Percutaneous Epiphysiodesis: A Masterclass in Precise Pediatric Growth Arrest

Key Takeaway
Learn the refined percutaneous epiphysiodesis technique for correcting pediatric limb-length discrepancies. This masterclass covers critical anatomical considerations, meticulous preoperative planning, and precise intraoperative steps for distal femoral, proximal tibial, and fibular growth arrest. Emphasizing fluoroscopic guidance and neurovascular protection, we ensure optimal outcomes while minimizing invasiveness. Postoperative care and complication management are also detailed for comprehensive fellow training.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues, to the operating theater. Today, we are examining the nuances of percutaneous epiphysiodesis, a cornerstone procedure in pediatric orthopaedic surgery for the definitive management of limb-length discrepancies (LLD). This technique, initially reported by Bowen and Johnson in 1984, represents a refined, minimally invasive evolution of the open epiphyseal arrest concept first described by Phemister in 1933 and subsequently modified by White in 1944. The percutaneous approach stands as a testament to how precise, minimally invasive surgical techniques can harness and alter profound biological growth mechanisms with minimal morbidity.
Our overarching objective is mathematically and biologically precise: to permanently inhibit the longitudinal growth of a longer extremity by prematurely arresting a selected physis, thereby allowing the shorter, contralateral limb to "catch up" during the remaining years of skeletal maturation. This intervention is classically indicated for mild to moderate projected discrepancies at skeletal maturity, generally falling between 2.0 to 5.0 centimeters. In this specific cohort, the predictable, uninterrupted growth of the shorter extremity is anticipated to equalize the limb lengths by the time the child reaches Risser stage 5.
Understanding the patho-epidemiology of limb-length discrepancy is critical before any surgical intervention is considered. Discrepancies can arise from a myriad of etiologies, broadly categorized into congenital (e.g., fibular hemimelia, proximal focal femoral deficiency), developmental (e.g., developmental dysplasia of the hip), traumatic (e.g., physeal fractures leading to premature arrest or diaphyseal fractures causing overgrowth), and infectious or neoplastic causes. Shapiro’s seminal work on the different patterns of growth inhibition remains fundamental to our preoperative assessment. By longitudinally tracking a patient, we must ascertain if the growth inhibition is proportional (maintaining a constant ratio of discrepancy) or disproportional (worsening at an accelerating or decelerating rate). This distinction directly impacts the mathematical predictability of our surgical timing and ultimate outcomes.
The clinical significance of untreated limb-length discrepancy extends far beyond cosmesis. Discrepancies exceeding 2.0 centimeters have been biomechanically linked to a multitude of compensatory mechanisms that can lead to long-term pathology. Patients often develop a compensatory pelvic obliquity and functional scoliosis, which, while initially flexible, can become rigid over time. Furthermore, gait biomechanics are significantly altered; the patient must vault over the longer limb or walk with a flexed knee, leading to increased energy expenditure, premature joint degeneration, and chronic lower back pain. By executing a precisely timed epiphysiodesis, we aim to abrogate these compensatory mechanisms and restore symmetrical biomechanical loading to the axial and appendicular skeleton.
Detailed Surgical Anatomy and Biomechanics
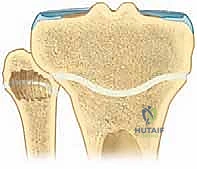
Navigating the surgical landscape of a percutaneous epiphysiodesis demands an intimate, three-dimensional understanding of physeal anatomy and its surrounding neurovascular relationships. The distal femoral and proximal tibial physes are not simple, flat plates; they are highly complex, undulating structures characterized by mammillary processes and distinct topographical variations. The distal femoral physis, in particular, is centrally narrow and peripherally thick, cupping the metaphysis. This anatomical constraint reinforces our preference for a peripheral ablation technique. By targeting the medial and lateral peripheries, we respect the central anatomy, allowing a spontaneous central closure to follow the peripheral tethering.
Posteriorly, the neurovascular structures present the most significant hazard during this procedure. At the level of the distal femur, the popliteal artery and vein, along with the tibial nerve, are deeply positioned within the intercondylar notch, lying directly posterior to the central aspect of the physis. In the proximal tibia, the popliteal trifurcation and the tibial nerve are similarly vulnerable just posterior to the posterior cortex. A catastrophic plunge with a curette or drill in the central or posterior-central zones can result in devastating vascular injury or limb-threatening compartment syndrome. Therefore, our instrumentation must always be directed with meticulous fluoroscopic guidance, strictly maintaining a trajectory within the peripheral anterior and mid-coronal planes.
