Comprehensive Introduction and Patho-Epidemiology
Partial resection of the lateral condyle of the fifth metatarsal head, universally recognized in orthopedic nomenclature as a bunionette excision or lateral condylectomy, constitutes a foundational procedure in the armamentarium of forefoot reconstructive surgery. The bunionette, colloquially termed a "Tailor’s bunion" due to the historical cross-legged sitting posture of tailors that predisposed them to lateral forefoot friction, is defined by a painful, hypertrophic bony prominence on the lateral aspect of the fifth metatarsophalangeal (MTP) joint. This localized prominence frequently precipitates overlying adventitial bursa formation, intractable keratosis, and severe discomfort when the patient is accommodated in standard, commercially available footwear. The patho-epidemiology of this condition demonstrates a strong female predilection, largely driven by the constrictive nature of modern women's footwear, which exerts abnormal compressive and sheer forces across the lateral column of the foot.
The pathomechanics underlying the development of a bunionette deformity are multifactorial and have been elegantly categorized by Coughlin into three distinct morphological types. Type 1 represents an isolated enlargement or hypertrophy of the lateral aspect of the fifth metatarsal head, with otherwise normal forefoot alignment. Type 2 is characterized by an abnormal lateral bowing of the distal diaphysis and metaphysis of the fifth metatarsal, leading to lateral translation of the articular surface. Type 3 is defined by an abnormally widened fourth-to-fifth intermetatarsal angle (IMA), representing a true structural splaying of the lateral forefoot. It is paramount for the operating surgeon to recognize that partial resection of the fifth metatarsal head is biomechanically appropriate almost exclusively for Type 1 deformities. Applying this localized resection technique to Type 2 or Type 3 deformities addresses merely the symptom rather than the architectural pathology, inevitably leading to high rates of recurrence and patient dissatisfaction.
The primary surgical objective of a partial condylar resection is the mechanical decompression of the lateral forefoot to mitigate pressure symptoms induced by footwear impingement. By reducing the cross-sectional width of the fifth metatarsal head by approximately 35% to 40%, the surgeon effectively eliminates the osseous block that conflicts with the shoe's toe box. However, the surgeon must maintain a profound respect for the biomechanical limitations of this procedure. A condylectomy does not, and cannot, correct underlying angular deformities of the metatarsal shaft, nor does it significantly narrow a splayed forefoot. The procedure is fundamentally an exostectomy combined with a soft-tissue balancing of the lateral MTP joint.
Consequently, meticulous patient selection, rigorous preoperative radiographic templating, and precise surgical execution are absolute prerequisites to prevent catastrophic iatrogenic complications. A poorly executed condylectomy can result in severe joint instability, medial subluxation of the fifth digit, avascular necrosis of the remaining metatarsal head, or under-resection leading to persistent impingement. The contemporary orthopedic surgeon must approach this seemingly straightforward procedure with the same anatomical reverence and biomechanical precision as a complex midfoot arthrodesis or a major joint arthroplasty, understanding that the functional demands placed upon the lateral column during the terminal stance phase of gait are substantial and unforgiving of technical error.
Detailed Surgical Anatomy and Biomechanics
A comprehensive, three-dimensional understanding of the lateral forefoot anatomy is non-negotiable for the orthopedic surgeon undertaking a fifth metatarsal head resection. The osteology of the fifth metatarsal is unique; it features a broad base that articulates with the cuboid, a diaphyseal shaft that exhibits a natural, mild lateral and plantar bow, and a bulbous head with a complex articular geometry. The articular cartilage of the fifth MTP joint extends further plantarly and laterally than medially, accommodating the functional demands of the fifth toe during the propulsive phase of gait. The lateral condyle, which is the target of the resection, serves not merely as a bony prominence but as a critical origin site for the lateral collateral ligamentous complex. Resection of this condyle inherently obliterates the origin of the proper and accessory lateral collateral ligaments, instantly rendering the joint dynamically unstable and necessitating meticulous reconstructive capsulorrhaphy during closure.
