Osteomyelitis: Comprehensive Surgical Management and Classification
Key Takeaway
Osteomyelitis remains one of the most challenging pathologies in orthopedic surgery, requiring a multidisciplinary approach for eradication. This comprehensive guide details the pathophysiology, classification systems, and evidence-based surgical management of bone infections. Key principles include aggressive surgical debridement, targeted antimicrobial therapy, and meticulous dead space management using local antibiotic delivery systems or soft-tissue transfers to restore osseous integrity and prevent chronic recurrence.
Introduction to Osteomyelitis
Osteomyelitis has historically represented one of the most difficult and challenging problems confronted by orthopaedic surgeons. In the early 1900s, prior to the advent of penicillin and modern surgical techniques, approximately 20% of patients with osteomyelitis died from systemic sepsis, and those who survived suffered profound morbidity, including chronic draining sinuses, limb deformity, and amputation.
Currently, while mortality from osteomyelitis is relatively low due to advanced antimicrobial therapies and aggressive surgical protocols, the morbidity remains substantial. Osteomyelitis is notoriously difficult to treat effectively due to the unique microanatomy of bone, which provides a sanctuary for bacterial biofilms, shielding them from both systemic antibiotics and host immune responses.
The cornerstone of successful management is early diagnosis coupled with appropriate, aggressive surgical debridement and targeted antimicrobial treatment. A multidisciplinary approach is mandatory, requiring seamless collaboration between the orthopaedic surgeon, an infectious disease specialist, and a plastic surgeon, particularly in complex cases involving significant soft-tissue loss or compromised vascularity.
Osteomyelitis is strictly defined as an inflammation of the bone caused by an infecting organism. The infection may be localized to a single portion of the bone or may involve multiple anatomical regions, including the medullary marrow, cortical bone, periosteum, and the surrounding soft-tissue envelope. While the infection is generally monomicrobial (frequently Staphylococcus aureus), polymicrobial infections are increasingly common, particularly in the context of the diabetic foot, open fractures, and contiguous spread from decubitus ulcers.
Pathophysiology and Biomechanics of Bone Infection
Understanding the pathophysiology of osteomyelitis is critical for executing effective surgical interventions. The pathogenesis depends heavily on the mechanism of bacterial inoculation, the virulence of the organism, and the host's immune status.
Biofilm Formation
The hallmark of chronic osteomyelitis is the formation of a bacterial biofilm. Once bacteria adhere to necrotic bone or orthopaedic implants, they undergo a phenotypic shift from a planktonic (free-floating) state to a sessile state, secreting a protective extracellular polymeric substance (EPS) known as the glycocalyx.
Clinical Pearl: Bacteria encased within a mature biofilm can survive antibiotic concentrations up to 1,000 times higher than those required to kill their planktonic counterparts. Therefore, systemic antibiotics alone are fundamentally incapable of curing chronic osteomyelitis; physical surgical disruption and removal of the biofilm (debridement) are absolute prerequisites for eradication.
The Ischemic Cascade
As bacteria proliferate within the rigid, non-expansile confines of the bone marrow, the localized inflammatory response leads to purulent exudate formation. The accumulation of pus increases intraosseous pressure, compressing the delicate intramedullary vascular sinusoids. This vascular compromise leads to localized bone ischemia and subsequent necrosis.
The dead cortical bone, stripped of its endosteal and periosteal blood supply, becomes a sequestrum—a devitalized fragment of bone that serves as a permanent nidus for infection. In response, the surrounding viable periosteum attempts to wall off the infection by forming a reactive shell of new bone known as an involucrum. Defects in the involucrum, termed cloacae, allow pus to decompress and track into the surrounding soft tissues, eventually forming a cutaneous sinus tract.
