Osteochondral Autograft Plug Transfer: A Masterclass in Articular Cartilage Restoration

Key Takeaway
Join us in the OR for a masterclass on osteochondral autograft plug transfer. We'll meticulously restore full-thickness articular cartilage lesions, detailing comprehensive anatomy, precise preoperative planning, and granular intraoperative execution. Learn critical techniques for graft harvest and delivery, navigate potential pitfalls, and ensure optimal patient outcomes through expert postoperative management.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the operating theater and to this definitive masterclass on articular cartilage restoration. Today, we are exploring the nuances of the osteochondral autograft transfer system (OATS), commonly referred to as the "plug" transfer. This sophisticated, joint-preserving technique is specifically designed for the treatment of focal, full-thickness articular cartilage lesions—often accompanied by associated subchondral bone loss—within a nonarthritic joint. The fundamental objective of this procedure is to restore the native topographic bone contour and the hyaline articular surface simultaneously. We achieve this by harvesting healthy, viable cartilage and its underlying subchondral bone from a lesser-weight-bearing donor site and transplanting it into the prepared defect. We are essentially moving a precise cylinder, or "plug," of living tissue, complete with its functional tidemark and subchondral bony architecture, to perfectly match a recipient socket. For larger or uniquely shaped defects, a mosaicplasty approach utilizing multiple strategically placed plugs is employed to achieve comprehensive, anatomically contoured coverage.
The pathogenesis of chondral damage is multifactorial and often traces back to specific traumatic mechanisms. A pivoting or twisting fall, significant direct axial impacts to the knee, anterior cruciate ligament (ACL) ruptures, or patellar dislocation events are classical precursors. These acute traumatic episodes generate immense shear and compressive forces that exceed the viscoelastic failure point of the articular surface, leading to focal delamination or full-thickness chondral fracturing. Osteochondritis dissecans (OCD), a distinct pathological entity involving the aseptic separation of subchondral bone and its overlying cartilage from the surrounding healthy tissue bed, is another primary indication. OCD most frequently manifests in the lateral aspect of the medial femoral condyle and requires diligent evaluation, as the viability of the separated fragment dictates whether in situ fixation or osteochondral autografting is the appropriate surgical intervention.
Clinically, isolated full-thickness chondral lesions can be surprisingly insidious, often remaining clinically silent in their initial stages. However, they must be highly suspected in the presence of traumatic hemarthrosis, particularly when associated with ligamentous disruption. As the pathology progresses, patients typically present with localized pain, often described as a persistent, deep, dull ache that exacerbates following weight-bearing activity or becomes most noticeable at night. Mechanical symptoms are prevalent; activities demanding high patellofemoral or tibiofemoral contact pressures—such as running, stair climbing, rising from a seated position, or deep squatting—provoke significant discomfort. Physical examination findings, while occasionally nonspecific, frequently reveal joint line tenderness, recurrent effusions indicative of active intra-articular inflammation, and palpable crepitus or catching.

The natural history of untreated full-thickness articular cartilage lesions is notoriously unforgiving due to the tissue's inherently limited regenerative capacity. Because articular cartilage is avascular, hypocellular, and alymphatic, it cannot mount a standard inflammatory healing response. Lesions that penetrate the subchondral bone may elicit a fibrocartilage repair response (predominantly Type I collagen), but this tissue lacks the biomechanical durability of native hyaline cartilage and inevitably degrades under physiological loading. Experimental models and longitudinal clinical studies demonstrate that severe bone bruising and associated chondral necrosis frequently precipitate early-onset osteoarthritis. While nonoperative management—including targeted physical therapy, nonsteroidal anti-inflammatory drugs (NSAIDs), intra-articular injections, and load-shifting orthotics—may provide transient symptomatic relief, these modalities do not alter the underlying structural deficit. Consequently, surgical intervention via osteochondral autografting becomes imperative for young, active patients seeking to preserve joint longevity and delay the need for arthroplasty.