The neurological topography of the lateral forefoot places two primary sensory nerve branches at significant risk during the surgical approach. Dorsally, the dorsolateral cutaneous branch of the sural nerve courses subcutaneously over the lateral and dorsolateral aspect of the fifth metatarsal shaft and head, providing sensation to the lateral aspect of the fifth digit. Plantarward, the proper digital branch of the lateral plantar nerve to the fifth toe travels in the plantar-lateral subcutaneous tissue. The surgical dissection plane must navigate precisely between these two neurological structures. Iatrogenic transection or aggressive retraction of either nerve can result in a painful postoperative neuroma, complex regional pain syndrome (CRPS), or debilitating localized dysesthesia that completely overshadows the mechanical relief provided by the bunionette excision.
The musculotendinous architecture surrounding the fifth MTP joint is the most critical anatomical consideration for preventing postoperative deformity. The tendon of insertion of the abductor digiti minimi (ADM) acts as the primary dynamic stabilizer against medial deviation of the fifth toe. This robust tendon courses just plantar to the biomechanical midline of the lateral aspect of the fifth metatarsal head, ultimately inserting onto the plantar-lateral tubercle of the base of the proximal phalanx. The flexor digiti minimi brevis lies immediately plantar to the ADM, while the extensor digiti minimi and extensor digitorum longus tendons stabilize the dorsal aspect of the joint.
Biomechanically, the fifth ray operates as an independent, mobile segment that accommodates uneven terrain and absorbs lateral column impact forces during the heel-strike to mid-stance transition. During terminal stance, the fifth MTP joint must transition into a rigid lever to assist in propulsion. If the ADM tendon is inadvertently transected during the capsulotomy—a common error when the incision is made directly on the lateral midline—the delicate balance of forces is irreversibly disrupted. The unopposed pull of the medial joint capsule, the adductor hallucis (transverse head), and the medial intrinsic musculature will rapidly draw the proximal phalanx into a severe, rigid medial subluxation or frank dislocation, often causing the fifth toe to under-ride or over-ride the fourth toe. Therefore, preserving the ADM insertion is the single most critical technical mandate of this procedure.
Exhaustive Indications and Contraindications
The decision to proceed with a partial resection of the lateral condyle rather than a corrective diaphyseal or metaphyseal osteotomy is dictated entirely by the specific pathoanatomy of the patient's foot, as elucidated through rigorous clinical and radiographic examination. The ideal candidate for a simple condylectomy is a patient presenting with a Coughlin Type 1 bunionette deformity. This patient exhibits localized pain, erythema, and adventitial bursa formation directly over the lateral condyle of the fifth metatarsal head. Crucially, this localized pathology must have proven refractory to a comprehensive regimen of conservative management, including aggressive shoe modification (widened toe boxes, soft upper materials), targeted padding, orthotic offloading, and non-steroidal anti-inflammatory drugs (NSAIDs).
From a radiographic perspective, the primary indication for this procedure is a symptomatic lateral prominence in the presence of a strictly normal or only negligibly elevated fourth-to-fifth intermetatarsal angle (IMA). A normal 4-5 IMA is typically defined as less than 8 degrees. Furthermore, the lateral bowing angle of the fifth metatarsal shaft should be within normal physiological limits (typically less than 2.6 degrees). When these radiographic parameters are met, the surgeon can be confident that the pathology is purely localized hypertrophy, and that a 35% to 40% resection of the lateral head will adequately decompress the lateral column without compromising the structural integrity of the forefoot.
