Osteomyelitis and Bite Injuries of the Hand: Comprehensive Surgical Management
Key Takeaway
Osteomyelitis of the hand frequently arises from contiguous soft-tissue infections, open fractures, or human bite injuries. Management demands aggressive surgical debridement, targeted intravenous antibiotic therapy, and early mobilization to prevent devastating stiffness. This guide details the biomechanics of clenched-fist injuries, step-by-step surgical approaches for joint exploration, and evidence-based protocols for managing acute, subacute, and chronic phalangeal and metacarpal infections.
OSTEOMYELITIS OF THE HAND
Osteomyelitis of the metacarpals and phalanges represents a formidable orthopedic challenge, often threatening the intricate biomechanical function of the hand. Unlike long bone osteomyelitis, infections in the hand rapidly compromise adjacent gliding tissues, leading to severe, often irreversible stiffness.
Etiology and Pathophysiology
The vast majority of osteomyelitis cases in the hand occur via contiguous spread rather than hematogenous seeding. Common etiologies include:
* Direct Inoculation: Open fractures, human or animal bite wounds, and penetrating trauma.
* Iatrogenic: Open reduction and internal fixation (ORIF) of closed fractures, or percutaneous pin tract infections.
* Contiguous Spread: Unrecognized or inadequately treated soft-tissue infections, such as felons, paronychia, or deep space abscesses.
* Systemic Compromise: Patients with peripheral vascular disease, diabetes mellitus, and immunodeficiency states are at a markedly increased risk due to impaired microcirculation and diminished host response.
Hematogenous osteomyelitis is exceedingly rare in the adult hand and is almost exclusively reserved for immunocompromised patients or intravenous drug users. Staphylococcus aureus remains the most commonly isolated organism across all etiologies, though polymicrobial infections are frequent in diabetic and bite-related cases.
Clinical Evaluation and Diagnostic Imaging
The principles of diagnosis mirror those of large bone osteomyelitis but require a high index of suspicion due to the subtle early presentation in the small bones of the hand.
Diagnostic measures include:
1. Plain Radiographs: Early radiographic signs (within the first 10–14 days) may only show soft tissue swelling. Periosteal reaction, focal osteopenia, and frank osteolysis are delayed findings.
2. Radionuclide Studies: In cases where plain radiographs are equivocal, advanced imaging is warranted. Technetium-99m bone scans are highly sensitive but lack specificity. Gallium-67 and Indium-111 labeled leukocyte scans provide higher specificity for active bone infection and are invaluable in differentiating cellulitis from true osteomyelitis.
3. Needle Aspiration: If imaging suggests bone infection without sequestrum formation (acute or subacute phase), fluoroscopically guided needle aspiration should be performed to obtain targeted cultures before initiating empiric antibiotics.
CLINICAL PEARL:
Infection of the distal finger pulp (a felon) may rapidly erode the distal phalanx due to the closed-compartment anatomy of the pulp space. Radiographs will demonstrate osteitis, especially if the abscess is deep and located proximally. This area of osteitis frequently regenerates after the soft-tissue abscess is adequately drained, particularly in children. It must not be confused with true sequestrating osteomyelitis, which requires aggressive bone resection.
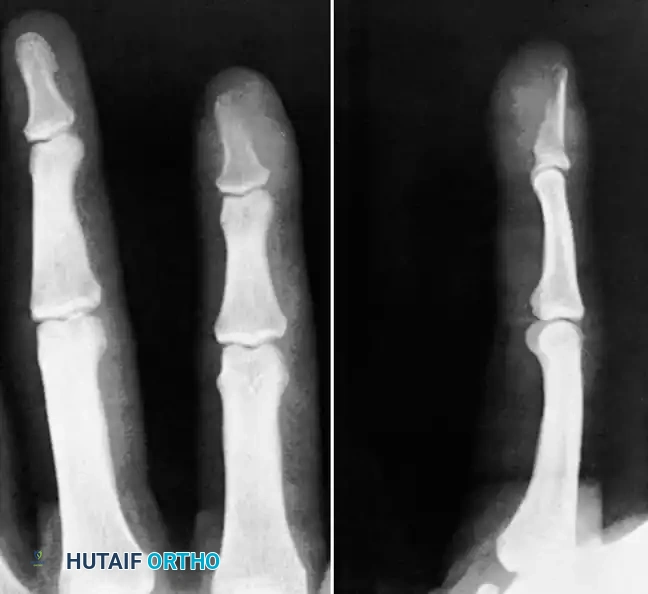
Fig. 75-14 Osteitis of distal phalanx caused by infection in finger pulp.

Fig. 75-15 Sequestrating osteomyelitis of middle phalanx.
Surgical Management of Acute and Subacute Osteomyelitis
If the infectious process is acute or subacute (lacking sequestrum formation) and an organism is successfully isolated via aspiration, the condition may resolve with targeted intravenous antibiotics without surgical drainage. However, if no organisms can be obtained, or if the patient fails to improve clinically within 24 to 48 hours, surgical intervention is mandatory.