Detailed Surgical Anatomy and Biomechanics
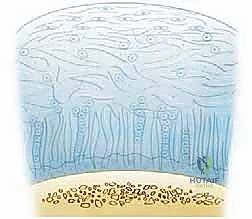
Before initiating any surgical intervention, a profound, three-dimensional understanding of articular cartilage ultrastructure and the surrounding knee anatomy is absolutely paramount. Articular cartilage is a marvel of biological engineering—a smooth, viscoelastic, hypocellular matrix primarily composed of sparsely distributed chondrocytes suspended within a vast extracellular network. This matrix is approximately 80% water and 20% organic solid, with Type II collagen accounting for 95% of the total collagen content. The collagen fibrils provide essential tensile strength and structural scaffolding, while the proteoglycan aggregates (predominantly aggrecan) create a highly hydrophilic environment. This intricate interplay allows the tissue to withstand significant, cyclical compressive loads with an astonishingly low coefficient of friction, estimated to be merely 20% of ice sliding on ice.
To appreciate the biomechanics of the osteochondral plug, we must dissect the four distinct histological zones of articular cartilage. The Superficial (Tangential) Zone comprises 10% to 20% of the total thickness and acts as the "gliding zone." Here, densely packed collagen fibers are oriented parallel to the joint surface, providing critical resistance to shear forces. The outermost layer, the lamina splendens, serves as a vital semi-permeable barrier, regulating molecular transport and protecting the deeper layers. The Middle (Transitional) Zone (40%-60% of thickness) features thicker collagen fibrils transitioning to an oblique orientation, forming the classic "arcades of Benninghoff." This zone is rich in proteoglycans and is primarily responsible for absorbing and distributing compressive loads. The Deep (Radial) Zone (30% of thickness) contains the largest collagen fibrils, oriented strictly perpendicular to the articular surface, anchoring the cartilage to the underlying bone and providing maximum resistance to compressive forces. Finally, the Calcified Zone represents the critical transition interface. The tidemark, located at the base of the deep zone, demarcates the uncalcified from the calcified cartilage. Surgically, harvesting a plug that preserves this tidemark and includes a robust cylinder of subchondral bone is non-negotiable, as it guarantees the graft's structural integrity and provides the necessary osseous foundation for creeping substitution and definitive incorporation at the recipient site.

From an osteological perspective, the femoral condyles are both the primary sites for chondral lesions and the primary reservoirs for donor grafts. The lateral aspect of the medial femoral condyle is the classic epicenter for OCD lesions. When selecting donor sites, we must meticulously target the non-weight-bearing or minimally weight-bearing portions of the articular surface to minimize donor site morbidity. The most frequently utilized donor regions include the superior and lateral margins of the lateral femoral condyle (above the linea terminalis), the medial periphery of the medial femoral condyle, and the intercondylar notch. The intercondylar notch is particularly advantageous for arthroscopic harvesting, offering excellent perpendicular access while sparing the primary articulating surfaces of the patellofemoral and tibiofemoral joints.
Navigating the muscular intervals and respecting the neurovascular bundles are critical components of a safe surgical approach. Arthroscopic techniques utilize standard anteromedial and anterolateral portals, often supplemented by accessory portals to achieve perfectly perpendicular access to the lesion—a biomechanical absolute for successful plug transfer. If an arthrotomy is mandated for massive lesions or inaccessible topography, a mini-medial or lateral parapatellar approach is employed, requiring meticulous dissection to preserve the extensor mechanism. Neurovascularly, the popliteal artery, popliteal vein, and tibial nerve lie perilously close to the posterior capsule; thus, aggressive posterior dissection or errant plunging with harvesting trephines must be strictly avoided. Medially, the saphenous nerve and its infrapatellar branch are vulnerable during portal placement and arthrotomy. Iatrogenic injury to the infrapatellar branch is a common cause of postoperative anterior knee pain and neuroma formation, underscoring the need for precise, trans-illuminated portal establishment.