Conversely, the contraindications for a simple condylectomy are numerous and must be rigorously respected to avoid surgical failure. The most absolute contraindication is the presence of severe forefoot splaying characterized by a significantly widened 4-5 IMA (Coughlin Type 3 deformity). In such scenarios, a simple exostectomy will fail to narrow the forefoot adequately; the underlying structural splay will persist, and the patient will experience rapid recurrence of symptoms as the remaining metatarsal head continues to impinge against footwear. Similarly, significant lateral bowing of the metatarsal shaft (Coughlin Type 2) necessitates a corrective osteotomy rather than a localized resection. The presence of an intractable plantar keratosis (IPK) directly beneath the fifth metatarsal head is another major caveat. A true IPK indicates structural plantarflexion of the metatarsal; while a plantar condylectomy can theoretically be added to the lateral resection, a rigid IPK strongly dictates the need for an elevating osteotomy of the fifth metatarsal to achieve durable mechanical offloading.
Indications and Contraindications Matrix
| Parameter | Primary Indications (Proceed with Condylectomy) | Absolute/Relative Contraindications (Consider Osteotomy or Avoid Surgery) | Rationale / Clinical Consequence |
|---|---|---|---|
| Deformity Type | Coughlin Type 1 (Isolated lateral condylar hypertrophy) | Coughlin Type 2 (Lateral bowing) or Type 3 (Widened IMA) | Resection fails to correct structural angular deformity; high recurrence rate in Types 2 and 3. |
| Radiographic 4-5 IMA | Normal (< 8 degrees) | Widened (> 8 to 10 degrees) | High IMA indicates forefoot splay. Exostectomy will not narrow the foot sufficiently. |
| Plantar Pathology | Mild, diffuse callus or absent plantar pathology | Intractable Plantar Keratosis (IPK) beneath the 5th metatarsal head | IPK implies a plantarflexed ray requiring an elevating osteotomy for durable mechanical relief. |
| Conservative Care | Failed minimum 3-6 months of shoe modification/padding | Patient has not attempted conservative footwear modifications | Surgery should never be the first-line treatment for friction-based forefoot pathologies. |
| Joint Status | Congruous, stable 5th MTP joint with preserved cartilage | Severe osteoarthritis, Charcot arthropathy, or pre-existing instability | Resection may exacerbate instability; arthritic joints may require arthroplasty or resection arthroplasty. |
| Vascular Status | Normal palpable pulses, ABI > 0.9 | Severe peripheral arterial disease (PAD), ABI < 0.5 | High risk of wound dehiscence, infection, and failure to heal the capsular repair. |
Pre-Operative Planning, Templating, and Patient Positioning
Preoperative planning for a partial resection of the fifth metatarsal head demands a meticulous synthesis of clinical examination findings and precise radiographic templating. The clinical evaluation must assess the exact location of the pain—differentiating between direct lateral pressure pain, plantar pressure pain (IPK), and intra-articular pain indicative of degenerative joint disease. The surgeon must evaluate the flexibility of the deformity and the baseline stability of the fifth MTP joint. A thorough neurovascular examination is mandatory, documenting baseline sensation and palpable pedal pulses, as compromised microvascular flow significantly increases the risk of postoperative wound complications and delayed healing of the capsular imbrication.
Standardized, weight-bearing radiographs of the foot (anteroposterior, lateral, and oblique views) are the cornerstone of surgical templating. Non-weight-bearing films are entirely inadequate for assessing forefoot splay and intermetatarsal angles. On the AP weight-bearing view, the surgeon must measure the fourth-to-fifth intermetatarsal angle (IMA), the fifth metatarsophalangeal angle, and the lateral bowing angle of the fifth metatarsal shaft. Once a Type 1 deformity is confirmed, the surgeon utilizes digital or physical templates to plan the osteotomy. The goal is to delineate a resection line that removes approximately 35% to 40% of the lateral metatarsal head. The planned cut must originate distally at the medial border of the lateral prominence and exit proximally at the metaphyseal flare, ensuring a smooth, flush transition with the lateral cortex of the diaphysis to prevent a postoperative step-off.