Surgical Steps for Open Drainage:
1. Positioning and Anesthesia: The patient is positioned supine with the arm on a hand table. Regional anesthesia (axillary or supraclavicular block) is preferred to allow for postoperative vasodilation. A pneumatic tourniquet is applied but exsanguination should be performed via arm elevation rather than an Esmarch bandage to prevent proximal seeding of the infection.
2. Approach: Utilize standard mid-axial or dorsal approaches depending on the involved bone, meticulously avoiding injury to the neurovascular bundles and extensor apparatus.
3. Decompression and Debridement: Open drainage of pus and thorough debridement of all necrotic soft tissue and devitalized periosteum are performed. This ensures adequate decompression of the abscess and provides high-quality deep tissue for aerobic, anaerobic, mycobacterial, and fungal cultures.
4. Irrigation: Copious irrigation with normal saline is performed.
5. Closure: The wound is strictly left open to heal by secondary intention or prepared for delayed primary closure. Early mobilization is instituted immediately postoperatively to prevent tendon adhesions.
Management of Chronic Osteomyelitis and Salvage Procedures
If the process has lingered and sequestra (segments of necrotic bone separated from living bone) have formed, it is classified as a chronic infection.
Salvage Techniques:
Salvage of the digit is technically possible but highly complex. Procedures include:
* Diaphysectomy and Sequestrectomy: Radical resection of all dead bone until punctate bleeding (the "paprika sign") is observed.
* Dead Space Management: The resulting void is managed with antibiotic-impregnated polymethyl methacrylate (PMMA) beads or spacers (the Masquelet technique).
* Stabilization: External fixation is often required to maintain digital length and stability.
* Reconstruction: Subsequent autologous bone grafting is performed once the infection is definitively eradicated (typically 6–8 weeks later).
SURGICAL WARNING:
While salvage is anatomically possible, it is frequently difficult to preserve a functioning digit. Severe, irreversible stiffness inevitably develops not only in the involved digit but often in the adjacent, uninjured digits due to prolonged immobilization and sympathetic sympathetic responses.
Amputation Considerations:
Especially in adults, unless the infection can be rapidly controlled to preserve satisfactory function, amputation should be strongly considered. A stiff, painful, and insensate digit is a severe liability to overall hand mechanics. When indicated, amputation should be performed at the joint proximal to the involved bone to ensure clean margins and adequate soft-tissue coverage.
HUMAN BITE INJURIES
Human bite injuries to the hand are notoriously deceptive and carry a high risk of devastating complications. They generally occur in two distinct clinical scenarios:
1. Inadvertent/Accidental: Relatively innocent injuries involving nail biting, dental procedures, or accidental nicks.
2. Intentional/Violent: Includes full-thickness bites, bite amputations, and the highly morbid "clenched-fist injury" (CFI), which occurs when a patient strikes another individual's tooth with a closed fist.
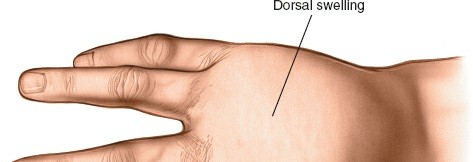
The Clenched-Fist Injury (Fight Bite)
Clenched-fist injuries account for the most severe, limb-threatening infections related to human tooth wounds. They most frequently involve the third (long) and fourth (ring) digits at the metacarpophalangeal (MCP) joint.
Biomechanics and Pathoanatomy:
The mechanism of introducing virulent anaerobic bacteria deep into the joint space is best understood through the biomechanics of the fist.
1. Inoculation Phase: The injury occurs when the hand is clenched in a tight fist (MCP joints flexed to 90 degrees). The opponent's tooth penetrates the skin, the stretched extensor tendon (sagittal band), the joint capsule, and frequently impacts the metacarpal head.
2. Entrapment Phase: When the altercation ends and the patient extends their fingers, the extensor tendon and capsule glide proximally. This shifting of tissue layers effectively seals the traumatic arthrotomy, creating a closed, anaerobic environment perfectly suited for bacterial proliferation.
PITFALL:
Patients frequently lie about the mechanism of injury due to embarrassment or legal concerns, claiming they "cut their hand on a fence." Rule of Thumb: Any small laceration over the dorsal MCP joint in a young adult must be treated as a human bite until proven otherwise.
Associated Injuries:
* Fractures: Metacarpal neck fractures (boxer's fractures) are common.
* Osteochondral Defects: The tooth frequently gouges the metacarpal head. Chondral and osteochondral fractures occur in 6% to 59% of these patients, acting as a nidus for deep joint infection.
Microbiology of Human Bites
The human mouth is teeming with virulent flora, with over 42 different bacterial species identified in normal saliva.
* Staphylococcus aureus and Streptococci (α-streptococcus being the most common single organism isolated in many series) are prevalent.
* Eikenella corrodens is a fastidious, gram-negative facultative anaerobe uniquely associated with human bites. It is notoriously resistant to first-generation cephalosporins, clindamycin, and macrolides.
