Percutaneous Osteotomies & Fassier-Duval Telescoping Nailing for OI Long Bone Deformity

Key Takeaway
This masterclass details percutaneous osteotomies and Fassier-Duval telescoping nailing for long bone deformities in osteogenesis imperfecta. We cover comprehensive surgical anatomy, meticulous preoperative planning, and granular intraoperative execution from a surgeon's perspective. Learn critical pearls, pitfalls, and postoperative management to optimize outcomes for these fragile patients, minimizing morbidity and enhancing function.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues, to this definitive exploration of the surgical management of long bone deformities in Osteogenesis Imperfecta (OI). Today, we are analyzing a highly complex yet profoundly rewarding procedure: multiple percutaneous osteotomies combined with Fassier-Duval (FD) telescoping intramedullary nailing. This technique represents a monumental paradigm shift in pediatric orthopedic surgery. By transitioning from the traditional, highly morbid open Sofield-Millar fragmentation techniques to a minimally invasive percutaneous approach, we offer these vulnerable patients improved comfort, vastly superior functional outcomes, and considerably lower perioperative morbidity. Our fundamental objective is to correct multiplanar deformities, restore mechanical axial alignment, and meticulously preserve the soft tissue envelope, thereby facilitating immediate mobilization and mitigating the devastating cycle of disuse osteopenia.
Osteogenesis Imperfecta is a phenotypically diverse and complex genetic disorder, primarily characterized by profound bone fragility, osteopenia, and recurrent fractures. The vast majority of cases (approximately 85-90%) stem from autosomal dominant mutations in the COL1A1 or COL1A2 genes, which encode the chains of type I procollagen. These mutations result in either a quantitative deficiency of structurally normal collagen (often seen in milder forms like Sillence Type I) or a qualitative defect where abnormal collagen is incorporated into the extracellular matrix, leading to severe structural compromise (Sillence Types II, III, and IV). However, the modern orthopedic surgeon must recognize that the genetic landscape of brittle bone diseases is expanding, with numerous recessive mutations affecting collagen folding, post-translational modification, and osteoblast function now identified.
Historically, the natural history of severe OI was grim. Infants with Sillence type II often faced early perinatal mortality due to pulmonary hypoplasia and severe rib fractures. Children with types III and IV endured severe, progressive disability driven by unrelenting recurrent fractures, chronic intractable bone pain, and grotesque skeletal deformities. Prior to the widespread implementation of intravenous bisphosphonate therapy, independent ambulation—and frequently even comfortable upright sitting—were unattainable goals for many of these children. Even in phenotypically milder forms, patients endure numerous significant fractures throughout childhood, which severely impact their psychosocial development, functional independence, and overall quality of life.

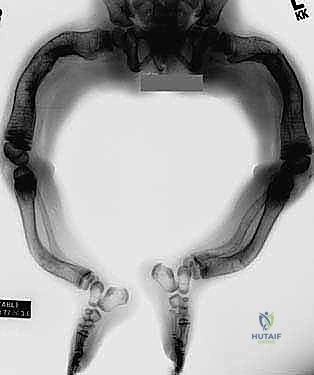
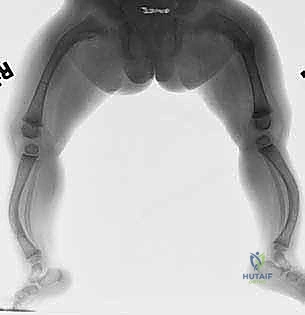
The defining clinical characteristics include a relentless cycle of recurrent fractures leading to progressive multiplanar deformity. In the lower extremities, this most commonly manifests as severe anterolateral bowing of the femurs and anterior bowing (procurvatum) of the tibias. This bowing is not merely a result of fracture malunion; it is a dynamic, progressive process accentuated by the persistent, unopposed pull of strong flexor muscle groups across structurally compromised, osteopenic bone. Furthermore, we frequently observe secondary spinal manifestations, including scoliosis, vertebral compression (flexion) fractures leading to progressive kyphosis, and a high incidence of spondylolysis and spondylolisthesis in ambulatory patients. Craniocervical abnormalities, such as basilar invagination, require vigilant monitoring, as their progression does not necessarily correlate with the overall severity of the peripheral skeletal disease.
While classic extraskeletal physical findings—such as blue sclerae, dentinogenesis imperfecta, triangular facies, and profound ligamentous laxity—are highly suggestive of the diagnosis, their absence absolutely does not preclude a diagnosis of OI. The severity of the intrinsic bone disease, the annualized fracture incidence, the magnitude of the deformity, and the patient's functional baseline are the paramount metrics guiding our surgical decision-making. We must also rigorously rule out differential diagnoses, including non-accidental trauma (child abuse), metabolic bone diseases (such as hypophosphatasia and severe rickets), and idiopathic juvenile osteoporosis.
