INTRODUCTION TO REGIONAL OSTEOMYELITIS
The surgical management of osteomyelitis is dictated not only by the chronicity of the infection and the virulence of the offending pathogen but fundamentally by the unique pathoanatomy of the involved region. Unlike diaphyseal long bone infections, where cylindrical cortical resection and intramedullary reaming are standard, osteomyelitis affecting the calcaneus, distal femur, and pelvic ring presents distinct biomechanical and neurovascular challenges.
In these specific regions, the relationship between the periosteum, the underlying cancellous architecture, and the adjacent soft-tissue envelope dictates the pattern of bone destruction and the subsequent surgical approach. The overarching principles of treatment remain constant: aggressive debridement of all necrotic tissue (sequestrectomy), obliteration of dead space, restoration of vascularity, and stabilization of the skeletal segment. However, the execution of these principles requires a master-level understanding of regional anatomy to prevent catastrophic complications such as pathological fractures, neurovascular compromise, or chronic, painful ulcerations.
OSTEOMYELITIS OF THE CALCANEUS
Pathoanatomy and Biomechanics
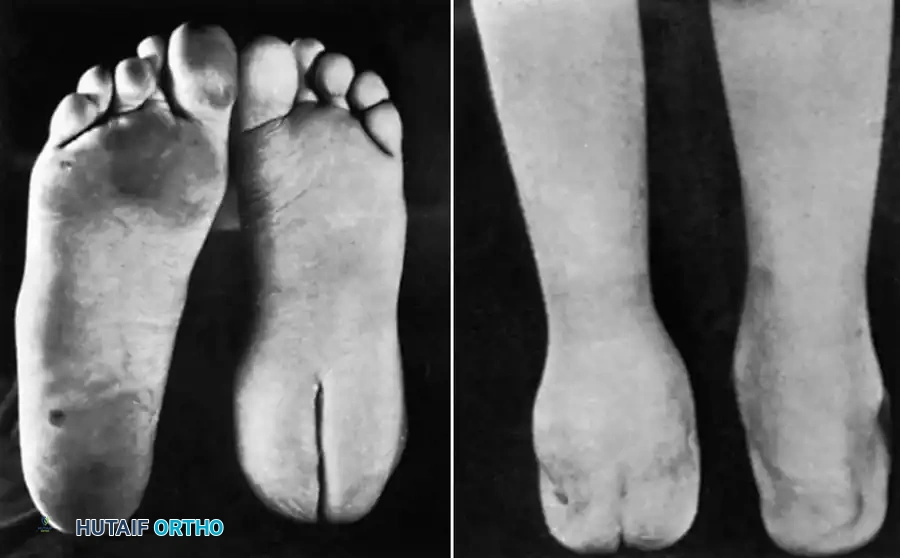
Osteomyelitis of the calcaneus, similar to infections of other tarsal bones, exhibits a unique pathophysiological progression. The calcaneus is predominantly composed of cancellous bone enclosed within a thin cortical shell. Crucially, the periosteum of the calcaneus is densely and firmly adherent to the underlying cortex.
When purulent material accumulates within the medullary cavity, it does not easily strip the periosteum to form a subperiosteal abscess. Instead, the rising intraosseous pressure causes the purulence to perforate directly through the cortex and periosteum. Consequently, the extensive cortical destruction and robust involucrum formation typically seen in long bone osteomyelitis are minimal or entirely absent in the calcaneus.
Surgical Warning: Because involucrum formation is minimal, aggressive resection of the calcaneal cortex can lead to catastrophic structural collapse. Debridement must be meticulous, focusing on the removal of internal cancellous sequestra while preserving the structural integrity of the cortical shell to maintain the biomechanics of the hindfoot.
Surgical Approaches to the Calcaneus
For localized abscesses, standard medial and lateral approaches to the calcaneus are generally satisfactory for simple incision and drainage. However, in cases of chronic, diffuse osteomyelitis of the calcaneus, these approaches provide inadequate exposure for thorough intralesional debridement and often fail to eradicate the infection.
For extensive chronic osteomyelitis, Gaenslen’s split heel approach through the plantar surface is the gold standard. While seemingly counterintuitive to incise directly through the primary weight-bearing surface of the foot, the biomechanical healing of this specific incision is highly favorable. The resulting scar is deeply situated within the plantar fat pad. As the wound heals, the thick, compartmentalized fibrofatty tissues on either side of the incision curl inward, forming thick, protective cushions. This anatomical retraction ensures that the mature scar does not bear direct pressure during the heel-strike phase of the gait cycle, rendering it entirely painless.