Patient counseling during the preoperative phase is as critical as the radiographic templating. The cosmetic correction achieved by a simple condylectomy is frequently less dramatic than the patient anticipates. Causes of postoperative dissatisfaction often stem from a fundamental misunderstanding of the procedure's biomechanical goals. The surgeon must explicitly warn the patient that only the painful bony prominence will be removed, and that the overall width of the forefoot will not be altered appreciably. The patient must understand that the primary goal is pain relief in sensible footwear, not the creation of a narrow foot capable of fitting into extreme, high-heeled, pointed-toe shoes. Managing these cosmetic expectations preoperatively mitigates postoperative friction and ensures patient satisfaction.
On the day of surgery, the patient is placed in the supine position on the operating table. A small bump or sandbag is typically placed under the ipsilateral hip to internally rotate the lower extremity slightly. This positioning maneuver brings the lateral border of the foot into a direct, accessible, and ergonomic view for the primary surgeon, preventing the need for awkward leaning or continuous assistant retraction. The procedure is optimally performed under regional anesthesia—typically a popliteal sciatic nerve block combined with a saphenous nerve block, or a comprehensive ankle block—supplemented with monitored intravenous sedation. A well-padded calf or ankle pneumatic tourniquet is applied and inflated following exsanguination to ensure a pristine, bloodless surgical field, which is critical for identifying and protecting the delicate subcutaneous neurological structures.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of the partial condylar resection requires strict adherence to anatomical planes and precise osseous contouring.
1. Incision and Exposure
The preferred approach is a straight lateral longitudinal incision, although a dorsolateral incision may be utilized based on surgeon preference or specific local skin conditions (e.g., avoiding a direct lateral scar over a prominent bursa). Make a straight lateral incision extending from the junction of the middle and distal thirds of the fifth metatarsal shaft, carrying it distally to the midshaft of the proximal phalanx.

It is imperative to incise only the epidermis and superficial dermis initially. Deepening the incision too rapidly with the scalpel risks inadvertent transection of the delicate subcutaneous nerves.

Utilize blunt dissection with a hemostat or Stevens tenotomy scissors to carefully spread the subcutaneous tissues. If utilizing the straight lateral approach, the dissection plane must be meticulously maintained safely between the dorsolateral cutaneous branch of the sural nerve (located dorsally) and the proper digital branch of the lateral plantar nerve (located plantarward). Gentle, broad-bladed retractors (such as Ragnell or Senn retractors) should be used to protect these neurological structures throughout the procedure.
2. Capsulotomy and Soft Tissue Preservation
The approach to the joint capsule represents the most critical juncture in preventing catastrophic postoperative toe deformity. The tendon of insertion of the abductor digiti minimi (ADM) passes just plantar to the biomechanical midline of the lateral aspect of the fifth metatarsal head. If the periosteal and capsular incision is made exactly on the midline or plantar to it, this vital dynamic stabilizer will be transected. Therefore, the capsular incision must be made in a straight longitudinal line exactly 2 to 3 mm dorsal to the midline.
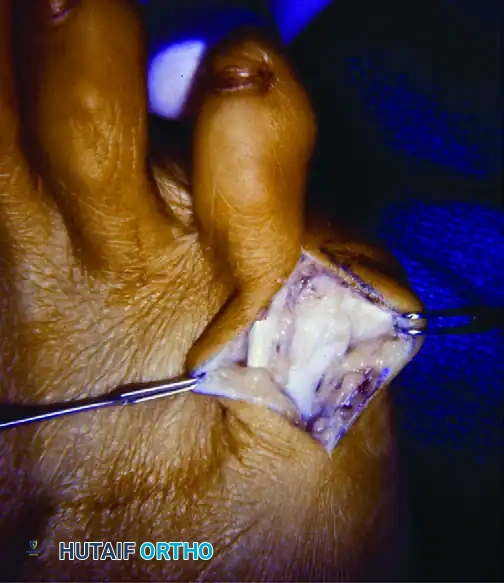
Following this dorsal offset rule, incise the capsule and periosteum down to bone. By sharp dissection using a #15 blade or a small periosteal elevator, elevate the capsule dorsally and plantarward, creating full-thickness flaps. The plantar flap will contain the preserved ADM tendon. Deliver the fifth metatarsal head laterally into the wound while simultaneously pushing the proximal phalanx medially.