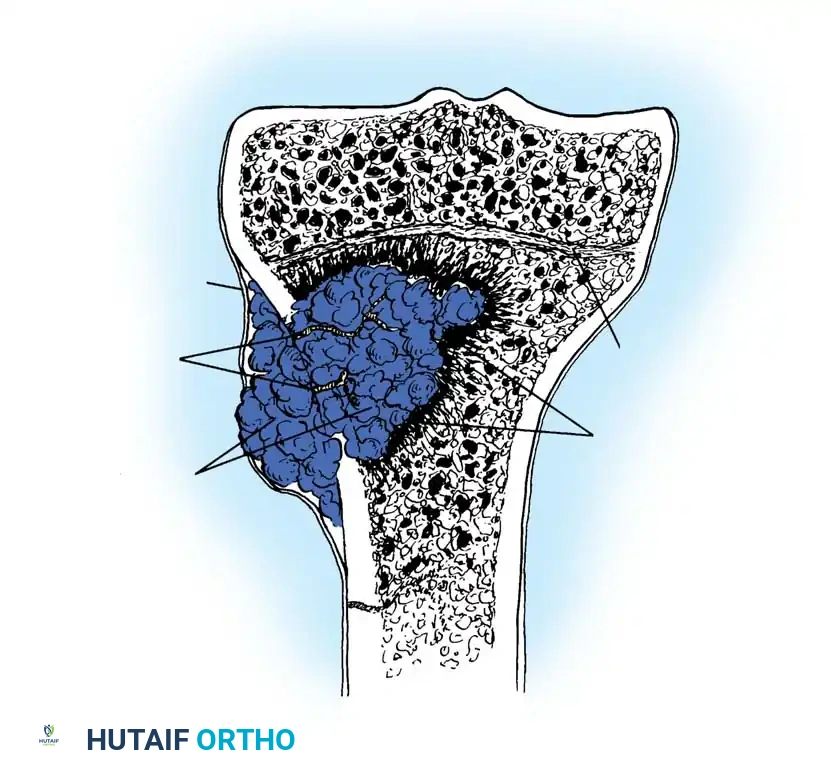
The illustration above demonstrates the classic progression of acute hematogenous osteomyelitis in a pediatric long bone. Note the metaphyseal abscess expanding through the Haversian and Volkmann canals, creating holes in the cortex. The purulent exudate breaches the cortex, lifting the periosteum to form a subperiosteal abscess, while inflammatory cells infiltrate the surrounding tissues. The epiphyseal plate typically acts as a barrier to joint involvement in older children, though transphyseal vessels in neonates can lead to concomitant septic arthritis.
Classification Systems
Classification of osteomyelitis is essential for standardizing communication, guiding treatment algorithms, and predicting prognosis. Classification is traditionally based on the duration of symptoms, the mechanism of infection, and the host's physiological response.
1. Classification by Duration and Mechanism
- Acute Osteomyelitis: Typically presents within 2 weeks of disease onset. It is characterized by suppurative infection accompanied by systemic signs of toxicity (fever, chills) and local signs of inflammation.
- Subacute Osteomyelitis: Presents between 2 weeks and 3 months. The host immune system and the bacterial virulence are in a state of equilibrium. A classic manifestation is the Brodie abscess—a localized, walled-off purulent cavity often found in the metaphysis of long bones.
- Chronic Osteomyelitis: Defined by the presence of necrotic bone (sequestrum), biofilm formation, and often a draining sinus tract. It can persist for months to decades.
The mechanism of infection is broadly divided into:
* Hematogenous: Resulting from bacteremia. Most common in children (metaphyseal seeding) and the elderly (vertebral osteomyelitis).
* Exogenous (Contiguous): Caused by direct inoculation via open fractures, penetrating trauma, iatrogenic surgical contamination, or contiguous spread from adjacent infected soft tissues (e.g., diabetic foot ulcers).
2. The Cierny-Mader Classification
The Cierny-Mader system is the gold standard for classifying chronic osteomyelitis. Unlike traditional systems, it is not based on the etiology but rather on the anatomical extent of the bone involvement and the physiological status of the host.
Anatomical Types:
* Type 1 (Medullary): Infection is confined to the intramedullary cavity (e.g., infected intramedullary nail).
* Type 2 (Superficial): Infection is limited to the cortical surface, typically secondary to a contiguous soft-tissue defect.
* Type 3 (Localized): Full-thickness cortical sequestration with a stable osseous segment. The bone maintains structural integrity after debridement.
* Type 4 (Diffuse): Circumferential or mechanically unstable disease. Debridement requires segmental resection, leading to mechanical instability that necessitates complex reconstruction.