🔪 Surgical Technique: Gaenslen’s Split Heel Approach
Patient Positioning and Preparation:
1. Place the patient in the prone position on a radiolucent operating table.
2. Place a well-padded support beneath the affected anterior ankle to maintain the foot in a neutral or slightly dorsiflexed position, providing optimal exposure of the plantar heel.
3. Utilize a thigh tourniquet to ensure a bloodless surgical field, which is critical for identifying the neurovascular structures and distinguishing necrotic from viable bone.
Incision and Superficial Dissection:
1. Make a longitudinal incision exactly in the midline of the plantar aspect of the heel.
2. Begin the incision at the level of the base of the fifth metatarsal and extend it posteriorly for 2.5 to 4 cm, continuing proximally to split the distal insertion of the Achilles tendon.
3. Deepen the incision through the thick plantar skin and subcutaneous fat pad.
Deep Dissection and Neurovascular Protection:
1. Identify and incise the plantar aponeurosis strictly in the internervous and intermuscular plane between the abductor digiti quinti (innervated by the lateral plantar nerve) and the flexor digitorum brevis muscles (innervated by the medial plantar nerve).
2. Critical Step: In the distal angle of the wound, carefully identify the lateral plantar artery and nerve. Gently retract these structures medially to protect them from iatrogenic injury during the deeper exposure.
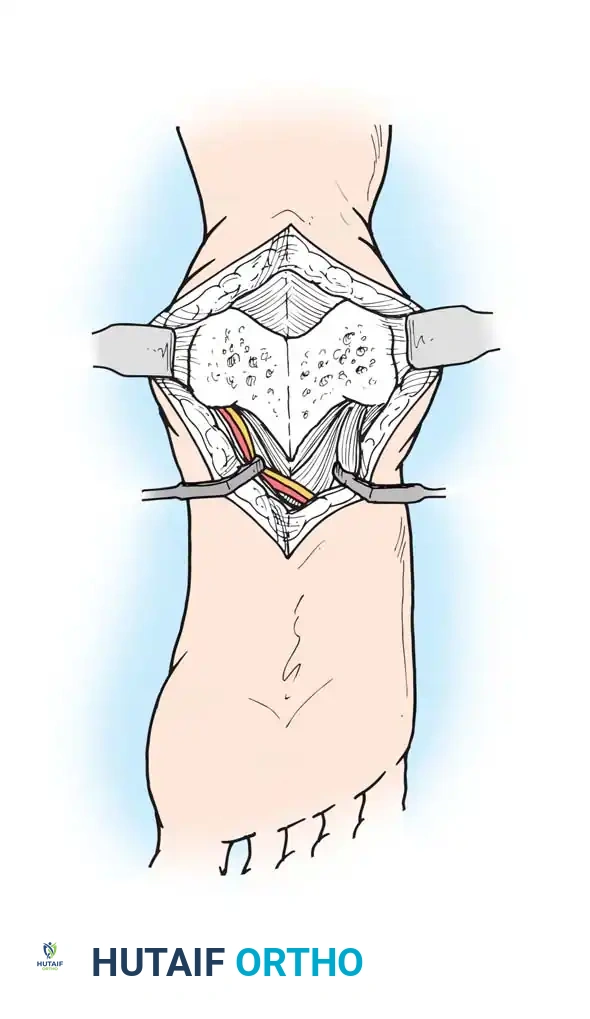
Osseous Exposure and Debridement:
1. Expose the quadratus plantae muscle. Split its fibers longitudinally along with the underlying long plantar ligament to expose the plantar cortex of the calcaneus.
2. Using a broad, sharp osteotome, divide the calcaneus longitudinally from posterior to anterior.
3. Insert a lamina spreader or broad retractors to separate the two halves of the calcaneus, exposing the interior cancellous architecture like an open book. If necessary, the subtalar joint can be visualized by increasing the retraction force.
4. Perform a radical sequestrectomy. Use curettes and a high-speed burr to remove all sequestra, purulent material, and obviously infected or necrotic cancellous bone.
5. Preservation of Cortex: Damage the outer cortical shell as little as possible to prevent structural collapse of the hindfoot.
6. Irrigate the cavity copiously with pulsatile lavage using sterile saline.
Closure:
1. Do not attempt a tight primary closure. Close the wound loosely over surgical drains, or pack the cavity with antibiotic-impregnated calcium sulfate beads or a polymethylmethacrylate (PMMA) spacer if dead space management is required.