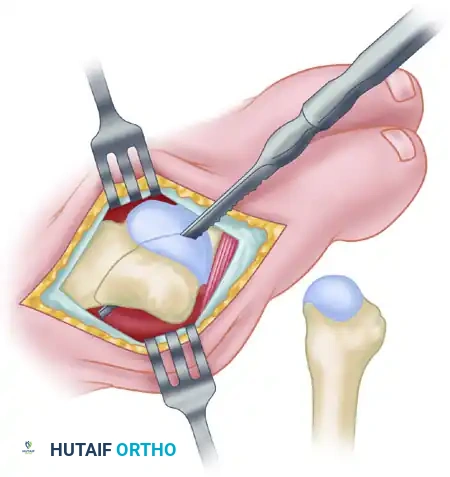
It is a crucial step to fully expose the medial edge of the articular cartilage. Failure to visualize the entire articular surface often leads to optical illusions regarding the true size and center of the metatarsal head, frequently resulting in massive over-resection.
3. Osteotomy and Condylar Resection
The objective of the osteotomy is to completely remove the hypertrophic lateral eminence without compromising the weight-bearing capacity of the metatarsal head or permanently destabilizing the joint articulation. Approximately 35% to 40% of the metatarsal head is typically removed. Using a thin osteotome or a small, fine-toothed sagittal saw blade, score the proximal margin of the proposed osteotomy at the metaphyseal flare.
Direct the saw cut in a strictly dorsal distal-to-plantar proximal direction. This oblique orientation is biomechanically superior to a straight vertical cut, as it ensures a smooth transition at the metaphyseal-diaphyseal junction and prevents the creation of a sharp, prominent bony step-off that could serve as a new nidus for recurrent lateral pressure symptoms.
During the saw cut, utilize continuous cold saline irrigation to prevent thermal necrosis of the remaining bone, which could predispose the fragment to avascular necrosis.
4. Addressing the Phalanx and Plantar Condyle
Once the primary metatarsal resection is complete, attention must be turned to the adjacent osseous structures to ensure a comprehensive decompression. Reduce the proximal phalanx over the remaining portion of the fifth metatarsal head and palpate the lateral flare of the base of the proximal phalanx. If this flare produces a projecting bony prominence that may rub against the shoe or the fourth toe, excise it meticulously with a rongeur or bone-biter.
Evaluate the plantar aspect of the metatarsal head. If a mild plantar callus coexists beneath the metatarsal head, use a bone rasp or the sagittal saw to smooth the plantar projection of the condyle flush with the shaft. Before proceeding to closure, meticulously round off all remaining bone edges—dorsal, plantar, and proximal—with a fine bone rasp to prevent any sharp edges from irritating the overlying soft tissues.
5. Capsular Imbrication and Closure
Because the partial resection inherently removes the origin of the lateral collateral ligament, the joint is rendered temporarily unstable. The closure is not merely an anatomical reapproximation of tissue; it is a critical reconstructive stabilization step. An imbricating (pants-over-vest) capsular closure is absolutely imperative to restore lateral resting tension and prevent medial drift of the digit.