The proximal fibula presents a unique and critical neurovascular risk that demands specific attention: the common peroneal nerve. This nerve courses obliquely along the lateral aspect of the popliteal fossa, tracking close to the medial border of the biceps femoris tendon and the lateral head of the gastrocnemius. It then winds superficially and posteriorly around the neck of the proximal fibula, passing deep to the peroneus longus muscle before bifurcating. Because of its intimate tethering to the fibular neck, the nerve is highly susceptible to direct iatrogenic transection, traction injury from aggressive retraction, or thermal necrosis if high-speed burrs are utilized improperly.
Biomechanically, percutaneous epiphysiodesis relies on the Hueter-Volkmann principle, which dictates that increased compressive forces across a growth plate will inhibit longitudinal growth. By surgically ablating the medial and lateral peripheral margins of the physis, we induce localized hematoma and subsequent osteogenesis. As these peripheral areas heal, they form robust, unyielding bony bridges (physeal bars) between the epiphysis and the metaphysis. Once these peripheral tethers are established, the continued biological drive for central physeal expansion is met with immense mechanical resistance. This generates massive compressive forces across the remaining central physis, rapidly leading to its spontaneous, premature closure within 6 to 8 months.
Exhaustive Indications and Contraindications
Patient selection is the crucible in which the success or failure of an epiphysiodesis is determined. The primary indication for this procedure is a projected limb-length discrepancy at skeletal maturity of between 2.0 and 5.0 centimeters. Discrepancies of this magnitude are sufficient to cause the aforementioned biomechanical and kinematic derangements, justifying surgical intervention. However, the exact timing of the surgery is dictated not by chronologic age, but entirely by skeletal bone age and the calculated remaining growth potential. We rely heavily on the Greulich and Pyle method, utilizing left hand and wrist radiographs, to ascertain the true biological maturity of the patient.
A critical nuance in our indications involves the etiology of the discrepancy. Patients with congenital anomalies (e.g., hemihypertrophy) or those who have sustained an asymmetric physeal injury require particularly vigilant monitoring. The predictable growth charts (such as the Green-Anderson data) are based on normal growth patterns. If the shorter limb has an intrinsic growth defect, its future growth may not parallel standard predictive charts, potentially leading to significant undercorrection if not accounted for. Therefore, a documented, historical trajectory of the discrepancy—ideally plotted over several years using the Mosley straight-line graph—is a prerequisite for accurate surgical timing.
Contraindications to percutaneous epiphysiodesis must be rigorously respected to avoid suboptimal outcomes or the creation of iatrogenic deformity. The most absolute contraindication is a projected discrepancy at maturity of greater than 5.0 centimeters. In such cases, arresting the longer limb sufficiently to achieve equality would result in unacceptable disproportion of the patient's overall height, leading to a "short-stature" phenotype that is cosmetically and functionally undesirable. For these severe discrepancies, limb lengthening procedures (e.g., utilizing intramedullary lengthening nails or external fixators) of the shorter extremity are the standard of care.
Furthermore, percutaneous epiphysiodesis is contraindicated in the presence of severe angular deformities that require simultaneous correction. While a precisely asymmetric epiphysiodesis (hemiepiphysiodesis) can correct mild angular deformities, severe varus or valgus malalignments associated with LLD are better managed with guided growth utilizing tension band plates or acute corrective osteotomies. Additionally, inadequate remaining growth potential (e.g., a bone age of >14 in girls or >16 in boys) renders the procedure futile, as the physis is already nearing natural senescence and insufficient growth remains in the contralateral limb to achieve equalization.
| Category | Specific Criteria / Conditions | Clinical Rationale |
|---|---|---|
| Absolute Indications | Projected LLD at maturity of 2.0 - 5.0 cm | Biomechanical threshold where compensatory mechanisms fail, yet overall height disproportion is avoided. |