2. Allow the deep plantar tissues to heal by secondary intention to facilitate the inward curling of the fat pad.
Postoperative Protocol:
* Apply a well-padded short leg cast with the foot in a strictly neutral position and the ankle at 90 degrees to prevent equinus contracture.
* Cut a window in the cast over the plantar calcaneus to permit regular wound inspection and dressing changes.
* Strict non-weight-bearing is enforced until radiographic and clinical evidence of bone consolidation and soft-tissue healing is observed, typically 8 to 12 weeks.
OSTEOMYELITIS OF THE DISTAL THIRD OF THE FEMUR
Pathoanatomy and Clinical Challenges
Chronic osteomyelitis of the distal third of the femur is notoriously difficult to eradicate. The anatomical configuration of the distal femur, combined with the local fascial compartments, creates a highly unfavorable environment when infected.
When an infection takes hold in the distal femoral metaphysis, purulent material frequently breaks through the posterior cortex. Because the posterior periosteum is relatively loose compared to the anterior aspect, a massive subperiosteal abscess can develop. This abscess completely separates the periosteum from the posterior cortex, effectively stripping the bone of its extrinsic blood supply. Consequently, large segments of the posterior femur undergo avascular necrosis, leading to persistent, draining sinuses.
Furthermore, the body's attempt to wall off the infection results in a dense mass of avascular scar tissue in the popliteal space. This scar tissue acts as a mechanical barrier, preventing the revascularization of the diseased bone. Surgically, this posterior scar mass is exceptionally hazardous to navigate due to its immediate proximity to the popliteal artery, popliteal vein, and the tibial and common peroneal nerves.
Clinical Pearl: Direct posterior approaches to the distal femur for osteomyelitis are fraught with danger due to the distorted anatomy and encased neurovascular bundle. A lateral approach with posterolateral fenestration is the safest and most effective method to achieve dependent drainage and adequate debridement.
🔪 Surgical Technique: Posterolateral Fenestration
Positioning and Incision:
1. Place the patient in the supine position with a bump under the ipsilateral hip to internally rotate the leg slightly, bringing the lateral aspect of the thigh into full view.
2. Make a lateral longitudinal incision over the distal third of the thigh. Begin the incision exactly 5 cm proximal to the lateral joint line of the knee and extend it proximally for approximately 10 cm.
Superficial and Deep Dissection:
1. Incise the iliotibial band longitudinally in line with the skin incision.
2. Identify the vastus lateralis muscle. Elevate and retract the vastus lateralis anteriorly, dissecting it off the lateral intermuscular septum. Ligate or cauterize the perforating branches of the profunda femoris artery as they are encountered.
3. Expose the lateral and posterolateral surfaces of the distal femoral shaft and metaphysis.
Joint Protection and Fenestration:
1. Critical Warning: Strictly avoid opening the knee joint at the distal extent of the incision. The suprapatellar bursa extends proximally beneath the quadriceps; inadvertently breaching this capsule will contaminate a sterile knee joint with purulent material from the osteomyelitic focus. Confine all osseous work strictly to the lateral and posterolateral diaphyseal-metaphyseal junction.
2. Use a surgical drill to outline an oval cortical window on the posterolateral surface of the femur. An oval shape minimizes stress risers compared to a rectangular window.
3. Connect the drill holes with a sharp osteotome and remove the cortical window.
4. Enter the medullary canal proximal to the metaphysis. Thoroughly curette and debride the canal.
5. The posterolateral placement of this window is strategic; it allows for gravity-assisted, dependent drainage of pus posteriorly away from the anterior compartment and knee joint.
Postoperative Protocol:
* The structural integrity of the distal femur is significantly compromised by both the infection and the surgical fenestration.
* The limb must be splinted with the knee in full extension until the soft tissues have healed.
* Prolonged protected weight-bearing (using crutches or a walker) is mandatory during ambulation to prevent a catastrophic pathological fracture through the cortical window.
OSTEOMYELITIS OF THE PELVIS: ILIUM
Acute Phase Management and Systemic Considerations
Osteomyelitis of the ilium is a severe, limb- and life-threatening condition. In the acute stage, the highly vascular cancellous bone of the ilium is rapidly invaded throughout its entirety. The infection quickly breaches the thin cortices, resulting in massive subperiosteal abscesses on both the medial (iliac fossa) and lateral (gluteal surface) cortices.
The clinical presentation is notoriously deceptive. Because of the proximity to the peritoneum and the hip joint, early symptoms frequently mimic acute appendicitis, pelvic inflammatory disease, or pyogenic arthritis of the hip. A high index of suspicion, coupled with advanced imaging (MRI of the pelvis), is required for an accurate diagnosis.