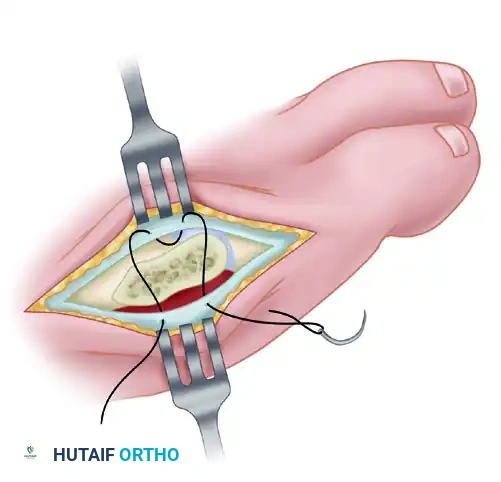
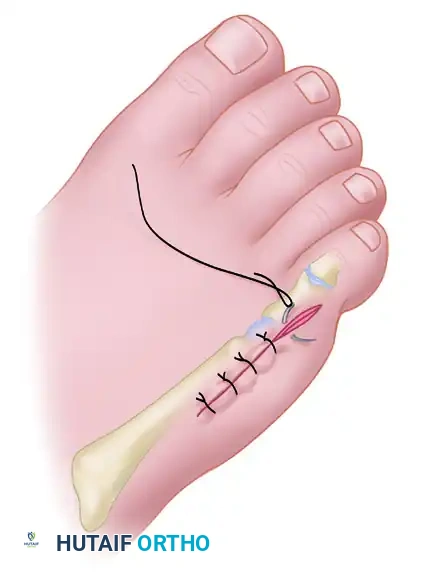
Ensure that the abductor digiti minimi insertion remains securely attached and is incorporated into the robust plantar leaf of the capsular repair. Use strong, absorbable sutures (e.g., 2-0 or 3-0 Vicryl) for the capsular imbrication. The surgical assistant must hold the fifth toe in slight abduction and neutral dorsiflexion/plantarflexion while the sutures are tensioned and tied. This sets the appropriate resting length of the lateral capsule.
Once the capsule is securely imbricated and joint stability is confirmed, close the skin with interrupted, nonabsorbable sutures (e.g., 4-0 Nylon or Prolene) using a vertical mattress or simple interrupted technique to ensure precise epidermal eversion.

Complications, Incidence Rates, and Salvage Management
While technically straightforward when performed by an experienced orthopedic surgeon, partial resection of the fifth metatarsal head carries specific, highly morbid risks that can lead to devastating patient outcomes if meticulous technique is not observed. The most dreaded and functionally debilitating complication of a simple bunionette excision is medial subluxation or frank dislocation of the fifth MTP joint.
This catastrophic complication occurs almost exclusively due to iatrogenic transection of the abductor digiti minimi tendon during the initial capsulotomy, or failure to perform an adequate, tensioned imbricating capsular closure after removing the lateral collateral ligament origin. The unopposed pull of the medial joint capsule and adductor structures rapidly pulls the toe into a severe, rigid varus deformity, often causing the fifth toe to painfully overlap or underlap the fourth toe.

Inadequate resection represents another frequent pitfall. Failure to remove the recommended 35% to 40% of the metatarsal head, or failure to adequately smooth the proximal metaphyseal flare with a rasp, will result in persistent lateral pressure symptoms. The patient will continue to experience pain in closed shoes, essentially rendering the surgery a failure and necessitating a revision exostectomy. Conversely, over-resection (removing more than 50% of the metatarsal head) severely compromises articular congruity. This leads to immediate joint subluxation, severe postoperative stiffness, and a high risk of avascular necrosis (AVN) of the remaining, devascularized articular fragment. This underscores the absolute necessity of fully exposing the medial articular cartilage to accurately judge the geometric center of the head before initiating the saw cut.
Finally, performing this localized procedure on a patient with a severely widened 4-5 IMA (forefoot splaying) represents a failure of surgical indication rather than surgical technique. The underlying structural splaying will persist unabated, and the lateral soft tissues will continue to be subjected to high friction forces against footwear, leading to rapid recurrence of the bursa and pain. Nerve injuries, particularly to the sural nerve branches, can result in debilitating neuromas that are notoriously difficult to treat, often requiring subsequent excision and nerve burying procedures.