Detailed Surgical Anatomy and Biomechanics
The surgical anatomy of the OI femur and tibia presents a unique set of biomechanical challenges that dictate our operative approach. Unlike the predictable anatomy of normal pediatric long bones, the OI long bone is characterized by extreme cortical thinning, a lack of distinct corticomedullary differentiation, and profound geometric distortion. The femur typically develops a severe anterolateral bow, often with the apex located in the proximal or middle third. As this bowing progresses, the mechanical axis deviates significantly from the anatomic axis, creating massive bending moments across the diaphysis during weight-bearing or even resting muscle contraction. This "cane-like" deformity exponentially increases the risk of catastrophic fracture at the apex of the curve.
Compounding the gross deformity is the internal architecture of the OI bone. The medullary canal is frequently obliterated by dense, sclerotic bone at the apex of the deformity—a physiological response to chronic micro-fracturing and altered stress shielding. This sclerosis poses a formidable obstacle during intramedullary reaming and guidewire passage. Furthermore, the proximal femur frequently develops severe coxa vara, driven by the mechanical disadvantage of the abductor musculature acting on a weakened femoral neck. This necessitates careful evaluation of the neck-shaft angle, as concomitant valgus producing osteotomies may be required to restore abductor mechanics and prevent femoral neck fractures.
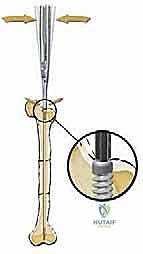
The biomechanical rationale for telescoping intramedullary nailing is rooted in the concept of load-sharing rather than stress-shielding. Rigid, large-diameter adult nails are strictly contraindicated in the growing OI patient. A rigid implant in osteopenic bone creates massive stress risers at the proximal and distal extents of the implant, predictably leading to peri-implant fractures. Furthermore, rigid nails cause profound stress shielding, resulting in the phenomenon of "disappearing bone," where the diaphysis resorbs entirely around the stiff implant. The Fassier-Duval nail, utilizing a smaller diameter, flexible, male-female telescoping design, allows the implant to share mechanical loads with the host bone, stimulating cortical hypertrophy while simultaneously accommodating longitudinal physeal growth.
The deforming forces acting upon these bones must be neutralized intraoperatively. The hamstrings, gastrocnemius-soleus complex, and iliopsoas exert continuous bending moments. When performing percutaneous osteotomies, the surgeon must ensure that the bone is completely sectioned and that these soft tissue tethers are adequately overcome to allow for tension-free realignment over the intramedullary nail. Failure to fully release or realign the bone against these muscle forces will result in immediate hardware failure, nail bending, or delayed union at the osteotomy site. The goal is to convert bending forces into compressive forces along the axis of the intramedullary device.
Exhaustive Indications and Contraindications
The landscape of OI management has been revolutionized by early diagnosis and the aggressive initiation of intravenous bisphosphonate therapy (e.g., pamidronate, zoledronic acid). These antiresorptive agents significantly increase bone mineral density, reduce the incidence of atraumatic fractures, and alleviate chronic bone pain. Crucially, this medical optimization has made surgical intervention feasible in a population where extreme bone fragility previously precluded stable internal fixation. However, bisphosphonates do not remodel existing deformities. Therefore, the primary surgical indications remain unyielding: recurrent fractures, intractable pain, and progressive deformity that critically impairs comfort, joint motion, and functional ambulation.



Surgical intervention should be timed optimally to coincide with the child's developmental milestones, specifically when they begin attempting to pull to a stand or crawl. There is absolutely no biomechanical or physiological advantage to delaying surgery until the child is older. Residual bowing will never correct with growth; in fact, the deformity will predictably worsen, leading to further fractures and the development of fixed secondary joint contractures. The objective is to correct as many involved, symptomatic long bones in a single anesthetic setting as can be safely tolerated by the patient, thereby minimizing repeated hospitalizations and psychological trauma.
Contraindications must be strictly observed to prevent catastrophic outcomes. Absolute contraindications include active osteomyelitis or systemic infection, severe cardiopulmonary instability precluding prolonged anesthesia, and an absolute lack of a definable medullary canal that cannot be negotiated even with the finest specialized reamers. Relative contraindications include extreme youth (typically under 18 months of age), as the epiphyses may be too small to adequately anchor the threads of the Fassier-Duval nail without violating the articular surface or causing physeal arrest. However, in cases of severe, life-altering deformity, custom-modified implants or off-label use of smaller devices may be considered by highly experienced surgeons.