Host Physiological Types:
* A-Host: Normal systemic and local immune/vascular function.
* B-Host: Compromised host.
* Bs (Systemic): Malnutrition, diabetes, renal failure, immunosuppression.
* Bl (Local): Peripheral vascular disease, severe scarring, radiation fibrosis, venous stasis.
* C-Host: The morbidity of the proposed treatment outweighs the potential benefits. The disease is essentially untreatable by surgical eradication, and suppressive therapy or amputation is indicated.
Surgical Warning: Accurately staging the host is as critical as staging the bone. Attempting a massive Type 4 resection in a severely compromised C-Host is a recipe for catastrophic failure. Host optimization (glycemic control, smoking cessation, nutritional repletion) must precede elective surgical intervention.
Surgical Management: Step-by-Step Approach
The surgical management of osteomyelitis is predicated on three non-negotiable pillars: radical debridement, dead space management, and soft-tissue coverage.
Preoperative Planning and Positioning
- Imaging: Plain radiographs are mandatory but often lag behind clinical progression by 10-14 days. Magnetic Resonance Imaging (MRI) with and without contrast is the modality of choice for defining the anatomical extent of marrow edema, soft-tissue abscesses, and sinus tracts. Computed Tomography (CT) is superior for identifying sequestra and planning the osseous resection.
- Optimization: Correct anemia, optimize HbA1c (< 7.0%), and ensure adequate peripheral perfusion (ABI > 0.8 or vascular surgery consultation).
- Positioning: Position the patient on a radiolucent table to allow unhindered fluoroscopic access.
- Tourniquet Use: A pneumatic tourniquet may be applied for visualization during the initial exposure. However, it must be deflated prior to the final osseous debridement to accurately assess bone viability (the "Paprika sign").
Step 1: Surgical Approach and Soft-Tissue Debridement
- Utilize extensile incisions that incorporate and excise prior surgical scars and chronic sinus tracts.
- Elliptically excise the sinus tract down to the bone. The tract is lined with infected granulation tissue and biofilm; leaving it behind guarantees recurrence.
- Obtain multiple deep tissue cultures (minimum of 3 to 5) from distinct areas of the infected bone and soft tissue using separate, sterile instruments. Never rely on superficial swab cultures of a draining sinus, as these merely represent colonizing skin flora.
Step 2: Radical Osseous Debridement
- The goal of osseous debridement is analogous to oncologic tumor resection: all necrotic, infected, and poorly vascularized bone must be excised until healthy, bleeding bone is reached.
- Use a high-speed burr with continuous saline irrigation, osteotomes, and rongeurs to unroof the medullary canal (cortical windowing).
- Remove all sequestra and infected hardware.
- The Paprika Sign: With the tourniquet deflated, meticulously burr the cortical margins until uniform, punctate bleeding is observed from the Haversian canals. This indicates viable, vascularized bone capable of delivering systemic antibiotics and supporting a graft.
Step 3: Dead Space Management
Radical debridement inevitably leaves a cavitary defect (dead space) that will fill with hematoma—an ideal culture medium for residual bacteria. Managing this dead space is critical.
- Polymethyl Methacrylate (PMMA) Antibiotic Bead Chains:
PMMA cement mixed with heat-stable antibiotics (e.g., Vancomycin and Tobramycin) provides massive local antibiotic concentrations (elution) without systemic toxicity. The beads are strung on a non-absorbable suture or surgical wire to facilitate removal. PMMA is non-biodegradable and requires a mandatory second surgical stage for removal (usually at 4-6 weeks) and subsequent bone grafting. - Biodegradable Antibiotic Delivery Systems:
Calcium sulfate or calcium phosphate matrices can be impregnated with antibiotics. These bioceramics elute antibiotics and gradually resorb over 4 to 8 weeks, eliminating the need for a second surgery to remove the carrier. They also act as an osteoconductive scaffold. - The Masquelet Technique (Induced Membrane):
For massive segmental defects (Cierny-Mader Type 4), a PMMA spacer is placed in the defect. Over 6-8 weeks, a highly vascularized, osteoinductive pseudo-membrane forms around the spacer. In the second stage, the spacer is removed, and the membrane is packed with autologous cancellous bone graft (e.g., Reamer-Irrigator-Aspirator [RIA] graft from the femur).