Exhaustive Indications and Contraindications
Patient selection is the single most critical determinant of success in osteochondral autograft transfer. The ideal candidate is a highly active, physiologically young patient (typically under the age of 45) presenting with a symptomatic, focal, full-thickness (Outerbridge Grade III or IV) articular cartilage defect. The size of the lesion is a primary limiting factor; OATS is exceptionally effective for lesions ranging from 1.0 cm² to 2.5 cm². Defects exceeding 2.5 cm² push the limits of autograft availability, significantly increasing the risk of donor site morbidity and often necessitating alternative strategies such as osteochondral allograft transplantation or autologous chondrocyte implantation (ACI). Furthermore, the surrounding articular cartilage must be healthy and firmly attached to the underlying bone to provide a stable "shoulder" for the transplanted plug.
Concomitant intra-articular pathology must be aggressively identified and addressed either prior to or concurrently with the cartilage restoration procedure. Cartilage grafts will universally fail in a biomechanically hostile environment. Therefore, any underlying ligamentous instability (e.g., ACL deficiency) must be reconstructed. Meniscal integrity is equally vital; meniscal deficiency exponentially increases contact pressures on the articular surface, so meniscal repair or allograft transplantation should be performed if indicated. Finally, overall limb alignment is a paramount consideration. Varus or valgus malalignment that excessively loads the affected compartment will rapidly destroy the newly implanted graft. In such cases, a corrective high tibial osteotomy (HTO) or distal femoral osteotomy (DFO) must be performed concomitantly to unload the restored compartment and ensure graft survivorship.

Contraindications to osteochondral autograft transfer are absolute and must be respected to avoid catastrophic failure. Diffuse, generalized osteoarthritis or multicompartmental degenerative joint disease precludes the use of focal resurfacing techniques. "Kissing lesions"—bipolar defects on opposing articular surfaces (e.g., a femoral condyle defect directly opposing a tibial plateau defect)—are a strict contraindication, as the altered biomechanics of the graft will rapidly abrade the opposing damaged surface. Inflammatory arthropathies, such as rheumatoid arthritis, create a hostile, catabolic intra-articular environment that will inevitably degrade the graft. Additionally, active intra-articular infection, uncorrected coagulopathies, and patients with a body mass index (BMI) exceeding 35 are generally considered poor candidates due to excessive mechanical loading and altered biological healing capacities.
Indications and Contraindications Summary
| Category | Specific Criteria | Clinical Rationale |
|---|---|---|
| Primary Indications | Focal full-thickness lesions (ICRS Grade III/IV) | Restores native hyaline architecture. |
| Lesion size 1.0 cm² to 2.5 cm² | Optimizes graft availability while minimizing donor morbidity. | |
| Osteochondritis Dissecans (OCD) | Replaces necrotic bone and detached cartilage. | |
| Physiologically young, active patients (<45 years) | Higher capacity for osseous integration and rehabilitation. | |
| Absolute Contraindications | Diffuse osteoarthritis / Multicompartmental disease | Focal repair cannot overcome generalized joint failure. |
| "Kissing lesions" (Bipolar defects) | Opposing defects cause rapid mechanical degradation of the graft. | |
| Inflammatory arthropathies (e.g., Rheumatoid Arthritis) | Catabolic synovial environment destroys the graft. | |
| Uncorrected malalignment or instability | Abnormal biomechanical forces will lead to early graft failure. |
Pre-Operative Planning, Templating, and Patient Positioning
A meticulous, multi-modal diagnostic workup is the foundation of flawless preoperative planning. Standard radiographic evaluation remains the initial step and must include specific views to comprehensively assess the joint. Standing anteroposterior (AP) views in full extension allow for the assessment of gross angular deformities and joint space narrowing. The 45-degree flexion posteroanterior (PA) weight-bearing view (Rosenberg view) is absolutely critical, as it exposes subtle joint space narrowing in the posterior aspect of the condyles that is frequently missed on standard extension views. A non-weight-bearing lateral view at 45 degrees of flexion helps assess patellar height and the posterior femoral condyles. An axial view of the patellofemoral joint (Merchant or Sunrise view) is essential for evaluating patellar tracking, tilt, and trochlear dysplasia. Finally, long-leg hip-to-ankle alignment films are mandatory to accurately quantify the mechanical axis; any significant deviation into varus or valgus must be calculated for potential concurrent osteotomy.