Before any surgical intervention, aggressive systemic resuscitation is paramount. Patients often present in a state of sepsis. Intravenous broad-spectrum antibiotics must be initiated immediately after blood cultures are drawn. Due to the highly vascular nature of the pelvis and the potential for massive intraoperative blood loss, blood transfusions may be necessary preoperatively, and adequate cross-matched blood must be available in the operating room.
Systemic Correlation: Ghahremani and colleagues highlighted a critical association between osteomyelitis of the ilium and Crohn’s disease (granulomatous enteritis and colitis). In these complex cases, fistulous tracts from the diseased bowel directly seed the pelvic bones. Eradication of the osteomyelitis is impossible without concurrent general surgical intervention to resect the involved bowel segments. Furthermore, pelvic osteomyelitis associated with intestinal lesions has a high incidence of anaerobic bacterial involvement, necessitating tailored antibiotic therapy.
Surgical Principles for the Ilium
The surgical management of iliac osteomyelitis requires a radical approach. Limited incision and drainage are universally associated with high recurrence rates. The goal is to remove all individual sequestra and completely drain the medial and lateral abscess cavities.
Because the iliac wing does not bear the primary weight of the axial skeleton (which is transmitted through the sacroiliac joint to the sciatic notch and down the femur), most of the iliac wing can be resected without causing significant biomechanical disability. Therefore, a partial pelvectomy (resecting the diseased iliac wing) is highly preferable to less radical, tissue-sparing operations that leave infected bone behind. The resection must be carried down to bleeding, healthy bone, often requiring the detachment and subsequent reattachment of the gluteal and abdominal musculature.
OSTEOMYELITIS OF THE ISCHIUM AND PUBIS
Pathoanatomy and Patient Populations
Osteomyelitis of the ischium and pubis presents unique challenges due to the complex muscular anatomy and the specific patient populations typically affected. When an infection localizes in these regions, abscesses typically develop deep within the pelvis, either beneath the external or internal obturator muscles or tracking inferiorly into the ischiorectal fossa.
Osteomyelitis of the ischial tuberosity is exceptionally common in bedridden, paralyzed, or spinal cord injury (paraplegic/tetraplegic) patients. In this demographic, prolonged pressure over the bony prominences leads to ischemic necrosis of the overlying skin and soft tissues (decubitus ulcers). These pressure sores inevitably become secondarily infected with polymicrobial flora (including anaerobes and Gram-negative bacilli), leading to direct contiguous spread into the ischium, causing profound osteomyelitis and bone necrosis.
Surgical Approaches and Reconstruction
For isolated osteomyelitis of the ischium and pubis not associated with massive pressure sores, McWhorter recommended a specialized drainage approach. This incision is strategically located away from the perineum to drastically decrease the risk of postoperative wound contamination from fecal and urinary flora. The approach allows for wide retraction of the gracilis and adductor muscle groups. If the infection extends deeply, the obturator membrane can be incised, allowing the surgeon to explore and debride the deep, intrapelvic surfaces of the bone.
For the paraplegic patient with ischial osteomyelitis secondary to a pressure sore, simple debridement is insufficient. Effective treatment mandates a multidisciplinary approach:
1. Radical Osseous Debridement: Complete ostectomy of the infected ischial tuberosity. The bone must be resected back to bleeding, viable margins.
2. Soft-Tissue Reconstruction: The resulting massive dead space cannot be left open. A soft-tissue transfer is universally required to close the defect, provide robust padding over the remaining bone, and bring a new blood supply to the region. This is typically achieved using regional muscle or myocutaneous flaps, such as the gluteus maximus flap, V-Y hamstring advancement flaps, or inferior gluteal artery perforator (IGAP) flaps.
For osteomyelitis localizing specifically to the region of the pubic symphysis (often seen following urological procedures, pelvic trauma, or in athletes as a progression of osteitis pubis), conservative measures often fail. Kelikian et al. advised that when less radical treatments are ineffective, complete en bloc resection of the pubic symphysis is required to eradicate the nidus of infection. While this alters the anterior pelvic ring, the posterior sacroiliac ligamentous complex usually provides sufficient stability to allow for functional, albeit sometimes altered, ambulation.
OSTEOMYELITIS OF THE SPINE
Infections involving the vertebral column, including pyogenic spondylodiscitis and epidural abscesses, present with profound neurological risks and require highly specialized anterior and posterior reconstructive techniques. The detailed pathophysiology, surgical indications, and operative management of osteomyelitis of the spine are comprehensively discussed in Chapter 40.