* Other common isolates include Micrococcus, Clostridium, Spirochaeta, and Neisseria.
Clinical Presentation and Complications
Patients frequently delay seeking medical attention, with an average delay of 2.5 days reported in the literature. This noncompliance significantly increases morbidity. Complications range from 25% to 50% and include:
* Septic arthritis and osteomyelitis
* Tendon rupture
* Permanent joint stiffness and secondary osteoarthritis
* Digital amputation
* Systemic sepsis and, rarely, death.
Surgical Management of Clenched-Fist Injuries
Initial Evaluation:
Radiographs in multiple planes are mandatory to rule out metacarpal fractures, osteochondral shearing injuries, and retained foreign bodies (tooth fragments).
Management < 24 Hours Post-Injury (No Signs of Sepsis):
1. The wound must be formally explored under local or regional anesthesia.
2. Swabs for aerobic and anaerobic cultures (with specific requests for E. corrodens) are taken.
3. The wound is aggressively irrigated.
4. Prophylactic intravenous antibiotics are administered, and the patient is closely observed. Some surgeons advocate for mandatory hospital admission for all human bites.
Management > 24 Hours Post-Injury (or Clinical Sepsis):
Patients presenting late with erythema, swelling, purulent drainage, and pain with passive stretch require emergent operative intervention.
Surgical Technique:
1. Exposure: Under tourniquet control, the traumatic transverse laceration is extended longitudinally (creating a T-type or lazy-S incision) to allow full visualization of the extensor mechanism.
2. Joint Exploration: The MCP joint must be visualized through the traumatic rent in the extensor tendon. The joint is taken through a full range of motion to identify the exact site of capsular penetration.
3. Debridement: The wound margins are sharply debrided. The joint is inspected for osteochondral fragments, which must be excised.
4. Irrigation: The joint and soft tissues are irrigated with copious amounts of normal saline (minimum 3 liters).
5. Closure: The wound is NEVER closed. It is left open to drain and heal by secondary intention.
Postoperative Protocol and Antibiotic Therapy
- Antibiotics: Empiric intravenous therapy must cover S. aureus, Streptococci, and E. corrodens. Recommended regimens include Penicillin G, Ampicillin, Carbenicillin, or Tetracycline (specifically for E. corrodens), combined with a Cephalosporin for Staphylococcal coverage. Amoxicillin-clavulanate (Augmentin) is the oral drug of choice for step-down therapy. Antibiotics are adjusted at 36 to 48 hours based on culture sensitivities and are typically continued for 7 to 10 days.
- Tetanus: Prophylaxis is updated immediately.
- Rehabilitation: If the infection is clinically resolving, active range of motion exercises are initiated 24 to 48 hours after surgical drainage to prevent extensor tendon adhesions. Daily washing of the wound with mild soap and water provides sufficient mechanical cleansing.
- Special Populations: In diabetics or patients on corticosteroids, healing is prolonged, and the threshold for repeat surgical debridement should be extremely low.
ANIMAL BITE INJURIES
While human bites carry the highest risk of complex anaerobic infections, animal bites are significantly more common and present their own unique microbiological challenges.
Canine (Dog) Bites
Dog bites to the hand typically present as crush injuries, puncture wounds, or deep, tearing lacerations due to the immense crushing force of the canine jaw.
* Microbiology: The canine oral flora includes S. aureus, Streptococcus viridans, Bacteroides species, and Pasteurella multocida.
* Antibiotic Therapy: Most of these organisms, particularly P. multocida, are highly sensitive to Penicillin. Amoxicillin-clavulanate is the standard empiric choice.
* Surgical Management: Tetanus prophylaxis is mandatory. Deep wounds require formal surgical debridement, excision of crushed/devitalized tissue, and copious irrigation. Deep wounds should be left open for delayed primary closure or secondary intention. Superficial, clean lacerations may be loosely approximated only after exhaustive irrigation with normal saline.
Feline (Cat) Bites
Cat bites are highly deceptive. Because feline teeth are sharp and needle-like, they frequently cause deep puncture wounds that inoculate bacteria directly into joints or tendon sheaths while leaving minimal surface trauma.
* Microbiology: Pasteurella multocida is the hallmark organism, isolated in the vast majority of cat bites. Infections develop incredibly rapidly, often presenting with severe cellulitis within 12 hours of the bite.
* Antibiotic Therapy: P. multocida is exquisitely sensitive to Penicillin.
* Surgical Management: Minor, superficial scratches can be managed with aggressive cleansing and close observation. However, deep puncture wounds over joints or tendon sheaths must not be ignored. The punctures should be connected with a scalpel to open the tract, allowing for thorough debridement and high-volume irrigation. Severe wounds are left open, while superficial extensions may be loosely closed.
Treatment for exotic land, marine animal, snake, and insect bites requires specialized antivenom and infectious disease consultation, as summarized in broader toxicological literature.
You Might Also Like