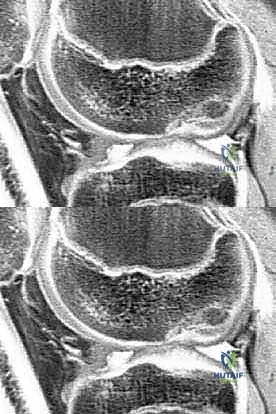
Magnetic Resonance Imaging (MRI) is the gold standard for non-invasive cartilage evaluation and surgical templating. We utilize high-resolution, cartilage-sensitive sequences, including T1-weighted gradient echo with fat suppression and fast spin-echo T2-weighted sequences. These protocols provide exquisite detail of the cartilage surface, allowing us to accurately map the surface area of the defect, assess the depth of subchondral bone involvement, and evaluate the integrity of the surrounding cartilage rim. Advanced compositional MRI techniques, such as T2 mapping and delayed gadolinium-enhanced MRI of cartilage (dGEMRIC), can quantify the biochemical composition of the cartilage (collagen orientation and proteoglycan content, respectively), helping to identify early, pre-structural degeneration in the adjacent native cartilage. Based on the MRI measurements, we rigorously template the size and number of osteochondral plugs required, mapping out the precise donor sites to ensure sufficient graft yield without compromising the donor region's structural integrity.

Patient positioning in the operating room must facilitate seamless transition between diagnostic arthroscopy, graft harvesting, and graft implantation. The patient is placed supine on the operating table. A thorough examination under anesthesia (EUA) is performed to assess ligamentous stability and range of motion, confirming preoperative clinical findings. A high-thigh tourniquet is applied to provide a bloodless field, which is critical for visualizing the tidemark and assessing subchondral bleeding during bed preparation. The operative leg is typically placed in a specialized leg holder or positioned over a post to allow for dynamic, unhindered manipulation of the knee from 0 to 120 degrees of flexion. This dynamic flexion is paramount; accessing different aspects of the femoral condyles for both harvesting and implantation requires specific degrees of knee flexion to achieve the absolute perpendicular trajectory required for the instrumentation.
Step-by-Step Surgical Approach and Fixation Technique
The surgical procedure commences with a comprehensive diagnostic arthroscopy to confirm the lesion's size, depth, and the status of the surrounding articular cartilage, as well as to address any concurrent meniscal or ligamentous pathology. Once the defect is identified, the recipient site preparation begins. Using an arthroscopic curette or a specialized ring curette, the damaged cartilage is meticulously debrided back to a healthy, stable, vertically oriented rim of native cartilage. This creates a contained "shoulder" that will secure the transplanted plug. The calcified cartilage layer at the base of the defect is removed, but aggressive penetration into the subchondral bone should be avoided at this stage to preserve the anatomical depth reference. A sizing guide is then introduced to determine the exact diameter of the required graft, ensuring the defect is fully encompassed.

Attention is then directed to the predetermined donor site, typically the superior-lateral aspect of the lateral femoral condyle or the intercondylar notch. Achieving a strictly perpendicular approach to the articular surface is the most critical technical aspect of the harvest. A tubular harvesting chisel or trephine of the corresponding size is positioned over the donor site. With a mallet, the trephine is driven into the bone to a standard depth, usually 12 to 15 millimeters. It is imperative to maintain the perpendicular trajectory to avoid creating an oblique plug, which would result in an uneven articular surface upon implantation. Once the desired depth is reached, the trephine is toggled slightly to break the cancellous bone bridge at the base, and the osteochondral plug is carefully extracted. The graft is immediately inspected to ensure the cartilage cap is intact, the tidemark is preserved, and there is sufficient subchondral bone for stable fixation.
