, middle, ring, and little fi ngers, J Trauma 20:183, 1980.
- McElfresh EC, Dobyns JH, O’Brien ET: Management of fracture-dislocation of the proximal interphalangeal joint, Clin Orthop Relat Res 158:215, 1981.
- Milford L: The hand: fractures and dislocations. In Crenshaw AH, ed: Campbell’s
You Might Also Like