Complications and Salvage Strategies Matrix
| Complication | Estimated Incidence | Primary Etiology | Salvage Management / Revision Strategy |
|---|---|---|---|
| Medial Subluxation / Dislocation | 5% - 10% | Transection of ADM tendon; inadequate lateral capsular imbrication. | Medial capsular release, extensor tenotomy, lateral capsular reconstruction, K-wire stabilization. |
| Recurrent Pain / Under-resection | 10% - 15% | Resecting < 30% of the head; leaving a sharp proximal metaphyseal step-off. | Revision surgery for further exostectomy and aggressive metaphyseal contouring. |
| Over-resection / Avascular Necrosis | < 5% | Resecting > 50% of the head; thermal necrosis from saw blade. | Conservative management (custom orthotics); if severe, 5th MTP joint resection arthroplasty or implant. |
| Sural Nerve Neuritis / Neuroma | 2% - 5% | Aggressive retraction; direct scalpel transection during superficial dissection. | Gabapentinoids, targeted steroid injections; surgical neuroma excision and proximal nerve burying. |
| Persistent Forefoot Splay | Variable | Incorrect indication (performing condylectomy on a Type 3 deformity). | Revision utilizing a corrective 5th metatarsal osteotomy (e.g., Scarf, Ludloff, or distal chevron). |
Phased Post-Operative Rehabilitation Protocols
A highly structured, phased postoperative rehabilitation protocol is essential to protect the delicate lateral capsular repair while simultaneously promoting early, safe mobility to prevent joint stiffness and deep vein thrombosis. The rehabilitation timeline is dictated by the biological healing phases of the soft tissues, as the osseous resection itself does not require prolonged immobilization for fracture union.
Phase 1: Immediate Postoperative Phase (Days 1-14)
Immediately following skin closure, the foot is placed in a meticulously applied, bulky, compressive dressing. Crucially, this dressing is not merely protective; it acts as a dynamic splint. The bandages must be applied with specific tension to hold the fifth toe in slight abduction and neutral alignment. This positioning releases tension on the lateral capsular repair and acts as a physical barrier against medial drift. Bathroom privileges and weight-bearing to tolerance on the heel and flat foot are allowed starting on the first postoperative day. The patient must be fitted with a firm-soled postoperative shoe or a controlled ankle motion (CAM) boot with an open toe box to accommodate the bulky dressing and strictly prevent any lateral forefoot compression. Elevation of the limb above the level of the heart is mandated for 45 minutes of every hour during the first 72 hours to minimize edema and hematoma formation.
Phase 2: The Two-Week Milestone and Subacute Healing (Weeks 2-6)
The patient returns to the orthopedic clinic at approximately 10 to 14 days for the first wound inspection. If the incision is fully coapted and healing optimally, the nonabsorbable skin sutures are removed. At this critical juncture, a soft toe spacer (fabricated from medical-grade silicone or dense foam) is placed deep within the fourth web space. This spacer acts as a constant mechanical block to prevent medial deviation of the fifth toe, thereby protecting the healing lateral capsular repair from pathological strain during ambulation. The patient continues to use this fourth web space spacer continuously for an additional 4 weeks. Weight-bearing continues to tolerance, transitioning from the postoperative shoe into a wide, supportive athletic shoe with a generous toe box, depending on the resolution of postoperative swelling.
Phase 3: Six-Week Milestone and Long-Term Maintenance (Weeks 6 and Beyond)
At the 6-week postoperative mark, the capsular imbrication is generally considered biologically stable enough to withstand normal physiological loads and the sheer forces of standard gait. The toe spacer may be discontinued. The patient is allowed to transition into more fashionable, commercially available shoes as tolerated. However, the surgeon must strongly counsel the patient that returning to the exact constrictive, narrow-toed footwear that precipitated the initial deformity will significantly increase the risk of recurrence or contralateral disease. Wide toe-box footwear is strongly encouraged as a long-term lifestyle modification. Patients should be advised that while pain relief is often rapid, the full resolution of postoperative edema and the final maturation of