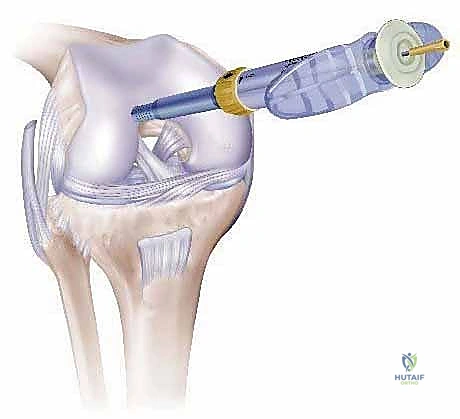
Returning to the recipient site, a recipient socket must be created to perfectly accommodate the harvested plug. A drill guide is positioned over the defect, again ensuring absolute perpendicularity to the surrounding healthy cartilage. A specialized drill or recipient chisel is used to create a socket that is precisely matched in diameter but slightly shallower (by 1-2 mm) than the length of the harvested plug. This depth mismatch is a crucial biomechanical principle; it allows for the subchondral bone of the plug to bottom out in the socket, ensuring a tight press-fit while leaving the cartilage cap perfectly flush with the surrounding native tissue. The socket is thoroughly irrigated to remove osseous debris, and a dilator may be briefly inserted to slightly expand the socket walls, facilitating smoother graft insertion.

The final phase is the delivery and seating of the osteochondral plug. The graft is introduced into the recipient socket using a specialized delivery tube or tamp. It is gently tapped into place using a mallet and a smooth-ended tamp. The surgeon must continuously monitor the orientation of the plug, ensuring that the curvature of the graft perfectly matches the anatomical contour of the condyle. The plug is seated until its articular surface is perfectly flush with the surrounding native cartilage. A graft that is left "proud" (protruding) will experience excessive shear forces and rapidly degenerate, while a "sunken" graft will fail to participate in load-bearing, leading to fibrocartilage infill and eventual failure. Once seated, the press-fit biomechanics of the bony cylinder provide immediate, robust mechanical stability, negating the need for supplemental hardware fixation. The knee is then cycled through a full range of motion under direct visualization to confirm graft stability and smooth articulation.
Complications, Incidence Rates, and Salvage Management
While osteochondral autograft transfer is a highly successful joint-preserving procedure, it is not without potential complications. A thorough understanding of these risks is essential for informed patient consent and proactive postoperative management. Donor site morbidity remains the most frequently cited concern, particularly when multiple plugs are harvested for larger mosaicplasties. Patients may experience persistent anterior knee pain, localized swelling, or crepitus originating from the harvest sites. Although the donor sockets eventually fill with fibrocartilage and cancellous bone, the altered biomechanics can be symptomatic in approximately 5% to 10% of patients. Meticulous selection of strictly non-weight-bearing donor regions and limiting the total harvested area are the primary strategies to mitigate this risk.

Graft-specific complications include subsidence, pull-out, and failure of osseous integration. Subsidence occurs when the plug sinks deeper into the recipient socket postoperatively, usually due to inadequate initial press-fit fixation, poor subchondral bone quality, or premature weight-bearing. This results in a mechanically ineffective graft and recurrent symptoms. Conversely, graft pull-out or delamination can occur if the plug was left proud or if the knee is subjected to excessive shear forces before creeping substitution has secured the bony interface. Subchondral cyst formation at the base of the graft is another recognized complication, often indicative of micromotion or synovial fluid intrusion into the osseous interface, which can compromise long-term graft survival.

When an osteochondral autograft fails, salvage management requires a careful reassessment of the joint's biological and biomechanical status. If the failure is localized and the overall joint remains well-aligned and stable, revision cartilage restoration may be attempted. Osteochondral allograft (OCA) transplantation is an excellent salvage option, particularly for larger defects resulting from graft subsidence and subsequent bone loss, as it provides mature, structural bone and viable hyaline cartilage without further donor site morbidity. Autologous Chondrocyte Implantation (ACI) or Matrix-Induced Autologous Chondrocyte Implantation (MACI) can also be considered if the subchondral bone bed can be adequately restored. However, if graft failure is accompanied by progressive, multicompartmental osteoarthritic changes or uncorrectable malalignment, joint arthroplasty (unicompartmental or total knee arthroplasty) becomes the definitive, albeit end-stage, salvage solution.