| Relative Indications | Projected LLD of 1.5 - 2.0 cm in highly symptomatic athletes | May prevent chronic stress injuries in high-demand populations, though non-operative management is usually preferred. |
| Absolute Contraindications | Projected LLD > 5.0 cm | Epiphysiodesis would cause unacceptable overall short stature; limb lengthening is required. |
| Absolute Contraindications | Skeletal maturity (Bone age >14 F, >16 M) | Insufficient remaining growth in the shorter limb to achieve equalization. |
| Relative Contraindications | Severe concurrent angular deformity | Requires more powerful corrective techniques (osteotomy or tension band plating) rather than simple ablation. |
Pre-Operative Planning, Templating, and Patient Positioning
Before the patient enters the operating room, an exhaustive preoperative planning phase must be completed. This is not merely an administrative step; it is the mathematical foundation of the procedure. Our assessment begins with a comprehensive physical examination, focusing on anthropometric measurements. We measure total height and bilateral leg lengths, but crucially, we also assess functional discrepancy using calibrated blocks. By placing blocks of differing thicknesses under the shorter limb until the pelvis is clinically level (assessed by palpating the anterior superior iliac spines), we obtain a functional measurement that accounts for pelvic asymmetries and foot height discrepancies, which standard long-leg radiographs may miss.
Radiographic templating relies on high-quality, standing full-length lower extremity scanograms or orthoroentgenograms. Using a calibrated magnification marker, precise measurements of the femur and tibia are obtained. We then employ multiple predictive methods to cross-verify our surgical timing. The Green-Anderson growth remaining charts are our primary tool, plotting the lengths against the patient's Greulich-Pyle bone age. We supplement this with the Multiplier Method for its rapid clinical utility, and the Mosley straight-line graph, which is exceptional for visualizing the historical trend of the discrepancy. Discrepancies between chronologic age, Tanner staging, and bone age warrant extreme caution; if the bone age is significantly advanced or delayed relative to chronologic age, the predictive charts become less reliable, and serial observation may be necessary before committing to surgery.
Once the precise timing is confirmed and the target physes (distal femur, proximal tibia, or both) are selected, we transition to operating theater setup. The patient is placed in the supine position on a fully radiolucent operating table. This is non-negotiable, as unimpeded fluoroscopic access is the linchpin of percutaneous safety. The C-arm image intensifier must be positioned such that perfect anteroposterior (AP) and lateral views of the target joints can be obtained seamlessly, without requiring the surgical team to lift or torque the patient's leg, which could distort our spatial orientation.
The entire limb, from the toes to the proximal thigh, is meticulously prepped and draped into a sterile field. This wide exposure is critical; it allows the surgeon to visually assess the mechanical axis of the limb during the procedure and provides access should an open conversion be required. A pneumatic tourniquet is placed high on the proximal thigh. However, in our masterclass approach, the tourniquet is strictly uninflated during the procedure. Operating without a tourniquet allows for continuous assessment of normal tissue perfusion, minimizes the risk of ischemic nerve injury (particularly to the peroneal nerve), and ensures that any unexpected arterial bleeding is immediately recognized and addressed, rather than being masked until tourniquet deflation.
Step-by-Step Surgical Approach and Fixation Technique
The intraoperative execution of a percutaneous epiphysiodesis requires a delicate balance of tactile feedback and radiographic vigilance. I strongly advocate for the use of manual curettes over motorized drills or burrs. Motorized instruments can easily deviate, plunge through the posterior cortex, or generate thermal necrosis that extends unpredictably beyond the intended ablation zone. A curette, conversely, provides the surgeon with immediate, nuanced tactile feedback—the distinct "crunch" of physeal cartilage versus the rigid, unyielding scrape of the metaphyseal bone.
Physeal Identification and Incision
We begin by precisely localizing the physis under fluoroscopy. Using a metal marker, such as a K-wire or a hemostat, we identify the exact level of the physis at its peripheral margin on the AP view.
Localization of the distal femoral physis using a metal pointer under fluoroscopic guidance.
Once the level is confirmed, a precise 3-mm longitudinal stab incision is made directly over the medial and lateral peripheral physeal plates using a #15 blade. This minimal incision is the hallmark of the percutaneous technique, drastically reducing postoperative pain and scarring.