Forearm fixation carries a distinct set of indications and a notably higher complication profile. Due to the complex interplay of pronation and supination, the narrow medullary canals of the radius and ulna, and the high risk of cross-union or hardware migration, forearm nailing is generally reserved for cases of severe functional impairment or recurrent fractures that fail conservative management. Furthermore, existing intramedullary nails—even if they are no longer telescoping—should not be electively removed unless they are symptomatic, migrating, or causing an impending fracture, as the removal process itself frequently induces new fractures in the fragile cortical shell.
| Category | Specific Criteria |
|---|---|
| Primary Indications | Recurrent fractures (≥2 in the same long bone within 6 months). |
| Progressive diaphyseal bowing (anterolateral femur, anterior tibia) > 20 degrees. | |
| Chronic, unremitting bone pain at the apex of a deformity. | |
| Deformity preventing independent ambulation, standing, or orthotic fitting. | |
| Absolute Contraindications | Active local or systemic infection. |
| Unstable cardiopulmonary status precluding general anesthesia. | |
| Complete obliteration of the medullary canal unamenable to specialized reaming. | |
| Relative Contraindications | Age < 18 months (epiphyses may be too small to anchor FD nail threads). |
| Severe, untreated malnutrition or vitamin D deficiency (requires pre-op optimization). | |
| Forearm deformity without significant functional impairment (due to high complication rates). |
Pre-Operative Planning, Templating, and Patient Positioning
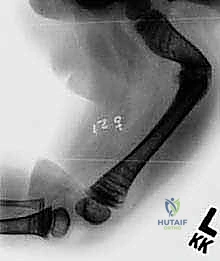
Meticulous preoperative planning is the absolute cornerstone of a successful surgical outcome in the OI patient. We are operating on highly fragile bone with complex, multiplanar, and often multi-apical deformities. The margin for error is virtually non-existent. Our primary diagnostic modality remains high-quality plain radiography. Full-length, standing (or supine traction) radiographs of both lower extremities, capturing the hips to the ankles on a single cassette, are mandatory. These images allow us to assess the entire mechanical axis, locate existing fracture sites, and precisely quantify the degree and location of the deformities.
Crucially, standard AP and lateral views are insufficient. We must obtain views with the patellae oriented directly anteriorly, followed by views with the lower extremities in maximum external rotation. Because the bowing in OI is typically anterolateral, a standard AP radiograph often underestimates the true magnitude of the deformity. The maximum external rotation view provides a true orthogonal projection of the maximum bowing plane, which is invaluable for predicting fracture risk and planning the exact levels of the percutaneous osteotomies. Standard PA and lateral spine radiographs are also required to evaluate for concomitant scoliosis or spondylolisthesis, which may impact patient positioning and anesthesia.
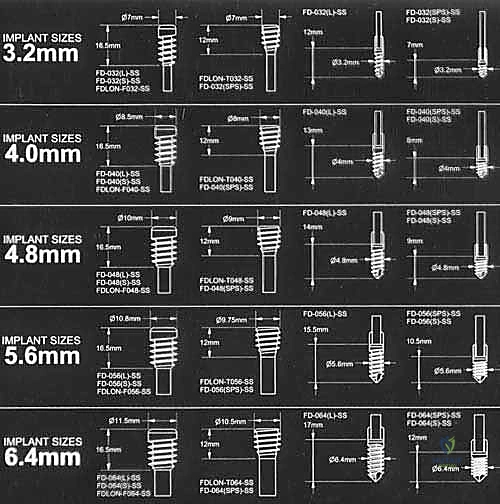
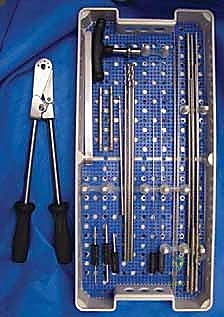
Templating is a non-negotiable step. Using both digital orthopedic templating software and physical overlay templates, the surgeon must preoperatively determine the estimated length and diameter of both the male and female components of the Fassier-Duval nail. The goal is to select a nail diameter that fills the narrowest portion of the isthmus without requiring excessive reaming, which could thin the already fragile cortices to the point of structural failure. The surgeon must ensure that every appropriate size, length, and type of device—including backup non-telescoping flexible nails (e.g., Nancy nails or Rush pins)—is available in the operating room prior to induction.
Patient positioning requires extreme care. The patient should be placed supine on a completely radiolucent Jackson table or a flat fluoroscopy table to allow for unhindered C-arm access from the hip to the ankle. For femoral nailing, a small radiolucent bump is placed under the ipsilateral hemipelvis to internally rotate the leg and present the greater trochanter. The entire lower extremity must be prepped and draped free to allow for intraoperative traction, manipulation, and continuous assessment of rotational alignment. The anesthesia team must be experienced with OI, utilizing careful intubation techniques to avoid cervical spine hyperextension and avoiding succinylcholine due to the risk of fasciculation-induced fractures.