Complications and Salvage Strategies Summary
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Donor Site Morbidity | 5% - 10% | Excessive harvest volume; Harvesting from weight-bearing zones. | Conservative management; Intra-articular injections; Rarely requires surgical debridement. |
| Graft Subsidence | 3% - 8% | Inadequate press-fit; Poor bone quality; Premature weight-bearing. | Osteochondral Allograft (OCA); Bone grafting followed by MACI. |
| Graft Proudness / Delamination | 2% - 5% | Improper seating depth; Excessive shear forces. | Arthroscopic contouring (chondroplasty); Revision OCA if severely damaged. |
| Subchondral Cyst Formation | 5% - 12% | Micromotion at the bony interface; Synovial fluid intrusion. | Observation if asymptomatic; Core decompression and bone grafting if symptomatic. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation program is as critical to the success of an osteochondral autograft transfer as the surgical execution itself. The protocol must delicately balance the need to protect the healing osseous interface with the biological requirement of mechanical stimulation to maintain chondrocyte viability and prevent intra-articular adhesions. The rehabilitation is typically divided into four distinct, biologically driven phases.
Phase I: Protection and Early Motion (Weeks 0-6). The primary goals of this phase are to protect the graft from excessive compressive and shear forces while restoring baseline joint mobility. Weight-bearing status is strictly dictated by the anatomical location of the lesion. For femoral condyle lesions, patients are generally restricted to toe-touch or non-weight-bearing with crutches for the first 4 to 6 weeks to prevent graft subsidence. Conversely, for patellofemoral lesions, weight-bearing in full extension is often permitted immediately, as the patella does not engage the trochlea in extension; however, flexion under load is strictly avoided. Continuous Passive Motion (CPM) machines are frequently utilized immediately postoperatively, running for 6 to 8 hours daily, to promote synovial fluid diffusion, nourish the cartilage cap, and prevent arthrofibrosis.

Phase II: Progressive Loading and Motor Control (Weeks 6-12). As radiographic and clinical evidence of early osseous integration emerges, the focus shifts to normalizing gait and initiating muscle hypertrophy. Weight-bearing is progressively advanced to full over a 2-to-3-week period. Closed kinetic chain exercises, such as mini-squats and leg presses (initially limited to pain-free arcs of motion), are introduced to stimulate mechanotransduction within the graft and rebuild quadriceps and hamstring strength. Stationary cycling is a cornerstone of this phase, providing excellent cardiovascular conditioning and joint mobility with minimal impact loading.
Phase III: Advanced Strengthening and Proprioception (Months 3-6). During this phase, the graft's bony base is typically well-incorporated, allowing for more aggressive rehabilitation. The emphasis shifts to unilateral strengthening, dynamic neuromuscular control, and advanced proprioceptive training. Activities such as elliptical training, swimming, and progressively challenging balance exercises (e.g., BOSU ball routines) are incorporated. The physical therapist focuses on correcting any compensatory movement patterns and ensuring symmetrical lower extremity strength. Running and high-impact activities remain contraindicated during this period to protect the maturing cartilage interface.
Phase IV: Return to Sport and High-Level Activity (Months 6-12+). The final phase bridges the gap between clinical recovery and athletic performance. Progression to this phase requires a pain-free joint, full functional range of motion, and isokinetic strength testing demonstrating at least 85% to 90% symmetry compared to the contralateral limb. Sport-specific drills, agility training, and plyometrics are gradually introduced under the strict supervision of a physical therapist or athletic trainer. A full return to high-impact, pivoting sports (e.g., soccer, basketball) is rarely permitted before 9 to 12 months postoperatively, ensuring the graft has achieved maximal biological maturation and mechanical resilience.
Summary of Landmark Literature and Clinical Guidelines
The evolution and validation of osteochondral autograft transfer are deeply rooted in rigorous clinical research. The pioneering work of Dr. László Hangody in the late 1990s and early 2000s established the foundation for this technique. Hangody’s extensive, long-term prospective studies demonstrated excellent clinical outcomes and high rates of return to sport, particularly for focal lesions of the femoral condyles. His 10-year follow-up data provided compelling