A precise 3-mm longitudinal skin incision is made over the targeted physis.
Periosteal and Physeal Penetration
Through this 3-mm incision, a 3-mm-wide straight osteotome is introduced. We carefully navigate through the subcutaneous tissue, avoiding major muscular intervals, until we palpate the periosteum. Under continuous AP and lateral fluoroscopic guidance, the osteotome is advanced to create a longitudinal split in the periosteum and the underlying cortex, directly in line with the physis.

Advancement of the 3-mm osteotome to split the periosteum and cortex.
The osteotome is gently tapped to penetrate the physeal plate to a depth of approximately 0.5 cm. It is imperative to confirm this depth on the lateral fluoroscopic view to ensure we are not violating the posterior cortex.

Fluoroscopic confirmation of the osteotome depth, ensuring it remains within the anterior and middle thirds of the physis.
Physeal Ablation via Curettage
Following the creation of the cortical window, the osteotome is withdrawn, and a small, angled curette is introduced into the physeal track.

Insertion of the angled curette into the physeal track.
The ablation process involves a systematic, sweeping motion. We direct the curette anteriorly, posteriorly, and centrally, meticulously scraping away the cartilaginous physeal tissue until the gritty texture of the adjacent epiphyseal and metaphyseal bone is felt.
Systematic sweeping motions with the curette to ablate the peripheral physis.

Continuous fluoroscopic monitoring during curettage to ensure instruments remain within the safe zones.
This process is repeated through both the medial and lateral incisions. Our goal is to destroy approximately the peripheral 10% to 15% of the physis on each side, creating a sufficient void for the subsequent formation of a robust bony bar.

Completion of the peripheral ablation, ensuring adequate destruction of the cartilaginous plate.
Proximal Fibular Technique
If a proximal tibial epiphysiodesis is performed, the proximal fibular physis must also be arrested to prevent progressive fibular overgrowth, which can lead to lateral knee pain, proximal tibiofibular joint subluxation, and ankle mortise distortion. Because of the common peroneal nerve, our approach here is highly specific.

Localization and approach to the proximal fibular physis, carefully avoiding the posterior neurovascular structures.
We make our incision strictly over the anterosuperior aspect of the fibular head. The curette is directed inferiorly and medially into the physis, deliberately working away from the posterior and lateral course of the peroneal nerve.

Curettage of the proximal fibula, directing instruments anterosuperiorly to inferiorly.
Once the ablation is complete across all targeted physes, the wounds are thoroughly irrigated to remove cartilaginous debris. The small incisions are closed with simple interrupted sutures or skin adhesive, and a sterile dressing is applied.
Closure of the 3-mm stab incisions.

Application of sterile dressings.