Step-by-Step Surgical Approach and Fixation Technique
The execution of multiple percutaneous osteotomies and Fassier-Duval nailing demands exceptional spatial awareness, fluoroscopic proficiency, and a delicate touch. The overarching principle is to achieve axial realignment with minimal disruption to the periosteal blood supply, thereby promoting rapid callus formation and early consolidation.
Femoral Osteotomy and Female Component Insertion
The procedure begins with the identification of the Center of Rotation of Angulation (CORA) using live fluoroscopy. Small, 1-2 cm stab incisions are made directly over the planned osteotomy sites. Rather than using an oscillating saw, which generates thermal necrosis and destroys the periosteum, we utilize a multiple-drill-hole technique. A sharp drill bit or a fine osteotome is used to perforate the cortex circumferentially at the apex of the deformity. Once the bone is adequately weakened, a manual, controlled osteoclasis is performed. This "greensticking" of the bone preserves the periosteal hinge on the concave side, maintaining critical vascularity.




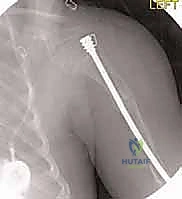
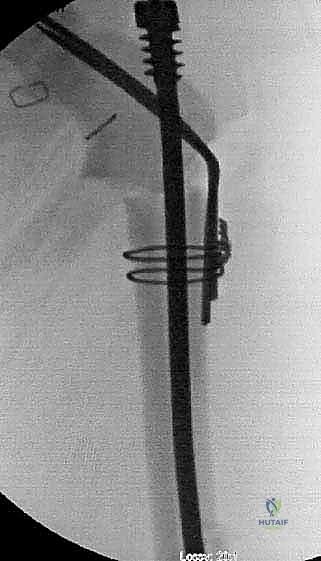
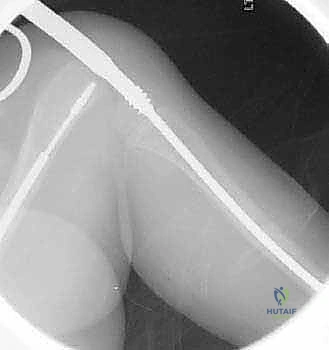
Following the osteotomies, a rigid, olive-tipped guidewire is introduced percutaneously. The entry point for the femur is typically the tip of the greater trochanter, avoiding the piriformis fossa to mitigate the risk of avascular necrosis of the femoral head. The guidewire is carefully negotiated down the medullary canal, crossing each osteotomy site. The surgeon must manually align the bone segments to allow passage. Once the guidewire reaches the distal femoral physis, sequential flexible reaming is performed. Reaming must be done meticulously, utilizing power only when advancing and never when withdrawing, to prevent the reamer from binding and shattering the diaphysis.





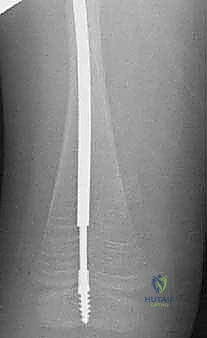
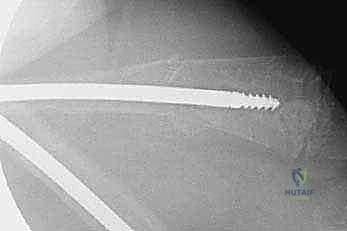
The female component of the FD nail is then introduced over the guidewire. It is advanced until the proximal threaded portion is securely embedded within the greater trochanteric apophysis. It is critical that the distal end of the female component resides proximal to the distal femoral physis to allow for unhindered longitudinal growth. Fluoroscopy is used in both AP and lateral planes to confirm that the female component is centrally located within the canal and that all osteotomy sites are appropriately aligned without residual translation or angulation.
Tibial Osteotomy and Male Component Insertion
Addressing the tibia often requires multiple osteotomies to correct the classic "saber shin" procurvatum deformity. The approach is percutaneous, utilizing stab incisions over the anterior tibial crest. The entry point for the tibial nail is trans-patellar tendon or paratendinous, entering the proximal tibia just distal to the apophysis to avoid recurvatum deformity from premature physeal closure.



Similar to the femur, a guidewire is passed across the osteotomy sites, and sequential reaming is performed. The male component of the FD nail is then introduced. In the femur, the male component is typically passed antegrade through the female component. In the tibia, depending on the specific iteration of the implant being used, it may be passed antegrade or retrograde. The critical step is the distal anchoring. The threaded tip of the male component must be securely driven into the distal epiphysis. The surgeon must utilize precise fluoroscopic guidance to ensure the threads cross the physis and purchase the epiphyseal bone without penetrating the articular surface of the knee or ankle joint.