Step 4: Soft-Tissue Transfer and Skeletal Stabilization
- Bone cannot heal without a robust, well-vascularized soft-tissue envelope. Local rotational muscle flaps (e.g., gastrocnemius for the proximal tibia, soleus for the middle third) or free tissue transfers (e.g., anterolateral thigh [ALT] or latissimus dorsi flaps for the distal tibia) bring a rich blood supply to the debrided bed, delivering oxygen, immune cells, and systemic antibiotics.
- Ilizarov Technique: If a massive segmental resection is performed, skeletal stability must be maintained. Circular external fixation (Ilizarov) allows for rigid stabilization while permitting distraction osteogenesis (bone transport) to regenerate the excised bone segment.
Specific Regional Considerations
Osteomyelitis of the Calcaneus
Calcaneal osteomyelitis frequently arises from contiguous spread of diabetic heel ulcers or penetrating trauma. The unique trabecular anatomy of the calcaneus allows infection to spread rapidly throughout the entire bone.
* Surgical Approach: Gaenslen’s split-heel approach or a lateral extensile approach.
* Management: Partial calcanectomy is often required. In severe cases with extensive soft-tissue loss and C-Host status, a below-knee amputation may provide the most reliable return to function.
Distal Third of the Femur
Often associated with infected total knee arthroplasty or distal femur fractures.
* Management: Requires extensive debridement, removal of implants, and placement of an articulating or static antibiotic-loaded cement spacer. Soft-tissue coverage may require a pedicled gastrocnemius flap.
Spine (Vertebral Osteomyelitis)
Typically hematogenous in origin, frequently involving the intervertebral disc (discitis) and adjacent endplates.
* Indications for Surgery: Neurological deficit (epidural abscess), spinal instability, severe kyphotic deformity, or failure of medical management.
* Management: Anterior debridement and corpectomy, followed by structural grafting (titanium cage or structural allograft) and posterior instrumented stabilization.
Postoperative Protocol and Rehabilitation
- Antimicrobial Therapy: Following surgical debridement, the patient must receive culture-directed intravenous (IV) antibiotics, typically for a duration of 4 to 6 weeks. This is managed in strict coordination with an Infectious Disease specialist.
- Monitoring: Inflammatory markers (CRP and ESR) should be tracked weekly. A steady decline indicates successful eradication, whereas a plateau or secondary spike warrants investigation for residual infection or fluid collection.
- Weight-Bearing: Weight-bearing status is dictated by the degree of osseous resection. Cierny-Mader Type 3 and 4 defects require strict non-weight-bearing until structural grafting has consolidated.
- Hyperbaric Oxygen Therapy (HBOT): May be utilized as an adjunct in refractory chronic osteomyelitis, particularly in irradiated tissues or severe diabetic vasculopathy. HBOT increases tissue oxygen tension, enhancing leukocyte oxidative killing and promoting angiogenesis.
Conclusion
The operative management of osteomyelitis demands a meticulous, uncompromising approach to surgical debridement and dead space management. The surgeon must view chronic osteomyelitis not merely as an infection, but as a complex biomechanical and biological failure of the bone-soft tissue unit. By adhering to the principles of the Cierny-Mader classification, executing radical resections to bleeding bone, utilizing modern local antibiotic delivery systems, and ensuring robust soft-tissue coverage, the orthopaedic surgeon can achieve high rates of eradication and restore functional limb salvage in even the most challenging cases.
📚 Medical References
- osteomyelitis, Clin Orthop Relat Res 286:289, 1993.
- Foster MR, Heppenstall RB, Friedenberg ZB, et al: A prospective assessment of nutritional status and complications in patients with fractures of the hip, J Orthop Trauma 4:49, 1990.
- Garre MA, Boles JM, Youinou PY: Current concepts in immune derangement due to undernutrition, J Parenter Enter Nutr 11:309, 1987.
- Gentry LO, Rodriquez GG: Oral ciprofl oxacin compared with parenteral antibiotics in the treatment of osteomyelitis, Antimicrob Agents Chemother 34:40, 1990.
- Gentry LO, Rodriquez-Gomez G: Ofl oxacin versus parenteral therapy for