Final clinical appearance of the limb post-procedure, demonstrating minimal soft tissue disruption.
Complications, Incidence Rates, and Salvage Management
While percutaneous epiphysiodesis is generally considered a safe and highly effective procedure, complications can and do occur, primarily stemming from errors in surgical timing or technical execution. The most common complication is undercorrection or overcorrection of the limb-length discrepancy. Undercorrection typically results from intervening too late in the patient's skeletal development, leaving insufficient growth in the shorter limb to catch up. Overcorrection occurs when the surgery is performed too early. Salvage for these timing errors may require a contralateral epiphysiodesis (if overcorrected and the patient is still growing) or eventual limb lengthening/shortening procedures at skeletal maturity.
A more insidious technical complication is the development of an iatrogenic angular deformity (genu valgum, genu varum, or recurvatum). This occurs due to asymmetric ablation of the physis. For instance, if the medial physis is adequately ablated but the lateral physis is insufficiently destroyed, the lateral side will continue to grow, driving the knee into progressive valgus. Similarly, failure to ablate the anterior physis adequately can lead to a recurvatum deformity. The incidence of angular deformity is reported to be between 2% and 10%. Salvage management requires vigilant postoperative monitoring; if an angular deformity is detected early, completion of the failed epiphysiodesis may suffice. If the deformity becomes clinically significant, corrective osteotomies or guided growth procedures at the end of skeletal maturity will be necessary.
Neurovascular injury is the most devastating potential complication. As previously detailed, the popliteal vessels and the common peroneal nerve are at highest risk. Plunging through the posterior cortex of the femur or tibia can result in arterial laceration or pseudoaneurysm formation. Injury to the common peroneal nerve during fibular epiphysiodesis can result in a permanent foot drop. The incidence of neurovascular injury is exceedingly low (<1%) when strict fluoroscopic guidance and proper anatomical approaches are utilized, but the catastrophic nature of this complication demands absolute respect for the posterior anatomy.
Infection and hematoma formation are rare due to the percutaneous nature of the procedure, occurring in less than 1% of cases. Joint penetration is another technical error, usually occurring if the entry point is too proximal on the femur or too distal on the tibia, violating the articular cartilage. This can lead to premature osteoarthritis and chronic effusion. Strict adherence to fluoroscopic landmarks prevents this complication.
| Complication | Estimated Incidence | Pathophysiology / Cause | Salvage / Management Strategy |
|---|---|---|---|
| Undercorrection | 5% - 15% | Surgery performed too late (advanced bone age). | Shoe lifts; limb lengthening at maturity if severe. |
| Overcorrection | 2% - 5% | Surgery performed too early. | Contralateral epiphysiodesis; limb shortening at maturity. |
| Angular Deformity | 2% - 10% | Asymmetric or incomplete physeal ablation. | Repeat ablation if caught early; corrective osteotomy at maturity. |
| Peroneal Nerve Palsy | < 1% | Direct trauma or thermal injury during fibular ablation. | Immediate exploration if transected; AFO bracing and observation for neuropraxia. |
| Joint Penetration | < 1% | Incorrect trajectory violating articular cartilage. | Arthroscopic debridement if symptomatic; long-term monitoring for OA. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following a percutaneous epiphysiodesis is remarkably accelerated compared to open procedures or limb lengthening, reflecting the minimally invasive nature of the surgery. The immediate postoperative phase (0 to 2 weeks) focuses on pain control, reduction of swelling, and the prevention of deep vein thrombosis. Patients are typically discharged on the day of surgery or after a 23-hour observation period. We permit immediate weight-bearing as tolerated with the assistance of crutches. A soft, bulky dressing is applied, and the use of a knee immobilizer is generally unnecessary unless the patient experiences significant quadriceps inhibition due to pain.
During the intermediate phase (2 to 6 weeks), the primary goal is the complete restoration of knee range of motion and normal gait mechanics. Patients are encouraged to transition off crutches as their comfort allows, usually within the first two weeks. Physical therapy may be prescribed if the patient exhibits a persistent limp or struggles to regain full terminal extension or deep flexion. Because the structural integrity of the metaphysis and epiphysis is largely preserved, there are no strict range of motion restrictions.
The long-term monitoring phase (6 months to skeletal maturity) is the most critical aspect of the postoperative protocol. The success of the procedure cannot be judged immediately. Patients must return for serial clinical evaluations and standing scanograms every 6 to 12 months until they reach skeletal maturity (Risser 5). The first postoperative radiograph at 6 months should demonstrate the formation of central bony bridges, confirming the successful arrest of the physis.
Return to competitive sports and high-impact activities is typically permitted once the patient has achieved full, painless range of motion, normal symmetric strength, and a normalized gait pattern, which usually occurs between 6 to 8 weeks postoperatively. However, the surgeon must counsel the family that the limb-length discrepancy will not resolve immediately; rather, the shorter limb will gradually catch up over the ensuing years of growth. Continuous monitoring ensures that any developing angular deformities or timing miscalculations are identified and addressed promptly.
Summary of Landmark Literature and Clinical Guidelines
The evolution of epiphysiodesis is a fascinating journey through the history of pediatric orthopaedics, underpinned by several landmark publications that have shaped our current clinical guidelines. The foundational concept of surgically arresting a physis to manage LLD was introduced by Phemister in 1933. His open technique involved excising a rectangular block of bone encompassing the physis, rotating it 180 degrees, and reinserting it to create a bony tether. While effective, this procedure required large incisions, extensive periosteal stripping, and carried a significant risk of morbidity and prolonged rehabilitation.
In 1944, White modified Phemister's technique by utilizing a square bone graft and adding a mortise and tenon configuration, which improved the mechanical stability of the graft but still required a morbid open approach. The true paradigm shift occurred in 1984 when Bowen and Johnson published their seminal paper detailing the percutaneous technique. By utilizing fluoroscopy and curettage through minimal stab incisions, they demonstrated that profound biological growth arrest could be achieved with drastically reduced surgical trauma, shorter hospital stays, and excellent cosmetic outcomes. Their work remains the bedrock of the modern masterclass technique we employ today.
Subsequent
